
Abstract
Background:
In 1976, Hawk and Hazard described the tall cell variant (TCV) of papillary thyroid carcinoma (PTC). While the lesions they described had cytologic features of papillary carcinoma, they showed more aggressive behavior with a greater propensity for extrathyroid extension and lymphovascular invasion than classic PTC. In 1991, Bronner and LiVolsi described a series of patients with TCV that progressed to spindle cell squamous carcinoma (SCSC), a unique form of anaplastic thyroid carcinoma. This study describes the variable clinical and pathologic presentations in 31 patients with anaplastic SCSC arising in association with TCV.
Methods:
The surgical pathology archives as well as the personal consultation files of one of the authors (V.A.L.) were reviewed to retrieve cases of SCSC arising in association with TCV. The available clinical as well as pathologic information on all patients was reviewed.
Results:
A total of 31 patients with SCSC arising in association with TCV were retrieved from our files. The average age at primary presentation was 67 (range 32–92) with a female-to-male ratio of 2:1. Three clinical scenarios for SCSC associated with TCV were identified. These were type I, consisting of TCV with SCSC at the time of presentation (18 patients); type II, consisting of SCSC arising as a recurrence in patients with a known history of TCV (5 patients); and type III, consisting of SCSC presenting as a primary laryngeal squamous cell carcinoma in a patient with or without a known history of TCV (8 patients). The type III cases were of most concern since they often were confused with primary laryngeal squamous cell carcinoma and most often were diagnosed after laryngectomy.
Conclusions:
SCSC of the thyroid is almost exclusively associated with TCV and can have variable clinical presentations. SCSC is most commonly seen associated with a primary diagnosis of TCV. SCSC may be seen, however, in patients with recurrent PTC and most importantly may present in a fashion similar to primary laryngeal SCSC. Therefore, caution should be exercised in evaluating laryngeal squamous lesions in patients with known history of TCV and without known risks factors for head and neck carcinogenesis.
Introduction
In addition, Bronner and LiVolsi and others have noted that some cases of TCV progress to spindle cell squamous carcinoma (SCSC), an unusual form of anaplastic carcinoma, with both spindle cell elements and squamous islands with focal keratinization (4,5). We now describe the variable clinical and pathologic presentations of 31 patients with SCSC arising in association with TCV. In the most common clinical scenario (type I), both TCV and SCSC components are present in the initial resection. In the second scenario (type II), SCSC arises as a recurrence in a patient with a known history of TCV. In the third clinical presentation, SCSC presents as a mimic of primary laryngeal squamous cell carcinoma in a patient who may or may not have a known history of TCV. These data indicate that a diagnosis of TCV is clinically relevant for pathologic evaluation of both the initial resection and recurrences, which may contain anaplastic SCSC. This is an important consideration in the differential diagnosis because SCSC may occur as a primary tumor in the oropharyngeal region. Further, patients with a history of TCV PTC who present with a presumed primary laryngeal squamous cell carcinoma should be evaluated for the possibility of a recurrence of TCV with transformation to SCSC, particularly if the patient does not have other risk factors for head and neck carcinogenesis.
Materials and Methods
This study was approved by the University of Pennsylvania Institutional Review Board. The cases were selected from the Surgical Pathology files from the Hospital of the University of Pennsylvania (20 cases) and the consultation files of one of the authors (V.A.L.; 11 cases). Clinical information was obtained through chart review, and the available pathologic history was reviewed for each case. Hematoxylin and eosin-stained sections were reviewed. In some of the type II and type III cases, the histology of the primary tumor and a few of the recurrences (type II cases only; see below) were not available for review since many of these specimens were at other institutions and from several years ago. In some of the cases, immunostains were available; these stains included cytokeratins, thyroid transcription factor 1 (TTF-1), and thyroglobulin.
Results
In all cases, the tall cell papillary component displayed long, well-formed papillae with fibrovascular cores lined by tall columnar cells with pink cytoplasm, in which the cell height was two to three times the cell width (Fig. 1A). In addition, the cells had typical nuclei of papillary carcinoma, with enlarged oval and overlapping nuclei showing central clearing and ground glass chromatin. Nuclear grooves and multiple intranuclear inclusions, which give rise to the characteristic “soap bubble” intranuclear inclusions characteristic of TCV on cytologic preparations (6), were also observed. The SCSC anaplastic component showed spindle cells as well as solid nests and infiltrating islands of moderately differentiated squamous cell carcinoma, some of which had bland cytology (Fig. 1B). Other areas showed anaplastic spindle cells with a high nuclear:cytoplasmic ratio, pleomorphic, hyperchromatic nuclei with irregular contours, and prominent nucleoli.

(
The clinical and pathologic findings are summarized in Tables 1 –3. The average age at presentation was 67 (range 32–92) with a female-to-male ratio of 2:1. Patients found to have SCSC associated with TCV presented in three clinical and pathologic scenarios. Clinically, the majority of patients simply presented with a thyroid mass (18 patients); histologically, these cases were characterized by a mixture of TCV PTC and SCSC present concurrently in the thyroidectomy specimen (type I). Both tumor morphologies were intimately admixed, with areas of transition from TCV PTC to the spindled and squamous appearance of the anaplastic component. The transition zone was notable for areas of hemorrhage, and the squamous cells, some of which appear bland, merge with more hyperchromatic, pleomorphic nuclei of the anaplastic squamous and spindled cells. Extrathyroidal extension and lymphovascular invasion were seen in 14 and 8 (14/18 and 8/18), respectively, of the type I cases.
SCSC, spindle cell squamous carcinoma; TCV, tall cell variant; PTC, papillary thyroid carcinoma; LVI, lymphovascular invasion; PNI, perineural invasion.
The tumors in the second group of cases (5 patients; type II) initially demonstrated TCV PTC in the thyroid resection, but the anaplastic SCSC developed only in recurrences or metastases, months to years later. In both cases 7 and 9 (Table 2), the transformation to SCSC occurred longer than 15 years after the diagnosis of TCV. The site of recurrence with SCSC transformation was most often in neck lymph nodes. Excision of these enlarged lymph nodes demonstrated metastatic TCV PTC with solid squamoid nests and pleomorphic spindled areas, consistent with SCSC transformation. In addition to anaplastic transformation in neck lymph nodes, one patient also had spindle-cell anaplastic carcinoma in an endobronchial mass (Case 28, Table 2). Metastatic TCV PTC in multiple pulmonary nodules was noted in another case; however, SCSC transformation was not seen in the lung wedge resection (Case 9, Table 2).
In the third clinical scenario (type III), eight patients presented with a laryngeal mass (Fig. 2), and in four cases had a biopsy showing invasive squamous cell carcinoma before laryngectomy. The smoking history was only available for two of these patients (Cases 15 and 29). Whereas one of the patients (Case 15) had a 20 pack-year smoking history at the time of presentation with the laryngeal mass, the other patient (Case 29) was a life-long nonsmoker and had no obvious risk factors for head and neck carcinogenesis. Five of the eight patients had a prior history of PTC, and three of these five patients were known to have had TCV. In all cases, however, evaluation of the laryngectomy specimen revealed anaplastic SCSC arising in association with TCV PTC. The lack of an associated in situ squamous carcinoma or dysplasia in the laryngeal mucosa argued against a primary laryngeal squamous cell carcinoma in these cases. In addition, the intimate association of the TCV and SCSC components, with transitions between PTC to SCSC, strongly suggests that both morphologies are components of one tumor, rather than from the collision of two tumors. Although not routinely available before 2000, TTF-1 immunoreactivity is also helpful for distinguishing between these possibilities. The expression of TTF-1 by the squamous anaplastic component is strong evidence that the squamous cells are derived from follicular cells (Fig. 3) and are less likely to represent a concurrent or metastatic squamous carcinoma colliding with PTC.

Gross photograph of laryngectomy specimen from Case 17, bisected to reveal a poorly circumscribed solid tumor mass involving the infraglottic space.
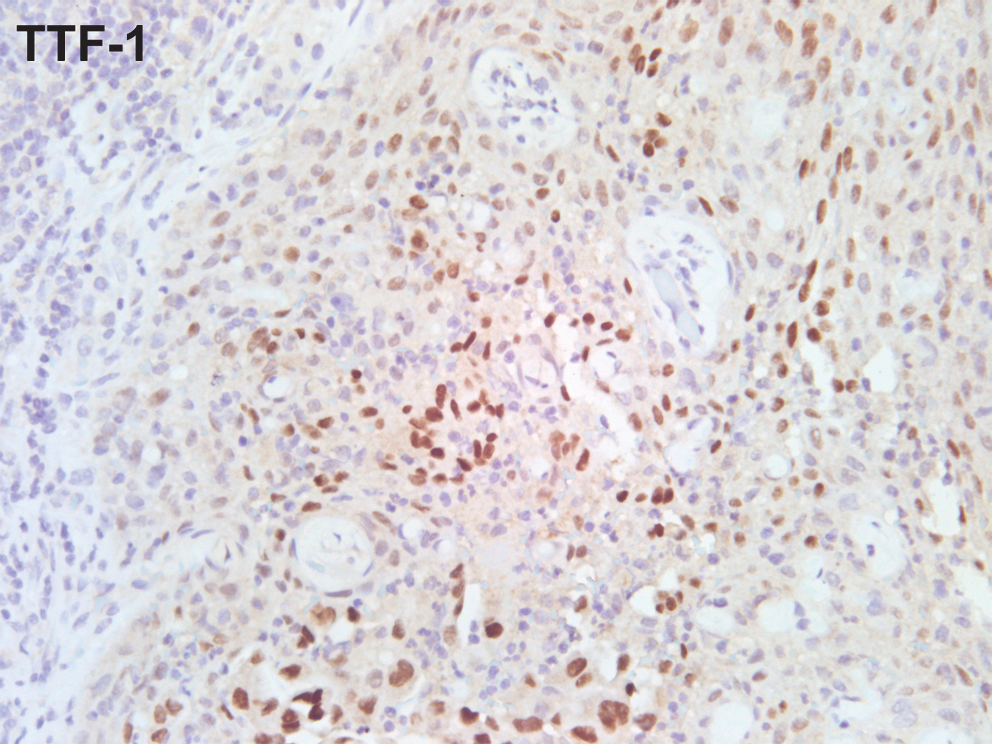
TTF-1 immunostaining of the squamous anaplastic component strongly supports the thyroid follicular origin of these cells, rather than a concurrent primary squamous carcinoma of the larynx (collision tumor). TTF-1, thyroid transcription factor 1.
Discussion
TCV of PTC, first described in 1976, is distinguished from other types of PTC by its tall columnar cell shape, with a height:width ratio of 2–3:1, and abundant eosinophilic or oxyphilic cytoplasm (1,2). The accurate classification of TCV is clinically relevant, since these tumors tend to behave more aggressively (7,8), and TCV may transform to SCSC anaplastic carcinoma (4,5). We now describe the variable clinical presentations of 31 patients with anaplastic SCSC arising from TCV PTC and the clinical and pathologic considerations for diagnosis of these unusual tumors. Based on histologic examination, each case was classified into one of three clinical presentations: type I, in which TCV and SCSC are both identified in the initial resection (18 patients); type II, in which SCSC arises as a recurrence/metastasis in patients with a known history of TCV (5 patients); and type III, in which SCSC presents as a primary laryngeal squamous cell carcinoma in a patient with or without a known history of TCV (8 patients).
Most commonly, patients with SCSC arising from TCV present with both tumor morphologies in close apposition in the initial thyroid resection specimen (type I) and present with a clinical thyroid mass. In contrast, the type II cases had a history of TCV or prior thyroidectomy with TCV PTC; months to years later, however, these patients presented with recurrences, most often in cervical lymph nodes, that showed metastatic TCV with dedifferentiation and transformation to SCSC. In both the type I and II cases, the histology demonstrates areas of transition from the well differentiated tall cell morphology, to more poorly differentiated, and spindle and squamous anaplastic morphology, and this intimate relationship leaves little diagnostic question that the SCSC arose in association with TCV PTC.
The type III cases presented very differently, with a laryngeal mass; four of eight patients had a biopsy diagnosed as invasive squamous cell carcinoma or poorly differentiated malignant neoplasm. These patients were presumed clinically to have a primary laryngeal squamous cell carcinoma. Only five of these patients had a history of PTC (three of who were found to have TCV PTC). In these cases, the clinical presentation of a laryngeal mass and the length of time (ranging from 2 to 15 years) from the apparently cured PTC led to the assumption that the new mass was a primary squamous carcinoma of the larynx. Hence, all type III patients underwent layrngectomy. However, histologic evaluation of the laryngectomy specimens showed anaplastic SCSC admixed with areas of TCV of papillary carcinoma.
The differential diagnosis includes a collision of a primary laryngeal SCSC with a recurrent PTC, or SCSC arising in association with TCV PTC. In all cases, the lack of an associated in situ squamous carcinoma or dysplasia argues against a primary laryngeal squamous cell carcinoma. In addition, the intimate association of the TCV and SCSC components, with transitions between TCV PTC to SCSC, strongly suggests that both components arose from one tumor, rather than from the collision of two tumors. TTF-1 positivity in the SCSC component in more recently diagnosed cases helps determine the primary origin of these tumors from the pre-existing TCV. (TTF-1 immunohistochemistry was not performed in all cases, as tissue blocks were not always available [consult cases], and in cases before 2000, TTF-1 immunostaining was not routinely available.)
TTF-1 reactivity in the SCSC component does support a thyroid origin but may also be seen in other primary squamous tumors, such as lung (9,10). In addition, thyroglobulin is negative, except at the tumor edge due to diffusion artifact. Immunohistochemistry for other markers may not be helpful in distinguishing between a primary laryngeal squamous cell carcinoma and SCSC. The squamous components of SCSC are usually positive for low- and high-molecular-weight cytokeratins, and the spindle cells are weakly and variably positive for low-molecular-weight cytokeratins and cytokeratins 903/904 (4). In the future, molecular techniques such as differential microRNA profiles between primary laryngeal squamous carcinoma and anaplastic SCSC may help distinguish between these tumors (11 –13).
Bronner and LiVolsi suggested the association of these two unusual tumors may represent an interesting histopathologic link in the pathology of the thyroid (4). Although several authors subsequently have proposed a step-wise progression from well-differentiated papillary carcinoma to poorly differentiated carcinoma, or to anaplastic carcinoma, the pathogenesis of this dedifferentiation is poorly understood (14 –16). The RAS mutations have been implicated in the progression of papillary carcinoma to poorly differentiated carcinoma (16). Recent studies have shown that BRAF is mutated at codon 599 in 40% or more of PTCs (17 –19). BRAF mutations may be enriched in TCV PTC; one study demonstrated that all six TCV PTC cases harbored the BRAF mutation (20). In addition, anaplastic carcinomas (two of three cases, and three of nine cases) with adjacent TCV PTC also tested positive for the BRAF mutation (20,21). However, BRAF mutations are seen at all stages of PTC, including papillary microcarcinomas, indicating that additional mutations must take place for dedifferentiation to occur. Acquisition of p53 mutations may be one such event in the progression of BRAF-mutated papillary carcinomas to anaplastic carcinoma (19).
In summary, patients found to have SCSC anaplastic carcinoma arising from TCV of PTC may present in various clinical scenarios. The clinical history of TCV is very important, especially when patients present with recurrences or metastases that have dedifferentiation of the primary tumor. If a patient with a history of TCV presents with a laryngeal mass, clinicians and pathologists should consider SCSC arising from TCV PTC in the differential diagnosis, particularly if the patient does not have a smoking history or other risk factors for head and neck carcinogenesis.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.