
Abstract
Background:
Papillary thyroid carcinoma (PTC) is the most frequent carcinoma of the thyroid gland and has a relatively good prognosis. However, it is important to identify PTC characteristics that indicate high risk for recurrence and metastasis. To date, overexpression of the membrane mucin, MUC1, has been investigated as a key molecular event in the pathogenesis of aggressive PTC. However, other membrane-associated mucins, matrix metalloproteinase-13 (MMP-13) and tissue inhibitor of metalloproteinase-13 (TIMP-3), have not been studied yet. The aim of this study was to evaluate the expression levels of MUC4, MUC15, MMP-13, and TIMP-3 and their prognostic significance in PTC.
Methods:
We analyzed MUC4, MUC15, MMP-13, and TIMP-3 expression in 10 PTC and 10 normal thyroid tissue samples using real-time reverse transcription–polymerase chain reaction. Tissue array blocks were obtained from 98 PTC cases. Tumor regions and nontumor regions were analyzed in tissue array blocks and immunohistochemistry studies were conducted using sectioned slides. Semiquantitative scores were correlated with clinicopathological factors of 98 PTC patients.
Results:
MUC4- and MUC15-specific mRNA was increased by 78-fold and 4.75-fold, respectively, in PTC samples compared with normal thyroid tissues. MMP-13 and TIMP-3 gene expression levels were decreased by approximately 0.39-fold and 0.53-fold, respectively. By immunohistochemistry, MUC4 and MUC15 expression levels were increased in PTC samples compared with normal thyroid tissues (p < 0.001). MMP-13 and TIMP-3 expression levels were decreased in PTC samples compared with normal thyroid tissues (p < 0.001). High MUC4 scores were significantly correlated with small tumor size and papillary thyroid microcarcinoma subtype. High MUC15 scores were significantly correlated with age (≥45 years), distant metastasis, and multifocality.
Conclusions:
MUC4 and MUC15 were overexpressed in PTC, and high MUC15 expression was associated with high malignant potential. MUC15 may serve as a prognostic marker and potential novel therapeutic target in PTC.
Introduction
Mucins comprise a heterogeneous family of high-molecular-weight glycoproteins characterized by extensively O-glycosylated tandem repeats rich in serine and threonine. To date, at least 20 mucin genes have been reported and are designated chronologically in order of discovery (1 –3). Complete or partial sequencing of mucin genes has led to classifying mucins as gel-forming mucins (MUC2, MUC5AC, MUC5B, MUC6, and MUC19), soluble mucins (MUC7 and MUC9), or membrane-associated mucins (MUC1, MUC3A, MUC3B, MUC4, MUC12, MUC13, MUC14, MUC15, MUC16, MUC17, and MUC20), with MUC8 and MUC11 remaining unclassified (4). These unique glycoproteins are typical of epithelial cells and are believed to exert a primary protective function in epithelial and mesothelial tissue linings. This protective function may, however, also be exploited by tumor cells to defend against immunological attack (5 –7). MUC1 has been proposed as a key molecule in TC pathogenesis (8 –12). However, other membrane-associated mucins such as MUC4 or MUC15 have been rarely investigated in PTC.
MUC1 overexpression facilitates faster Met turnover. Phosphorylation of the MUC1 cytoplasmic tail by Met enhanced its interaction with p53, suppressing the AP1 transcription factor from interacting with the MMP1 promoter, ultimately reducing MMP1 transcription (13). Therefore, we included matrix metalloproteinases (MMPs) and their inhibitor, tissue inhibitor of metalloproteinase (TIMP), as candidate genes in this study.
MMPs are enzymes that play a role in tumor development by promoting various events, including degradation of extracellular matrix (14). There are various types of MMPs such as collagenases, gelatinases, stromelysins, matrilysin, and membrane-bound MMPs that are categorized based on substrate specificity (14). The expression levels and activities of MMP-2 and MMP-9, and their inhibitors, TIMP-1 and TIMP-2, have been shown to increase in PTC tumor cells (15). MMP-7 and MMP-11 may be inversely linked to aggressive PTC characteristics (16). However, MMP-13 and TIMP-3 have not been investigated in PTC.
The aim of this study was to investigate the expression levels of the membrane mucins, MUC 4 and MUC15, and MMP-13 and TIMP-3, which regulates MMP-13 (17 –19), in PTC, and to examine clinicopathological correlations such as invasive and metastatic characteristics.
Materials and Methods
Case selection and tissue sample preparation
Tumor specimens were obtained from 10 PTC patients who underwent total thyroidectomy in the Department of Surgery, Severance Hospital, Yonsei University College of Medicine, Seoul, Korea. The specimens were prepared for real-time reverse transcription–polymerase chain reaction (RT-PCR). Ten normal thyroid tissues were obtained from each contra-lateral lobe of PTC patients exhibiting apparently normal morphology as a control. Both tumor and normal specimens were stored at −70°C for RT-PCR.
Tissues for immunohistochemistry were randomly selected from 98 PTC patients who underwent surgery in the same department between 2007 and 2008. Ninety eight normal thyroid tissues were obtained from each contra-lateral lobe of PTC patients exhibiting apparently normal morphology as a control. These patients included 18 males and 80 females, and the average age was 43.4 years. After surgical resection, the specimens were fixed with 10% formalin. A tissue array block was made using tissues from these 98 patients, and an immunohistochemical study was conducted using sectioned slides from the tissue array block. The study protocol was approved by the institutional review board of the hospital.
Real-time quantitative PCR
MUC4, MUC15, MMP-13, and TIMP-3 expression levels were analyzed by RT-PCR. Total RNA from tissues was isolated using TRIzol reagent, and 3 μg of total RNA was used to synthesize cDNA (SuperScript III Reverse Transcriptase; Invitrogen, Camarillo, CA), according to the manufacturers' protocols. Residual genomic DNA was eliminated by DNase I digestion. Real-time PCR amplification for MUC4 was performed in the presence of double-labeled fluorogenic probe for MUC4 TaqMan probes; Applied Biosystems, Foster City, CA). A SYBR-Green real-time PCR method was used to detect MUC15, MMP-13, and TIMP-3 amplification using 200Nm primer. Primers specific for MUC15 (forward: CAACAACAGCCACGGAATAA; reverse: GGCTTGTGGAAATGGTAGATG), MMP-13 (forward: TGGTCCAGGAGATGAAGACC; reverse: TCCTCGGAGACTGGTAATGG), and TIMP-3 (forward: ACCTGCCTTGCTTTGTGACT; reverse: GGCGTAGTGTTTGGACTGGT) were designed using Primer Express Software (Applied Biosystems) to produce 97-, 97-, and 95-bp fragments, respectively. Their specificities were confirmed by BLASTIN (
Tissue microarray and immunohistochemistry
To construct the tissue array block, sections of PTC tissue cores were stained with hematoxylin and eosin to identify areas of tumorous and normal tissue. Once the areas of interest had been identified, the recipient tissue array block was constructed using manual tissue array equipment (Quick-Ray; UNITMA, Seoul, Korea). We placed 2-mm cores in the recipient block, heated the block to fix the samples into the block, and applied a paraffin layer to ensure proper facing. To facilitate blind grading, an Excel spreadsheet (Microsoft Corporation, Redmond, WA) was constructed using sample accession numbers but without information regarding the final pathological finding.
Sectioned slides were deparaffinized three times in xylene for 20 minutes each and rehydrated using a graded alcohol solution. Antigen retrieval was performed in 10 mM citrate buffer at pH 6.0 for 10 minutes in a microwave. Slides were allowed to cool to room temperature and sequentially rinsed three times in phosphate-buffered saline and 50 mM Tris-HCl (pH 7.6), 150 mM NaCl, and Tween 20 (0.025%; TBS-T) for 2 minutes each. Endogenous peroxidase activity was quenched by incubating in peroxidase-blocking reagent (code S2001; DakoCytomation, Carpinteria, CA). Each incubation step was carried out at room temperature, followed by three sequential washes of TBS-T for 5 minutes each. Sections were incubated in primary antibody diluted in 10% serum (goat serum; Jackson ImmunoResearch Laboratories, West Grove, PA; rabbit and horse serum, Vector Laboratories, Burlingame, CA). The secondary antibody was diluted in antibody diluent (DakoCytomation) and incubated with a biotinylated secondary antibody for 30 minutes, peroxidase-labeled streptavidin for 20 minutes (LSAB-2; DakoCytomation), and diaminobenzidine chromogen substrate (DakoCytomation) for 5 minutes. Slides were counterstained with hematoxylin, dehydrated in a graded alcohol solution, and mounted. The negative controls were incubated with nonimmune immunoglobulin G of the primary antibody host.
The following antibodies were used in our study: mouse monoclonal MUC4 (1:100, Invitrogen); rabbit polyclonal MUC15 (1:50; Santa Cruz Biotechnology, Santa Cruz, CA); mouse monoclonal MMP-13 (1:50; Santa Cruz Biotechnology); and mouse monoclonal TIMP3 (1:50; Santa Cruz Biotechnology).
Immunohistological scores and clinicopathological parameters
A surgical pathologist, blind to the identity of the specimens, examined the percent positivity and intensity of immunostained slides and scored them as previously reported (15,21,22). As shown in Table 1, the percent positivity was the number of cells showing positive stain (grade 0, 0%; grade 1, 1%–33%; grade 2, 34%–66%; and grade 3, 67%–100%, respectively). The intensity grade 0 was defined as no immunoreaction, grade 1 as weak immunoreaction, grade 2 as moderate immunoreaction, and grade 3 as strong immunoreaction, respectively. The total scores in PTC (tumor score) and normal thyroid tissues (nontumor score) were determined as the sum of the positivity and intensity grades.
Based on the clinical and pathologic records, a retrospective analysis was performed on the following variables: age, gender, tumor size, subtype (papillary thyroid microcarcinoma [PTMC], PTC), lymph node metastasis, extra-capsular invasion, multifocality, distant metastasis, and clinical stage. Clinical stage was determined according to the pathological TNM system (23). Immunohistochemical results were correlated with the clinicopathological parameters to evaluate the prognostic significance.
Statistical analysis
Scores were expressed as the mean ± standard deviation. Statistical analysis was performed using SPSS statistical software (version 13.0; SPSS, Chicago, IL). The Mann–Whitney U-test was used to compare the expression levels of each gene by real-time PCR between PTC and normal tissue. The independent-samples T test was used to compare average scores of tumor markers using immunohistochemistry and clinicopathological variables. The numbers of positive immunoreactivities (tumor score >0) in PTC and normal thyroid tissues were evaluated using the chi-square test. A p-value <0.05 was accepted as a significant difference.
Results
Expression levels of MUC4, MUC15, MMP-13, and TIMP-3 RNAs in PTC and normal thyroid tissues
To compare gene expression in PTC and normal thyroid tissues, MUC4, MUC15, MMP-13, and TIMP-3 mRNA expression was analyzed by real-time RT-PCR. As shown in Figure 1, MUC4 mRNA increased approximately 78-fold and MUC15 approximately 4.75-fold in PTC compared with normal thyroid tissues. These findings demonstrate that PTC upregulated expression of membrane mucins, MUC4 and MUC15, at the transcription level. MMP-13 and TIMP-3 gene expression decreased by approximately 0.39-fold and 0.53-fold, respectively, in PTC compared with normal thyroid tissue (Fig. 1). These findings indicate that MMP-13 (collagenase) and TIMP-3 (MMP-13 inhibitor) expression levels were downregulated in PTC at transcription level.
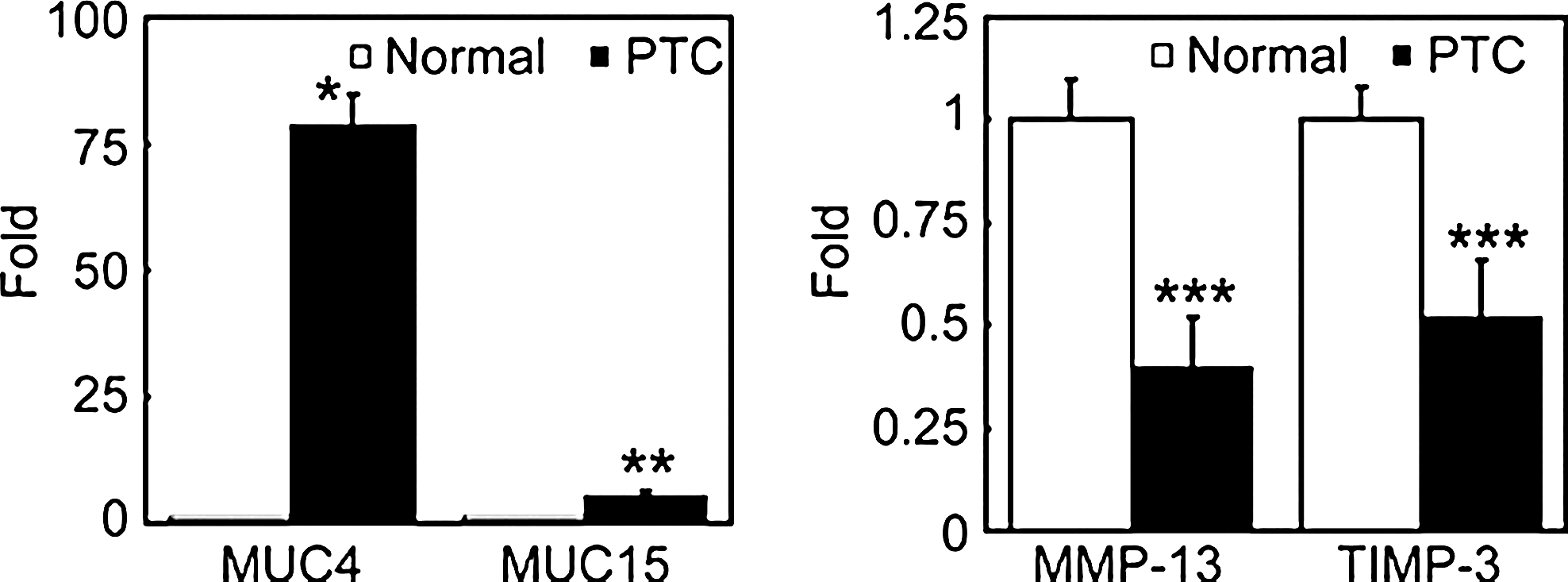
Real-time reverse transcription–polymerase chain reaction assay of relative MUC4, MUC15, MMP-13, and TIMP-3 mRNA levels in PTC and normal thyroid tissues. Data were normalized to the expression of the housekeeping gene glyceraldehyde-3-phosphate dehydrogenase. The y-axis shows an increase in specific mRNA over unstimulated samples. Data represent the mean ± standard deviation from triplicate experiments; *p < 0.001, **p < 0.01, ***p < 0.05 compared with normal. PTC, papillary thyroid carcinoma.
Immunohistochemical expression in PTC and normal thyroid tissues
To investigate differences in MUC4, MUC15, MMP-13, and TIMP-3 protein expression between PTC and normal thyroid tissues, tissue-microarrays were constructed. Representative pictures of MUC4, MUC15, MMP-13, and TIMP-3 expression are presented in Figure 2.
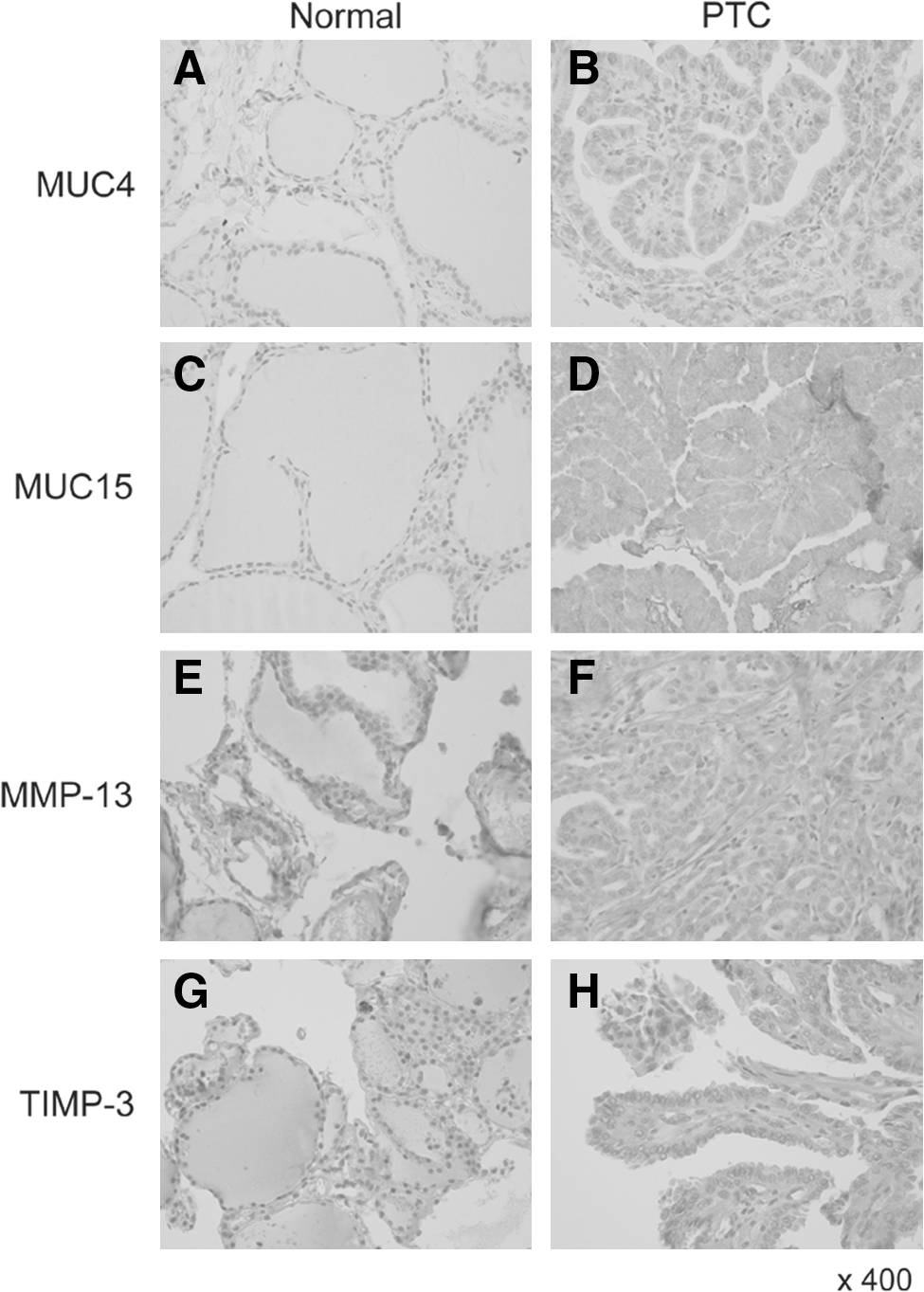
Immunohistochemical analysis of MUC4, MUC15, MMP-13, and TIMP-3 expression in PTC and normal thyroid tissues. MUC4
In tumor regions, positive immunoreactivities (tumor score >0) were present in 78 of 98 cases (80%) for MUC4, 97 of 98 (99%) for MUC15, 7 of 98 (7%) for MMP-13, and 8 of 98 (8%) for TIMP-3. In nontumor regions, positive immunoreactivities (nontumor score >0) were present in 10 of 98 cases (10%) for MUC4, 74 of 98 (75%) for MUC15, 48 of 98 (49%) for MMP-13, and 24 of 98 (25%) for TIMP-3 (Table 2).
The immunohistochemical scores in PTC and normal thyroid tissues were determined as the sum of the positivity and intensity grades. The percent positivity was scored from 0 to 4 (grade 0, 0%; grade 1, 1%–33%; grade 2, 34%–66%; grade 3, 67%–100%). The intensity grade was scored from 0 to 4 (grade 0, no immunoreactions; grade 1, weak immunoreactions; grade 2, moderate immunoreactions; grade 3, strong immunoreactions).
PTC, papillary thyroid carcinoma.
MUC4 and MUC15 protein expression levels were increased in tumor regions compared with nontumor regions (p < 0.001). MMP-13 and TIMP-3 protein expression decreased in tumor regions compared with nontumor regions (p < 0.001). MUC4, MUC15, MMP-13, and TIMP-3 protein expression corresponded to gene expression levels (Table 3).
Positive immunoreactivity was defined as the immunohistochemical score >0 in tumor and nontumor regions, respectively.
Correlations between immunohistochemical tumor scores and clinicopathological parameters
The correlations between MUC4 and MUC15 scores and clinicopathological data are shown in Table 4. MUC4 high scores significantly correlated with small tumor size, and PTMC subtype. MUC15 high scores significantly correlated with age (≥45 years), presence of distant metastasis, and presence of multifocality. Correlations between MMP-13 and TIMP-3 and clinicopathological data were not analyzed because there were too few positive immunoreactivities in tumor region.
Tumor scores were determined as the sum of the positivity and intensity grades in tumor region.
NS, not significant; PTMC, papillary thyroid microcarcinoma; LN, lymph node; ECI, extracapsular invasion.
Discussion
PTC accounts for 80% of thyroid malignancy and is characterized by slow growth and an excellent prognosis (24). However, 10%–15% of cases exhibit aggressive behavior with hallmarks of local invasion, distant metastasis, treatment resistance, and mortality (25). Although several clinicopathological variables have been identified to assess the malignant potential of individual tumors at presentation, none consistently identify patients at risk for poor outcomes. Molecular factors underlying aggressive PTC behavior may more accurately predict outcomes and potential therapeutic targets.
Membrane-associated mucins such as MUC1, MUC4, and MUC15 lubricate epithelial cell surfaces, prevent tissue hydration, and constitute a barrier against infection (26). They may serve as cell surface receptors and sensors and conduct signals in response to external stimuli, leading to coordinated cellular responses such as proliferation, differentiation, apoptosis, or secretion of specialized cellular products (27). Cancer cells might use mucins in much the same way, as protection from adverse growth conditions and to control the local environment during invasion and metastasis.
To date, MUC1 overexpression has been thoroughly investigated as a key molecular event in the pathogenesis of aggressive PTC (9,10). MUC4 has also been suggested as a tumor biomarker (28 –30). It can serve as a ligand of the receptor tyrosine kinase ErbB2 and modulate apoptosis via multiple mechanisms (28). MUC4 mRNA and protein expression has been shown to be weak and insignificant in thyroid tissues, though the study was limited by small sample size (15 PTC and 22 normal thyroid tissues) (12). In our study of 98 patients, MUC4 gene expression increased by approximately 78-fold in PTC, and MUC4 protein staining scores also significantly increased in PTC compared with normal thyroid tissue. Differences in PCR methods and antibodies may explain these differences. High MUC4 expression was associated with small tumor size and PTMC subtype. MUC4 may play an important role in early oncogenesis of papillary thyroid cancer.
Our data are first demonstration of MUC15 protein expression in the thyroid gland, although previous studies have shown abundant MUC15 gene expression in the thyroid gland (31,32). MUC15 is upregulated in colorectal tumors and its expression enhances the oncogenic potential of colon cancer cells (33). In our study, MUC15 gene expression increased by 4.75-fold in PTC, and MUC15 protein staining scores also significantly increased in PTC compared with normal thyroid tissue. Of the 98 tissues, 89% scored 5–6 points in tumor regions but only 3% scored 5–6 points in nontumor regions. High MUC15 expression in tumor cells was associated with old age, the presence of distant metastasis, and multifocality. These findings implicate that MUC15 overexpression is associated with aggressive PTC behavior.
MMP and TIMP protein expression have been reported frequently, first by Campo et al., in TC. MMP-2 protein overexpression is associated with tumor invasion and metastasis in TC (34). MMP-2, MMP-9, TIMP-1, and TIMP-3 proteins and activities are increased in PTC tumor cells, and they play an important role in PTC invasion and metastasis (15). In contrast to other MMPs, overexpression of MMP-7 and MMP-11 is inversely linked to aggressive PTC characteristics, and their downregulation may indicate poor prognosis (16). Our study is the first to examine MMP-13 and TIMP-3 expression levels in PTC. MMP-13 and TIMP-3 expression levels were downregulated in tumor cells compared with nontumor thyroid cells. In other tumors such as breast cancer, squamous cell carcinoma of head and neck, and malignant melanoma, MMP-13 was over-expressed in tumor cells, and high expression was associated with aggressiveness and poor prognosis. The physiologic significance of MMP-13 and TIMP-3 downregulation in PTC remains to be investigated.
In conclusion, the present study suggests that the membrane mucins, MUC4 and MUC15, are overexpressed in tumor cells, and high MUC15 expression was associated with high malignant potential. MUC15 may serve as a prognostic marker and potential therapeutic target in PTC.
Footnotes
Acknowledgments
This work was supported by the Health Fellowship Foundation. We gratefully acknowledge the valuable technical assistance of Suil Ji.
Disclosure Statement
The authors declare that no competing financial interests exist.