
Abstract
Background:
Unilateral Graves' disease is a rare disease variant that can occur in a bilobar thyroid gland. We report the first documented case of unilateral Graves' disease in the left lobe of a bilobar thyroid gland and review the pertinent literature.
Patient Findings:
A 48-year-old man presented in June 2010 with thyrotoxicosis. I-131 radioisotope uptake was elevated at 33.4%, and scintigraphy revealed that uptake of the radioisotope was uniformly increased in the left lobe of the thyroid gland. Ultrasonography of the thyroid gland revealed a non-nodular, enlarged, and heterogeneous left lobe; Doppler investigation of the lobe showed hypervascularity classically seen in Graves' disease. The right lobe of the thyroid, on the other hand, appeared homogeneous and hypovascular on ultrasonography. Thyroid-stimulating immunoglobulin was significantly elevated at 191% (reference range <140%). Unilateral Graves' disease was the most likely diagnosis.
Summary:
As has occasionally been described in the literature, unilateral involvement of the thyroid gland is a rare presentation of Graves' disease. Pre-existing functional or structural differences (either congenital or acquired) between the two lobes may contribute to this rare presentation. To our knowledge, this is the first reported case of unilateral Graves' disease presenting in the left lobe of a bilobar thyroid gland.
Conclusion:
Although the pathophysiology of unilateral Graves's disease has not been clearly elucidated, clinicians should be aware that Graves' disease can present unilaterally in either lobe of the thyroid gland.
Introduction
Patient
In June 2010, a 48-year-old African-American male veteran was referred to our general endocrine clinic for evaluation of thyrotoxicosis. The patient had been involved in a minor motor vehicle accident, and at an outside hospital underwent a noncontrasted cervical-spine computed tomography, which showed a “mildly enlarged left lobe of the thyroid gland.” Subsequently, ordered thyroid function tests (TFTs) revealed a suppressed thyroid-stimulating hormone (TSH) level and elevated levels of free thyroxine and free triiodothyronine (Table 1). The patient endorsed a 10 lb (4.54 kg) unintentional weight loss over the preceding 2 months, as well as increased sweatiness and jitteriness. He had no significant medical history other than hyperlipidemia treated with simvastatin, vitamin D insufficiency on replacement therapy, and a mood disorder managed with citalopram. He denied use of over-the-counter supplements or other medications, and had no known family history of thyroid disorders. On examination, he was in no distress and had normal vital signs. There was no obvious thyroid orbitopathy, tremor, or dermopathy, and deep tendon reflexes were normal. The thyroid gland was palpable and slightly enlarged, with the left lobe being slightly larger than the right. There were no discrete nodules or masses appreciated, and the thyroid was nontender to palpation. A thyroid bruit was not noted on auscultation.
FT4, free thyroxine; FT3, free triiodothyronine; TSH, thyroid-stimulating hormone; TSI, thyroid-stimulating immunoglobulin; TPO-Ab, thyroid peroxidase antibodies; H, high; L, low.
Nuclear medicine imaging with I-131 performed on July 14, 2010, demonstrated an elevated uptake of 33.4%, with the increased activity distributed uniformly throughout the left thyroid lobe (Fig. 1). Ultrasonography of the thyroid gland performed and reviewed by our radiology department on July 22, 2010, showed a non-nodular, heterogeneous, and hypervascular left lobe measuring 5.5 × 2.1 × 2.3 cm (Figs. 2a, b); the right thyroid lobe measured 5.2 × 1.7 × 1.8 cm and was homogeneous and hypovascular in appearance compared to the contralateral lobe (Fig. 3). Given the significant elevation in thyroid-stimulating immunoglobulin (TSI) (Table 1) and radiologic findings suggestive of diffuse (rather than discrete nodular) hyperfunction of the left thyroid lobe, unilateral Graves' disease of the left thyroid lobe was considered the most likely diagnosis. The patient refused pre-treatment with methimazole. Given his relative young age and overall good health, he was prescribed a beta-blocker and referred for radioiodine ablation. His TFTs (Table 1) and radioisotope uptake of 34.2% on September 21, 2010, confirmed continuing hyperthyroidism immediately before receiving 19.8 mCi of I-131 sodium iodide.

Initial I-131 uptake concentrated in the left thyroid lobe.

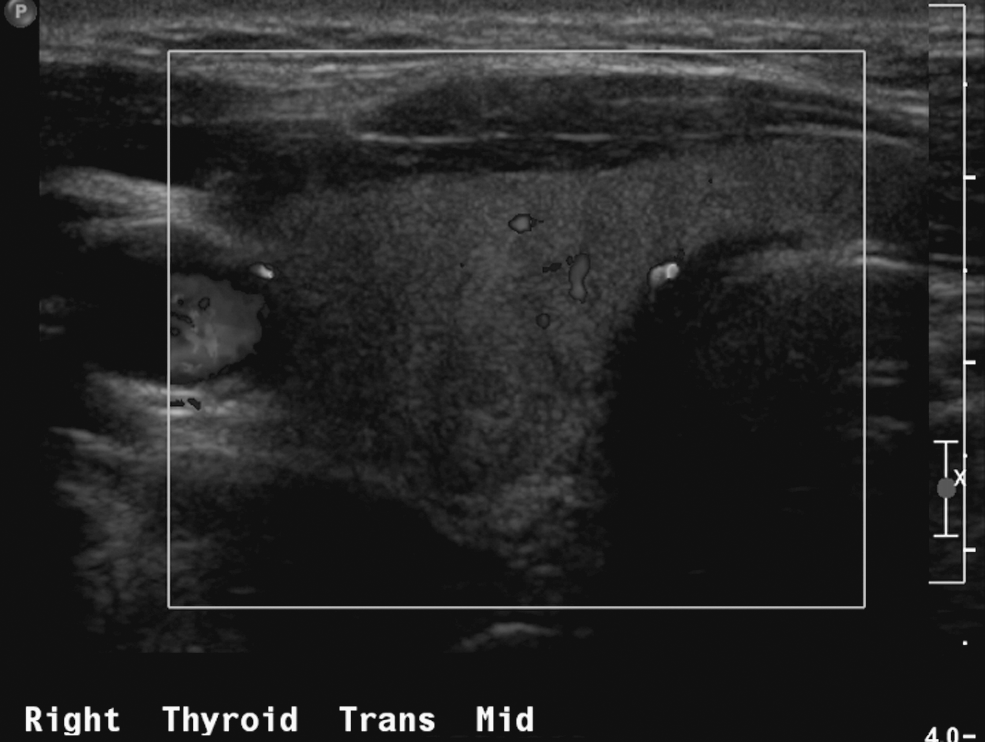
Transverse view on ultrasonography of the right thyroid lobe showing the homogeneous and hypovascular appearance of the lobe (color Doppler shown here in gray scale).
By January 2011, the patient had complete resolution of his hyperthyroid symptoms. His free thyroxine had normalized, and free triiodothyronine measurement decreased significantly (though remained above the upper limit of normal). TSH continued to be suppressed, not unexpected given the short period of follow-up (Table 1). On February 1, 2011, his 24-hour radioisotope uptake was determined to be normal at 21.3%, with the tracer now found homogeneously in the previously suppressed right thyroid lobe, and a small amount of uptake noted in the inferior left thyroid lobe (Fig. 4).
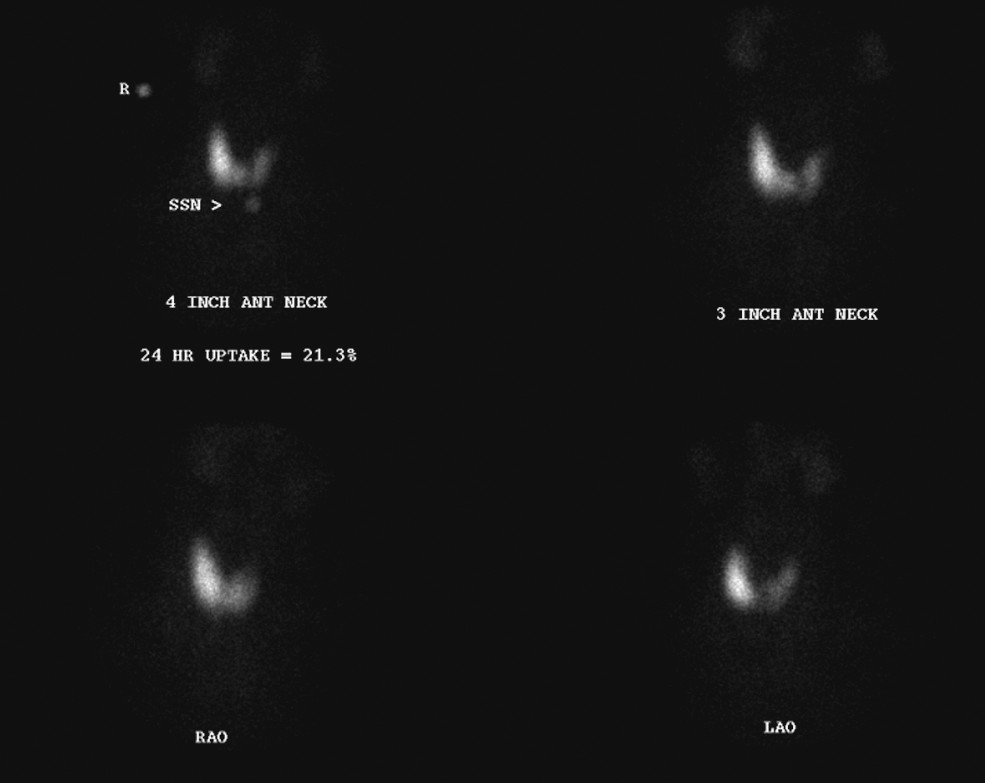
Post-treatment I-131 uptake is normal in a functional right thyroid lobe (small amount of uptake noted in the inferior left thyroid lobe).
Discussion
Unilateral Graves' disease not caused by thyroid hemiagenesis is rarely reported in the medical literature. In 1993, Sakata et al. were the first to describe this disease entity in two Japanese women with unilateral diffuse uptake of radioisotopes in the right thyroid lobe (1). Each patient underwent right hemithyroidectomy, and unilateral Graves' disease was diagnosed via histopathology showing hyperplastic columnar epithelium and infiltrative lymphocytes. In both cases, the patients became thyrotoxic due to hyperfunction of the remaining left thyroid lobe after 8 and 23 months, respectively, and were then successfully treated with long-term methimazole therapy.
In 1999, Dimai et al. described a 31-year-old female Caucasian patient who was thyrotoxic and had a unilateral goiter (2). Ultrasonography of the thyroid gland revealed changes consistent with autoimmune thyroid disease limited to the right lobe, and I-123 uptake was homogeneously concentrated in the right lobe. Fine-needle biopsy revealed lymphocytic inflammation of the right but not the left lobe, and thyroid receptor antibodies (TRAB) and thyroid peroxidase antibodies (TPO-Ab) were increased. Unilateral Graves' disease was diagnosed; the patient responded well to 12 months of thiamazol treatment and was still euthyroid 3 years after diagnosis.
In 2004 Gratz et al. reported a 33-year-old woman who presented with thyrotoxicosis and a heterogeneously enlarged right thyroid lobe with normal appearing left thyroid lobe on ultrasonography (3). Radioisotope uptake was concentrated in the right lobe, in addition to positive TRAB and TPO-Ab. Fine-needle biopsy sampling yielded densely packed lymphocytes from the right lobe but normal follicular cells from the left. The patient was maintained on long-term thiamazol with normalization of thyroid function labs.
In 2006, Italian authors Bolognesi and Rossi reported a 39-year-old man who was thyrotoxic and had positive TRAB and TPO-Ab (4). Ultrasonography showed a heterogeneous pattern limited to the right lobe, with Doppler examination showing much greater vascularization there as well. Radioisotope scanning showed unilateral uptake in the right lobe. Twelve months of methimazole treatment normalized the patient's TRAB and TFTs. Upon discontinuation of methimazole, the TSH again became suppressed; a repeat radioisotope scan showed an uptake pattern unchanged from the initial scan, confirming unilateral Graves' disease recurrence. This patient was the last reported case of unilateral Graves' disease occurring in a bilobar gland until now.
Interestingly, our patient had significantly elevated TSI after initially testing negative for TPO-Ab (Table 1). On the other hand, TPO-Ab was positive in each of the aforementioned cases that reported its value. Therefore, it is germane to note that our TSI bioassay (Thyretain TSI Reporter BioAssay; Diagnostic Hybrids, Athens, OH) performed by a reference lab has a 99.5% specificity for Graves' disease (5). TPO-Ab, though can be observed with Graves' disease, is absent in 20%–55% of the patients (6). Finally, TRAB testing would have provided good specificity but a low sensitivity of 67% (5), which is not acceptable in the setting of the low TPO-Ab titer. Our case reinforces the concept that when appropriately used in unusual or ambiguous clinical settings, TSI complements imaging studies and provides great diagnostic power.
To our knowledge, the present case is the first documentation in the medical literature of unilateral Graves' disease involving the left lobe of a bilobar thyroid gland. Each previously reported case of unilateral Graves' disease involved the right lobe of a bilobar thyroid gland, at least initially. Although the normal right thyroid lobe is usually larger than the left, there is no clear explanation for its predilection in hyperfunction (3). Epidemiological studies have revealed that thyroid hemiagenesis preponderantly involves the left thyroid lobe, though a much smaller number of cases of right lobe hemiagenesis has been reported as well (7 –10). Given this, it is possible that the right thyroid lobe may have yet to be elucidated vascular or developmental advantages over the left lobe in both organogenesis and functional status. Pre-existing functional or structural changes due to congenital (such as the isolated lymphatic draining of each lobe, which leads to differences in autoimmunity) or acquired factors (such as previous viral inflammation in the quiescent lobe) may play a part (11,12). It is also possible that in cases of unilateral Graves' disease in bilobar thyroid glands, the observed predilection for right lobe disease is due to chance. Regardless of the possible pathophysiology, our case adds to the existing medical literature in that unilateral Graves' disease confined to the left thyroid lobe in a bilobar gland is an observed phenotype.
Conclusion
We report the first case of unilateral Graves' disease in the left lobe of a bilobar thyroid gland. This case illustrates how the laboratory results and two radiographic modalities complemented one another and provided a complete picture of the patient's disease process. Our patient's positive TSI, hypervascular and heterogeneously enlarged left thyroid lobe on ultrasonography (compared to the hypovascular homogeneity of the right thyroid lobe), and the uniformly distributed increased I-131 uptake in the left thyroid lobe all point to unilateral Graves' disease as the unifying diagnosis. Pathophysiology of this disease variant has not been clearly elucidated, but clinicians should be aware that Graves' disease can present with unilateral involvement in either lobe of the thyroid gland.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.