
Abstract
Background:
In China, use of radioiodine therapy is problematic because of the need for lifelong levothyroxine substitution. Our aim was to find an optimum dosing strategy for 131I treatment of hyperthyroidism due to Graves' disease (GD). We attempted to achieve euthyroidism to avoid long-term levothyroxine treatment.
Methods:
Six hundred patients with GD were randomized into five groups, each comprising 120 individuals, to receive an individual 131I activity selected from five different ascending activity ranges. The ranges were modulated according to a clinical score system. Follow-up was extended over a 12-year time frame. The primary outcomes were euthyroidism, hyperthyroidism, hypothyroidism, and recurrent hyperthyroidism. The secondary endpoint was the accumulated 131I activity needed to achieve euthyroidism.
Results:
Out of 682 screened patients, 600 entered the study in 1997. Five hundred twenty-nine completed the last follow-up visit at the end of the study in 2009. Group 3 was identified as the study arm that received the optimum radioiodine activity, with 71.8% of the patients maintaining a euthyroid status, 5.8% remaining hyperthyroid, and 22.3% becoming hypothyroid by the end of the study. This group received 1.85–4.07 MBq per gram of thyroid tissue (average administered activity 261 ± 162 MBq). Over the 12-year follow-up period, the recurrence rate was 13.6%. The efficacy of 131I treatment was related to activities modulated by a clinical score (χ 2 = 82.1, p = 0.000).
Conclusion:
Our protocol effectively treated hyperthyroidism and significantly reduced the hypothyroidism rate. It may be preferable to the intentional induction of permanent hypothyroidism recommended by many experts.
Introduction
Methods
Study design
This 12-year prospective, randomized, open-label blinded end-point study was conducted in the Hyperthyroidism Treatment Center of the First Affiliated Hospital of the Sun Yat-Sen University, Guangzhou, China. A computerized system was used for randomization. After the input of a seed number, 600 eligible patients were matched to a randomized number generated according to their visit sequence. The randomization numbers were ranked in ascending order. Before that, we set the numbers modulo 5, with a residue of 1, 2, 3, 4, 0, which was assigned to group 1, 2, 3, 4 and 5, respectively. A stepwise activity escalation scheme was assigned to the five groups, comprising a 131I activity range in seven steps. The study's clinical phase began in April 1997 and ended in December 2009. A study period of 12 years was appropriate, as our previous data still showed changes in outcomes after an observation period of 9 years (2). No regulatory changes affected the study during the study period. It was in conformity with the Declaration of Helsinki and approved by the Dongshan district authorities. At the time the study was established, there was no formal institutional ethics committee in existence. All of the patients or their parents gave written informed consent.
Study population
We screened 682 patients with GD and older than 8 years, between April and December 1997. Radioiodine treatment in children and adolescents in China is exceptionally accepted as an alternative to ATD. Before treatment, its potential hazards are discussed with their parents compared with ATDs, which are considered no less harmful. Six hundred eligible patients (Fig. 1) agreed with our study protocol and met the following inclusion criteria: (i) newly diagnosed GD, patients on ATDs, which was suspended 2 weeks before 131I treatment, or patients with a history of taking ATDs; (ii) thyroid function serum tests confirmed hyperthyroidism; (iii): 24-hour uptake of 131I ≥40%. If the uptake was <40%, sources rich in iodine were restricted (food or pharmaceuticals) until the uptake was ≥40%.
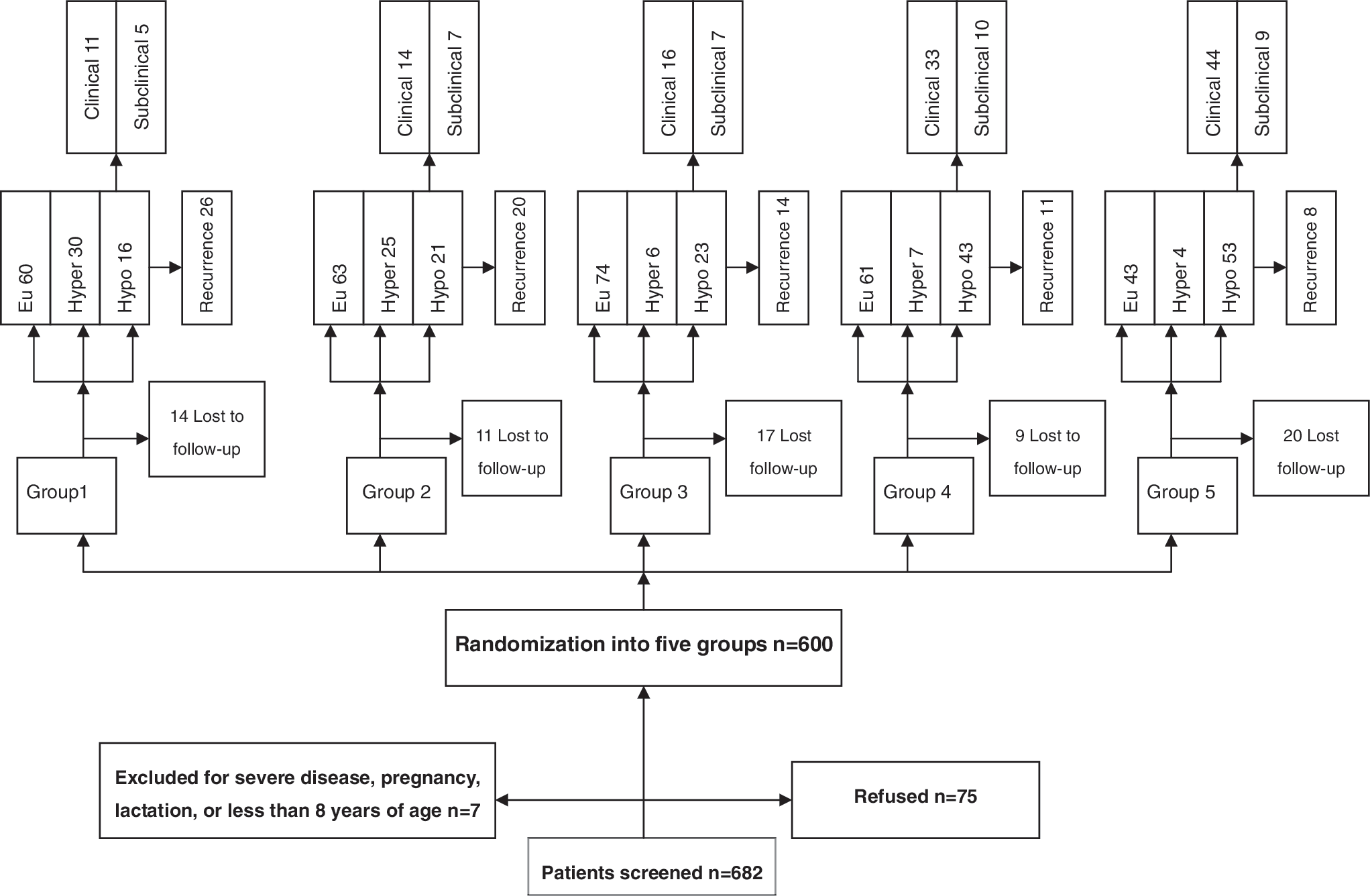
Study flow diagram and outcome.
The study population included different stages of the disease, as presented in the general characteristics (Table 1).
ATD, antithyroid drug; FT3, free triiodothyronine; FT4, free thyroxine; S-TSH, super-sensitive thyrotropin; Md, median.
Exclusion criteria were (i) elevated liver enzymes, or elevated creatinine; (ii) agranulocytosis; (iii) pregnancy (excluded by testing) or lactation; (iv) patients younger than 8 years.
Interventions
The five groups received 131I activities according to a clinical score range. We used a scoring system to combine the factors to select the activity that was validated in an earlier work and described in an earlier study (2) that included no subjects of this study. Within each group, patients received a range of varying dosages of radioiodine depending on clinical factors, including patient age, length of disease, complications, the severity of their hyperthyroidism, use of ATDs, and gland characteristics (Table 2). Thus, a score ranged from 0 to 12. The basic activity unit of 0.37 MBq/g of thyroid tissue at score 0 was increased by 0.37 MBq/g every 2 scores (range 0.37–5.55), resulting in seven incremental steps. Group 1 to 5 started with activities of 0.37, 1.11, 1.85, 2.56, and 3.33 MBq per gram of thyroid tissue at score 0 (Table 3). The MBq activity to be administered was then calculated based on a formula using probe measured 131I thyroid uptake (131I TU) of a test activity:
Total score ranges from 0 to 12, increase per 2 score is 0.37 MBq.
The thyroid weight was ultrasonically assessed by two specialists using a Biosound Esaote AU4 device (Rome, Italy) and a 10 MHz probe. The mean value of the weight was taken, using the ellipsoid formula to estimate the gland lobe volumes from its mean axes. Interobserver and intraobserver precision for this method (3) was in the same 12% to 14% range as others have demonstrated (4).
Maximum administered outpatient activity was limited to 555 MBq 131I due to authority restrictions. Activities exceeding the limit were administered after a 1 week interval for regulatory reasons. This activity was included in the overall calculation of the first treatment activity. At the 3- or 6-month follow-up visit, a determination was made whether or not the patient should receive a second treatment following the same calculation method as for their first assignment. The same procedure was applied for a third treatment, which was necessary for eight patients. The decision was based on elevated free triiodothyronine levels (FT3) and clinical symptoms. Patients with hyperthyroidism were advised to restrict their intake of food rich in iodine during the whole study period.
Follow-up
Patients were examined at intervals of 2–4 weeks during the disease, if they were stable. The intervals were extended to 3–6 months thereafter. At each visit, a complete history was recorded, and a physical examination was performed. Thyroid hormones FT3, free thyroxine (FT4), and super-sensitive thyrotropin (S-TSH) were tested; other tests were performed as needed. The normal range in our laboratory is as follows: FT3: 2.91–9.08 pmol/L, FT4: 9.05–25.50 pmol/L and S-TSH: 0.4–3.1 uIU/mL. Thyrotropic receptor antibodies (TRAb) were not estimated due to high costs. It was also not a focus within this study. Every patient in the five groups, except those lost to follow-up, was followed-up over 12 years by experienced physicians who were unaware of the patient's treatment assignments. They reviewed the data to determine which patients had reached study end-points. After the administration of 131I, all patients with hyperthyroid were administered a beta blocker (propranolol) over the whole study period as necessary; three months after 131I, they also received ATDs if necessary (either methimazole or propylthiouracil). ATD was withdrawn 3 days before the follow-up visits. Patients developing hypothyroidism were treated with levothyroxine.
End points
Study end-points included euthyroidism, hyperthyroidism, clinical hypothyroidism, and subclinical hypothyroidism occurring each year. Recurrence was separately counted during the 12 years. The definition for euthyroidism was FT3, FT4, and TSH in the normal ranges, no thyroid medication; for persisting hyperthyroidism: FT3 and/or FT4 higher than the normal ranges and/or decreased TSH after the withdrawal of ATDs before sampling; for recurrence: FT3 and/or FT4 elevated above normal ranges after the withdrawal of ATDs over at least 2 years; and for hypothyroidism: FT3 and/or FT4 below normal ranges, or only elevated TSH, without levothyroxine substitution.
The secondary end-point was the accumulated amount of 131I activity to achieve euthyroidism.
Statistical analysis
The sample size was estimated by the method of multiple comparisons of rates. In consideration with the multi-factor analysis with more baseline factors and patients lost to follow-up, and patients excluded due to side effects, a target enrollment of 600 patients was planned, 120 in each group. One-way analysis of variance assessed measurement data of the baseline characteristics. The categorical data was R × C chi-squared tested. The Wilcoxon rank sum test was applied to analyze non-normally distributed numerical variables. Group differences in outcome were assessed using R × C chi-squared tests. Multinomial logistic regression was used to determine the relationship of 131I activity and end-point. The dependent variables were: 1 = euthyroidism, 2 = hyperthyroidism, and 3 = hypothyroidism (including subclinical). The independent variable was 131I activity. The baseline was euthyroidism. The optimum activity was determined according to the following definition: success rate = [1–not cured rate (hyperthyroidism)], and as low as possible hypothyroidism rate.
The SPSS software (version 13.0) for Windows was used for all analyses.
Results
Out of 682 screened patients, 82 patients were excluded before randomization: 75 (11.0%) due to the withdrawal of their agreement, 7 (1.0%) due to severe damage of the liver or kidneys, severe agranulocytosis, pregnancy or lactation, or because they were younger than 8 years of age. Six hundred eligible patients were assigned a randomized number according to their hospitalization sequence (Fig. 1). Twenty-five patients younger than 18 were included: 3 were children, 9, 10, and 11 years of age; 22 were adolescents, age 14–17.
Seventy-one of 600 (11.8%) patients were lost to follow-up over the study period. Among the remaining 529 patients, the total range of 131I activities was 18.5–1443 MBq. Thirty-six patients were administered 131I twice, and 8 patients received three administrations.
The remaining patients in the five groups showed no significant differences in baseline characteristics (Table 1).
The efficacy per year for euthyroidism, hyperthyroidism, and hypothyroidism is shown in Figure 2a–c. The end-of-year 12 efficacy showed highly significant differences between the end-points of the five groups (χ 2 = 82.1, p = 0.000). In particular, the optimum activity group 3 had the highest rate in euthyroidism, with the lowest rate of hyperthyroid and hypothyroid cases (Table 4).
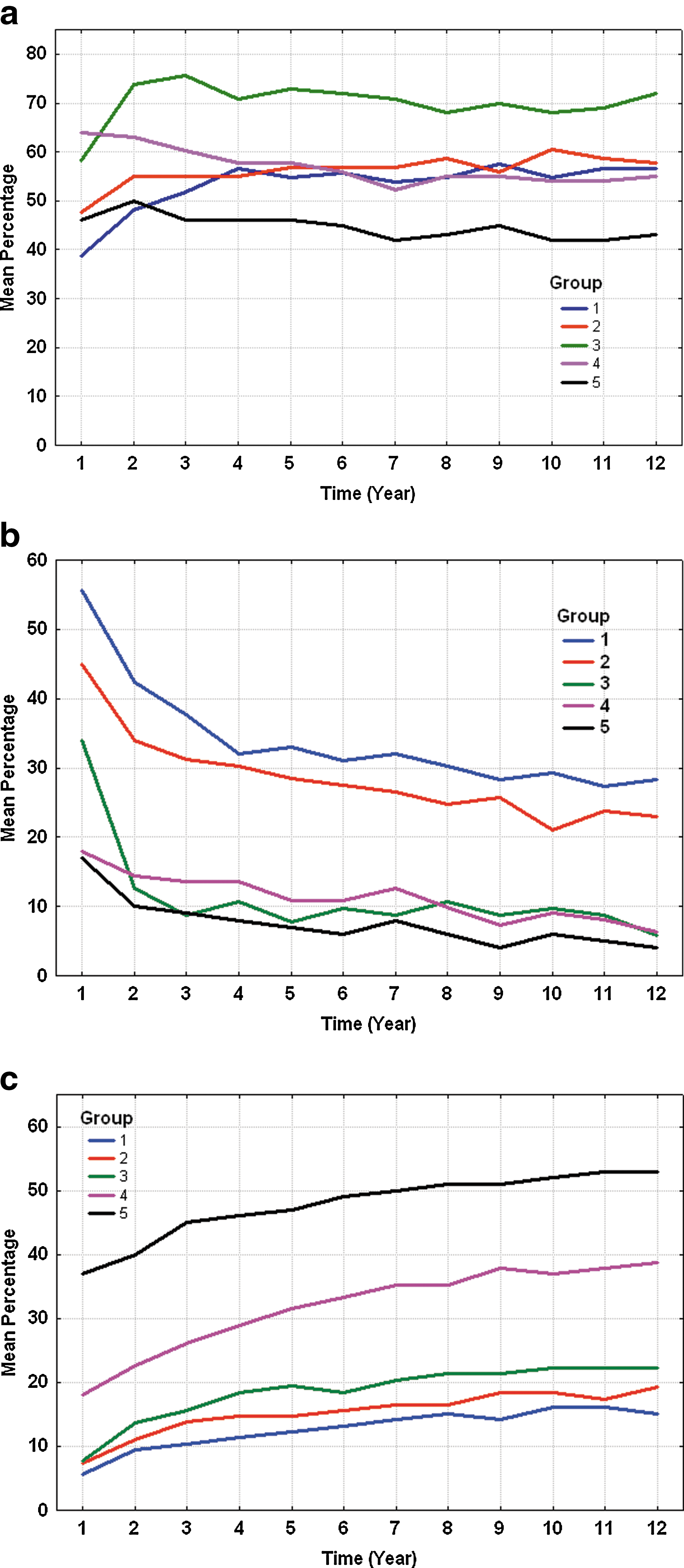
Primary study endpoints at end of each year after first administration:
The total number of recurrences within 12 years in group 3 was moderate (χ 2 = 14.8, p = 0.005). In summarizing these findings, group 3 had the optimum activity scheme, including the clinical features score, according to the aim of our study. The logistic regression analysis showed that the efficacy of 131I was associated with the activity (Table 5). A negative β1 coefficient of −0.40 represented a decrease of hyperthyroidism at an odds ratio of 0.67 by ascending group activity ranges. A positive β2 coefficient of 0.41 independently represented a higher hypothyroidism rate, occurring at an odds ratio of 1.50 for each administered group-by-group activity increase. The average group-by-group 131I mean (standard deviation) activity ranges were 131(99), 180(110), 261(162), 320(218), and 410(257) MBq. The proportion of overlap between the groups, as expressed by the Cox and Snell coefficient of determination, was only 11%.
χ 2 = 747.997, df = 2, p = 0.000.
OR, odds ratio; CI, confidence interval.
The mean ATD treatment period after radioiodine therapy was approximately 6 months; most of the patients tended to be euthyroid. For patients with hypothyroidism, a relatively low levothyroxine replacement activity (50–100 μg/day) was sufficient. Some of them were temporarily hypothyroid. After several months to years of intervention, they finally became euthyroid or hyperthyroid. Eight out of 37 cases of temporary hypothyroidism occurred 1 year after 131I treatment. Twenty-six out of 37 finally became euthyroid, and 11 relapsed hyperthyroid. Interestingly, there were nine cases that had received a very low 131I activity (≤74 MBq) and became hypothyroid, and two cases with very high 131I activities (≥1110 MBq) still remained hyperthyroid. We were unable to identify predictive factors for such cases. As important secondary outcomes, we did not see any death rate during the observation time of our study. Ophthalmopathy was also not significantly different between the groups at study entry and at the end of the study, similar to the 131I study arm in a previous study (2).
Discussion
We began to develop a low dose concept to reduce hypothyroidism and to offer an alternative to ATD therapy, which frequently lasted over 10 years. There was also a growing demand for radioiodine therapy by parents refusing surgery for their children after long-term ATD therapy had failed. Since radioiodine therapy for benign thyroid disorders is considered safe worldwide, we were challenged to minimize hypothyroidism as the most frequent side effect.
For this study, radioiodine was administered first-line, followed by antithyroid medication as needed to control hyperthyroidism. The usefulness of the clinical features was derived from logistic regression analyses of our preceding study (2) in which we employed a fixed 131I activity in a group of GD. Despite potential weaknesses, these insights were used as a clinical score. In patients with hard glands, complications, a long course of disease, previous ATD treatment, and of an older age, the thyroid tissue appeared to be less sensitive to 131I. Patients with these characteristics tended to have a higher 131ITU or a higher absorbed activity per gram of tissue, respectively. Although this approach is different from the guideline-recommended pretherapeutic calculation of an absorbed activity, it is not uncommon to adjust (mainly increase) 131I activity according to clinical judgement in daily practise. We did not see any disadvantage in giving such an approach a systematic level, in comparison to individual decisions.
A shortcoming of our study could be the lacking TRAb information at patient recruitment due to unavailability. However, careful analysis of other studies revealed that a relatively high number of TRAb-negative or normal-range GD cases were also accepted (5), suggesting that the diagnosis in such cases was mainly based on thyroid hormone levels and clinical findings, as was in our study.
In comparison to a number of other studies, a significantly larger portion of our patients were rendered euthyroid at the end of our study period (6 –9). As a potential ethnic influence affecting our outcome, Asians may require lower radioiodine activities to achieve a cure, compared with non-Asians. However, this issue would be beyond this study. Concerning potential hazards of 131I therapy in children, it is important to understand that thyroid doses resulting from 131I are in high deterministic ranges, causing cell death, rather than in tumour-inducing stochastic low dose levels (10,11). There is no evidence of tumor induction through 131I therapy (12).
Our previous study (2) independently showed that 21.5% of the patients who received radioiodine became hypothyroid after 9 years; only a few cases occurred in the last year of observation. Using the same treatment concept in this study (which is not a follow-up study), no late hypothyroid cases were observed in group 3 after 10 years.
In our study, we found a useful approach for first-line low activity 131I administration, followed by ATDs as necessary if the patient was still hyperthyroid. Early hypothyroidism within 2 years due to high activity concepts is widely accepted, theoretically, whereas patients receiving low activity treatment can even recover to euthyroidism after several months of levothyroxine treatment. This may be due to a functional recovery of thyroid cells that escaped necrosis. Late hypothyroidism after several years is probably not related to 131I activity, and recovery to euthyroidism is rarely observed. In a different study, we even observed hypothyroidism after ATD therapy alone (2). In a small fraction of patients with GD, hypothyroidism may finally occur during a natural course.
Our target was the optimization of the outcome in light of later patient care, especially in rural areas. Following current guidelines, there is a tendency to achieve a rapid cure using high 131I activities, at the expense of a high and early hypothyroidism rate requiring lifetime care (13 –18). Such guidelines do not match the needs of patients in developing countries such as China. In our study, in comparison, the highest average activity of 410 ± 257 MBq resulted in only 4% hyperthyroidism, but with more than twice the hypothyroidism rate, as compared with 261 ± 162 MBq. This can be compared with others who observed a significant 40% of hyperthyroid and 46% of patients with hypothyroidism with GD (19), even with a low dose strategy (20). The odds ratio in our study groups suggested that a 30% increase of average activity per group induced 3.5 times more patients with hypothyroidism from the lowest to the highest group.
Short time to cure may enhance patient compliance and in many countries, affordability of substitution is not a factor. However, in China, compliance with and availability of lifelong levothyroxine substitution imposes a burden on patients in our huge rural population. With a mean life expectancy of more than 40 years after 131I therapy of GD, it matters whether 50% or 20% of patients should have replacement therapy and lifetime follow-up care. Regarding the incidence of GD, a much higher number out of approximately 10 million patients treated with 131I would need substitution. Thus, our concept may be preferable to the intentional induction of early hypothyroidism using 3–4 times higher fixed activities, followed by a lifelong correction (19). With our concept, hyperthyroidism was not prolonged, and the need for ATDs was shorter and less frequent compared with the recommendation of first-line ATD treatment (16).
Hypothyroidism is claimed to be associated with increased mortality (2,21 –24). Therefore, striving for a treatment concept that reduces the hypothyroidism rate seems to be justified. Compared with the high 10-year rate of 59% and 25-year rate of 82% hypothyroidism (25) seen with other treatments, our data suggest that such high rates could be avoided. Although others focus on the most accurate dosimetric concepts, as requested by council directives issued by authorities (16), our concept appeared to be simple and more effective.
Further, 131I induced contribution in cancer incidence was found to be activity dependent (26,27). Although this issue remains unconfirmed, it was attributed to activities above 260 MBq (8,27), supporting our individual low activity concept. However, at the end of the study, which was beyond the latency period, no malignancies occurred in our young subjects. Finally, if we want to ask “is there anything new” (27), the answer we should consider that in a country with huge rural and undersupplied areas, our tailored activity concept could significantly decrease long-term hypothyroidism rates and its burden on patients, reported to exceed 90% after 35 years (6). Better than the intentional “sledgehammer approach” to the problem (28), our study could demonstrate an alternative and efficient concept, which may be similarly effective in comparable parts of the world. Even though data show a conclusive tendency after 12 years, the shortcoming may still be too short an observation time, suggesting the need for another follow-up.
Footnotes
Acknowledgment
The authors are grateful to Dr. David S. Cooper for his competent suggestions and highly appreciated advice.
Disclosure Statement
None of the authors have to declare any potential conflict of interest. This research did not receive any specific grant from any funding agency in the public, commercial, or not-for-profit sector.