
Abstract
Background:
Distant metastases are more common in patients with follicular thyroid carcinoma (FTC) than in patients with papillary thyroid carcinoma, and the outcome is often poorer in patients with distant metastases. In this study, we attempted to identify the risk factors for distant metastases in FTC.
Methods:
Between 1989 and 1997, 134 patients with FTC underwent initial surgery, and their median follow-up period was 12.5 years. Seventeen patients had widely invasive FTC, and 117 had minimally invasive FTC. Distant metastases were observed in 36 patients (26.9%). Thirteen of these patients had distant metastases at the time of initial surgery (M1), and in the other 23 patients distant metastases were diagnosed with during their follow-up periods. Risk factors for distant metastases and cause-specific survival were analyzed. The factors analyzed were age at the time of initial surgery, sex, primary tumor size, histological findings (invasiveness, extent of vascular, and capsular invasion), and distant metastases at the time of initial surgery.
Results:
Univariate analysis showed that age and primary tumor size were significant factors related to postoperative distant metastases in the group of 121 patients who did not have distant metastases at the time of initial surgery. When the patients with M1 were included, the cumulative distant metastases-free-survival rate was significantly lower in the group with widely invasive FTC. The cumulative survival rate was significantly higher in the groups of patients with the minimally invasive type, who were under 45 years old, whose primary tumor size was under 4 cm and who did not have distant metastases at the time of the initial surgery. Multivariate analyses showed that tumor size and age were significant risk factors for postoperative distant metastases and that age and the presence of distant metastases at the time of the initial surgery were significant risk factors for poorer cause-specific survival.
Conclusion:
Age and primary tumor size were significant risk factors for postoperative distant metastases. Based on the findings in this study, we conclude that conservative management is sufficient for younger patients with minimally invasive FTC whose primary tumor is small.
Introduction
Hemithyroidectomy is generally performed to treat follicular tumors that are indeterminate as to whether they are follicular carcinomas preoperatively. Completion total thyroidectomy and radioiodine (RI) ablation is usually recommended when pathological diagnosis of follicular cancer has been made (11,12). Serum thyroglobulin (Tg) levels are a sensitive marker for recurrence after completion total thyroidectomy and RI ablation (13,14). Not all patients with FTC develop a recurrence or distant metastases, however, and only selected patients who have risk factors for distant metastases should undergo completion total thyroidectomy and RI ablation.
In Japan, the use of RI is strictly limited by law, and RI ablation cannot be used to treat all patients with FTC. Thus, a risk factor analysis for distant metastases in patients with FTC is a necessary and reasonable means of selecting patients for completion total thyroidectomy and RI ablation. We retrospectively analyzed the outcome and risk factors for prognosis and distant metastases in FTC.
Subjects and Methods
Between 1989 and 1998, 2390 patients with differentiated thyroid carcinoma underwent initial surgical treatment at our institution. Of them, FTC was diagnosed in 180 patients (7.5%), but 17 patients with concomitant PTC, 26 patients with oxyphilic cell carcinoma, and 3 patients with clear cell carcinoma were excluded from this study. The remaining134 patients were adopted as the subjects of this study. Patients with poorly differentiated FTC were not included, because the biological characteristics of poorly differentiated FTC and the therapeutic strategy are different from those of differentiated FTC. The surgical specimens were all reexamined histologically by one of the co-authors (K.K.), and the diagnoses were reconfirmed. The pathological diagnosis and classification of the follicular carcinoma were based on the recent World Health Organization classification system (15). The presence of capsular and/or vascular invasion and the absence of nuclear features of PTC defined pathological diagnosis of FTC. According to the degree of invasiveness, FTC was classified as minimally invasive follicular carcinoma and widely invasive follicular carcinoma. When limited capsular and/or vascular invasion was observed, follicular carcinoma was classified as minimally invasive, whereas when widespread infiltration of adjacent thyroid tissue and/or blood vessels was observed, follicular carcinoma was classified as widely invasive. There were 117 patients with the minimally invasive type and 17 with the widely invasive type. Follicular adenoma had been diagnosed in one patient postoperatively, but distant metastases were discovered 3 years after surgery. Another patient had neither vascular nor capsular invasion, but cervical lymph node metastases were diagnosed histologically. These patients were classified as having minimally invasive FTC.
The patients consisted of 103 women and 31 men, and their average age was 44.7 years old (y/o) (range; 10–83 y/o). The median follow-up period was 150 months. The median size of the primary tumor was 49 mm (range: 7 to 105 mm). The demographic data are summarized in Table 1. The standard initial surgical procedure used to treat patients with a follicular tumor in our institution has essentially been lobectomy. If a patient had a concomitant benign thyroid disease, that is, Graves' disease or a nodular goiter of the opposite lobe, or had distant metastases, total or subtotal thyroidectomy was performed. The initial operation performed on the subjects of this study was lobectomy in 110 patients, subtotal thyroidectomy in 10 patients, and total thyroidectomy in 14 patients. Fifty patients underwent lymph node dissection, because lymph node metastases were suspected on the basis of a preoperative ultrasound examination and lymph node metastases were confirmed histologically in 14 (28%) of them. Completion total thyroidectomy was performed in patients with minimally invasive FTC only when there were obvious distant metastases, whereas it was performed in all patients with the widely invasive type of FTC regardless of whether distant metastases had been diagnosed preoperatively. Curative surgery was performed in all patients except in those who were distant-metastases-positive preoperatively (M1), and no macroscopic residual tumor was observed in any of the patients who were distant-metastases-negative preoperatively (M0). Most patients with M0 underwent less than total thyroidectomy, and RI ablation or RI scintigraphy was not performed in these patients. All patients were followed in the outpatient clinic of our hospital. Postoperative follow-up studies were usually performed at 1 month, 3 months, 6 months, 12 months, and every 6 months thereafter. The serum Tg level was routinely measured at every hospital visit, and a chest computed tomography (CT) scan was performed routinely once a year. When a gradual increase in the postoperative Tg level was observed, a chest CT scan and bone scintigraphy were performed. If no metastatic sites were detected, completion total thyroidectomy was performed and was followed by 131I scintigraphy and FDG-PET CT. All patients with M0 underwent completion total thyroidectomy and RI therapy when a recurrence was detected. All patients with M1 underwent total thyroidectomy as the initial surgical procedure and subsequent RI therapy.
M1: Patients with distant metastasis preoperatively.
Fisher's exact test.
Including patients with a postoperative histological diagnosis of follicular adenoma.
χ2 test.
Patients who underwent cervical lymph node dissection only.
The data were analyzed with a statistical software program (JMP 8.0, SAS Institute, Inc., Cary, NC). Cumulative cause-specific survival (CSS) and cumulative distant-metastases-free survival (DMFS) were analyzed. A univariate analysis was conducted in relation to CSS and DMFS by the Kaplan-Meier method for the following variables: age at surgery (<45 vs. 45 y/o or more), sex, tumor size (<4 cm vs. 4 cm or more), histological type (minimally invasive vs. widely invasive), degree of capsular invasion, degree of vascular invasion, and initial distant metastases (M0 vs. M1, analyzed in relation to CSS only). Differences between groups were analyzed for significance by the log-rank test. Multivariate analysis was performed by using the Cox proportional hazard model. The significant factor was shown with the hazard ratio of each category, and p-values <0.05 were regarded as statistically significant.
Results
As of a median follow-up time of 150 months, 36 patients (26.9%) had distant metastases. Thirteen (9.7%) of them had distant metastases at the time of the initial surgery, and the other 23 (19.1%) developed distant metastases during their follow-up periods (M2). Patients in whom distant metastases were diagnosed before 1 year after surgery were classified as M1 patients, and patients in whom distant metastases were diagnosed >1 year after initial surgery were classified as M2 patients. The initial distant metastases in the M2 patients was detected at a mean interval of 70 months after initial surgery, and the intervals ranged from 12 to 189 months. The sites of the distant metastases were bone alone (n = 13), lung alone (n = 12), both bone and lung (n = 7), brain (n = 2), and multiple sites, that is, lung, bone, and brain (n = 1) and lung, liver, and brain (n = 1). Lung and/or bone were the most frequent sites of metastases. All patients who had undergone less than total thyroidectomy as their initial surgery underwent RI therapy and surgery and/or external radiation after completion total thyroidectomy when distant metastases were later detected.
A total of 18 patients, 9 of the M1 patients and 9 of the M2 patients, died of their disease, and all 18 had distant metastases. Of these 18 patients, 11 had lung metastases and 12 had bone metastases. Four M1 patients were transferred to other hospitals near their home for follow-up, and the hospitals were asked for a report of their outcome.
Significantly more patients with preoperative distant metastases were observed in the groups of patients who were 45 y/o or more, whose primary tumor was size 4 cm or more, whose tumor was the widely invasive type, who were positive for capsular invasion, and who had lymph node metastases (Table 1). After excluding the M1 patients, postoperative distant metastases were significantly more common in the groups of patients who were 45 y/o or more and in the group whose primary tumor size was 4 cm or more (Table 2). Of the 117 patients with minimally invasive FTC, 26 patients had capsular invasion alone, 33 patients had vascular invasion alone, and 58 patients had both vascular and capsular invasion. Distant metastases were observed in 4 patients (15.4%) with capsular invasion alone, 6 patients (18.2%) with vascular invasion alone, and 16 patients (27.6%) with both vascular and capsular invasion. There was no statistical significance among distant metastases ratio of these patients groups. Cumulative DMFS was also not significant among these three groups (data not shown).
M2: Patients developed distant metastasis during follow-up (excluding M1 patients).
Fisher's exact test.
Including patients with a postoperative histological diagnosis of follicular adenoma.
χ2 test.
Patients who underwent cervical lymph node dissection only.
The CSS curve for all patients calculated by Kaplan-Meier method is shown in Figure 1, and the 10-, 15-, and 20-year CSS rates of the patients were 89.9%, 84.6%, and 79.2%, respectively. CSS was significantly poorer in the groups of patients who were 45 y/o or more, whose primary tumor size was 4 cm or more, whose tumor was the widely invasive type, and in the M1 group (Fig. 2A–D). The 10-, 15-, and 20-year CSS rate of the M0 patients were 96.1%, 93.6%, and 84.8%, respectively, whereas the 5- and 10-year CSS rate of the M1 patients were 41.0% and 30.8%, respectively. Thus, the outcome of the group with distant metastases was poorer.

Cumulative cause-specific survival (CSS) curve of all patients with follicular thyroid carcinoma. The 10-, 15-, and 20-year CSS rates were 89.9%, 84.6%, and 79.2%, respectively.
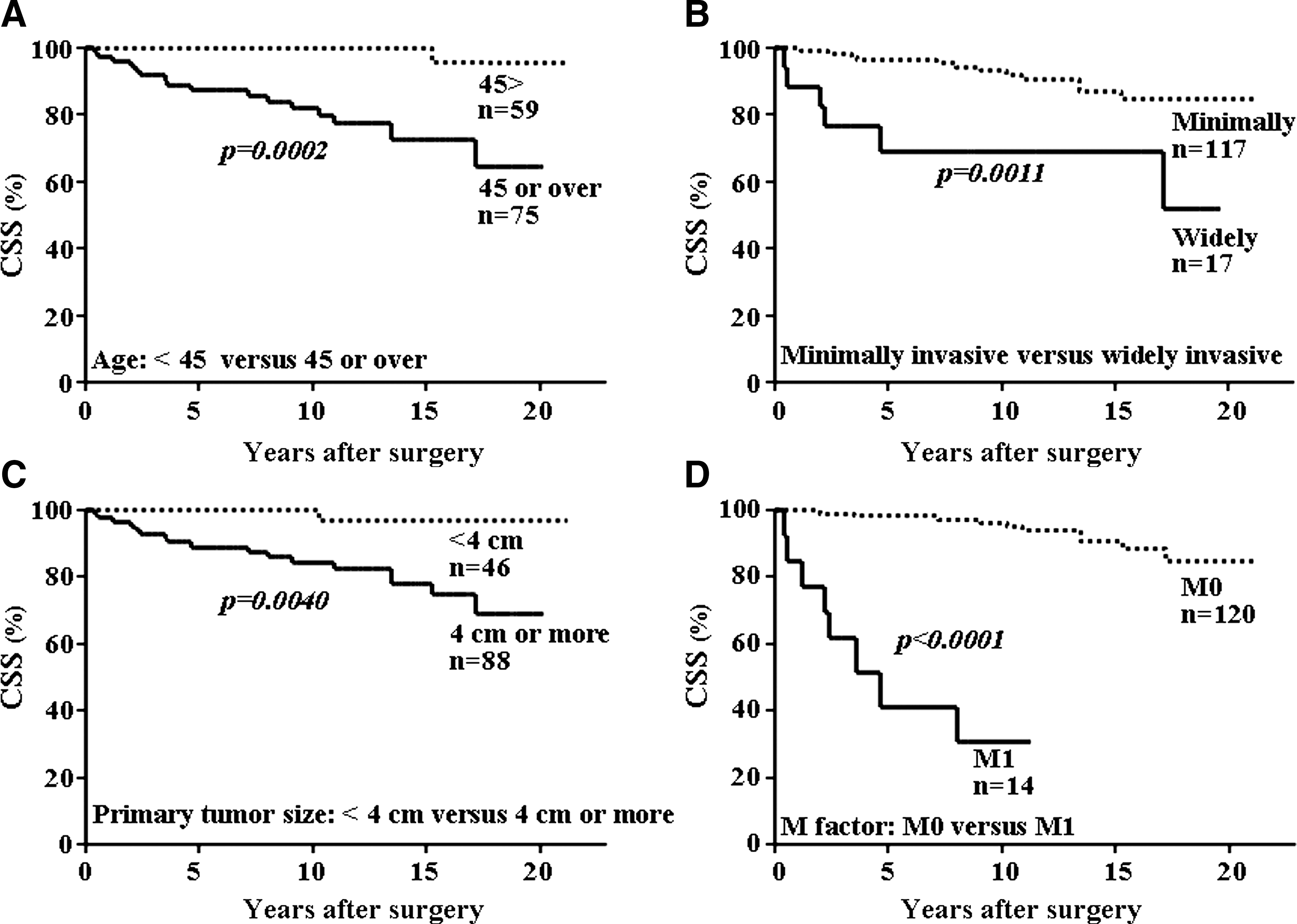
Univariate analysis in relation to CSS. The groups of patients who were 45 y/o or over, whose tumor were widely invasive type, whose primary tumor size were 4 cm or more, and who had distant metastasis at the time of the initial surgery, had significantly poorer outcome.
The DMFS curve of the 121 M0 patients calculated by the Kaplan-Meier method is shown in Figure 3, and their 10-, 15-, and 20-year DMFS rates were 85.2%, 75.9%, and 73.5%, respectively. The DMFS rate was significantly lower in the groups of patients who were 45 y/o or more and whose primary tumor size was 4 cm or more (Fig. 4A, C). The difference in DMFS rates between the group with the minimally invasive type and the group with the widely invasive type was not significant (Fig. 4B). The difference in DMFS rates between the group with capsular invasion alone and the group in which vascular invasion was positive was not significant (Fig. 4D).

Cumulative distant-metastases-free survival (DMFS) curve of the patients without distant metastasis at the initial surgery. The 10-, 15-, and 20-year DMFS rate were 85.2%, 75.9%, and 73.5%, respectively.

Univariate analysis in relation to DMFS. The groups of patients who were 45 y/o or over and whose primary tumor size were 4 cm or more, had significantly lower DMFS rates. However, invasiveness and vascular invasion did not have a significant effect on DMFS.
The results of the multivariate analyses in relation to CSS and DMFS are shown in Table 3. Age 45 y/o or more and M1 were identified as independent and significant prognostic factors for poorer CSS. Significant factors related to DMFS in the M0 group were age 45 y/o or more and tumor size 4 cm or more. When M1 patients were included in the multivariate analysis in relation to DMFS, which was calculated as distant metastases occurring at the same time of surgery in M1 patients, widely invasive type was identified as one of independent prognostic factors related to DMFS.
Discussion
FTC is often discussed together with PTC as differentiated thyroid cancer. Both arise from follicular epithelial cell and usually have a favorable prognosis. However, there are several differences between the biological behaviors of these two malignancies. PTC often metastasizes to lymph nodes, whereas frequently FTC metastasizes to distant sites, and that is why the prognosis of FTC is poorer than that of PTC. The prognostic factors and surgical strategy for FTC should be discussed separately from those of PTC.
Many studies have shown that the incidences of FTC and anaplastic thyroid carcinoma are higher in iodine deficiency areas (16,17) and that PTC is predominant in iodine-replete populations. Populations starting iodine prophylaxis demonstrate an increase in the ratio of PTC to FTC. The distribution and characteristics of thyroid tumors in former iodine-deficient countries have approached those of iodine-sufficient countries. Japan has been known to be an iodine-sufficient country and the biological characteristics of FTC in formerly iodine-deficient countries are thought to be similar to those of FTC in Japan. The outcome of FTC in iodine-deficient areas has been reported to be poorer than in iodine-sufficient area. In our series, 9.7% of the patients had distant metastases on presentation, and the reported percentage of M1 patients varied from 3.1% to 21% (18 –27). Ito et al. (28) of Japan reported that 5.1% of their patients had distant metastases at the time of surgery, and the low prevalence of distant metastases at surgery reflected the indolent biological characteristics of FTC in iodine-sufficient areas. They also reported that 29 (9.2%) of 316 M0 patients developed distant metastases during their follow-up periods, whereas distant metastases were observed in 23 (19.0%) of our 121 M0 patients. The 10-year CSS rate and the 10-year DMFS rate of the M0 patients in our study were 96.1% and 85.2%, respectively, almost the same as reported by Ito et al., and they were much higher than in previous reports from other countries (19 –21,23,25). Iodine intake is thought to be related to the biological behavior of FTC. In most Japanese institutions, routine RI ablation after completion total thyroidectomy is not performed for all patients in whom FTC has been diagnosed histologically after lobectomy (28,29). The reason is that the use of RI is strictly restricted by law, and Japanese endocrine surgeons and endocrinologists do not consider FTC as having as poor a prognosis in Japan as it does in other countries. That is also why the treatment strategy for FTC is not as aggressive in Japan as it is in other countries. The proportion of patients with minimally invasive FTC who had distant metastases (22%) was clearly high, but both the 10-year DMFS rate and CSS rate in this study were almost the same as in other recent reports (Table 4).
Number in parentheses are reference numbers.
10-year DFS (disease free survival) was reported instead of DMFS.
The 10- and 5-year CSS rates of the M1 patients in our study were 41% and 30.8%, respectively, and much lower than those of the M0 patients. Distant metastases are thought to be the most important prognostic factor, and since no method of preventing distant metastases has ever been reported, only early treatment for distant metastases might improve the prognosis. RI ablation after completion total thyroidectomy is the standard strategy for the treatment of FTC diagnosed pathologically after lobectomy. However, >80% of our patients did not develop distant metastases, and completion total thyroidectomy did not seem necessary in these patients. Our results showed that the risk factors for distant metastases after thyroidectomy were age and primary tumor size. Our paper is not the first to report tumor size as a prognostic factor for FTC. Some authors (9,18,20,25,27 –29) have already suggested the existence of a difference in outcome according to tumor size, although the tumor size categories varied from report to report. We adopted 4 cm as the cut-off value for tumor size, because it is the tumor size in the definition of T3 in the TNM classification system.
The widely invasive type has been reported to be a risk factor for distant metastases (19,27,28) and RI ablation after completion total thyroidectomy has been indicated for the treatment of patients with the widely invasive type. The difference between the DMFS rates of the group with the minimally invasive type and the group with the widely invasive type was not significant. Statistical analysis would be inappropriate because of small number of M0 patients with the widely invasive type of FTC (10 patients). The difference in CSS rates between the group with the minimally invasive type and the group with the widely invasive type was significant, because almost 60% of the patients with the widely invasive type had distant metastases whereas only 20% of the patients with the minimally invasive type had distant metastases (with M1 patients included in both groups). Multivariate analyses showed that the significant and independent factor related to distant metastases were age and primary tumor size. When the M1 patients were included, the results of multivariate analysis indicated that the independent factors related to distant metastases were age, primary tumor size, and invasiveness. Several histological factors, including widely invasive type, vascular invasion, and differentiation, have previously been reported to be related to poorer CSS (19,24,27,28,30). We excluded poorly differentiated carcinoma from our series, because poorly differentiated thyroid carcinoma is classified as an independent clinical entity separate from PTC and FTC in the 2004 World Health Organization classifications (15). The treatment strategies for poorly differentiated carcinoma should be discussed separately from the strategies for differentiated thyroid carcinoma.
Vascular invasion has been regarded as an important predictor of developing distant metastases, and FTCs with capsular invasion alone rarely give rise to distant metastases (19,22,31,32). However, the same as in other studies (5,10,33,34), we were unable to show a relationship between distant metastases and vascular invasion. Patients without vascular invasion should be followed carefully.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.