
Abstract
Background:
Paragangliomas in the region of the thyroid gland are rare tumors that can present a diagnostic challenge by mimicking follicular and c-cell derived thyroid tumors.
Summary:
Thyroid-associated paragangliomas are likely a subset of laryngeal paragangliomas and, although quite rare, should be considered in the differential diagnosis of a hypervascular thyroid nodule. The preoperative diagnosis of thyroid-associated paragangliomas can be challenging since the cytologic and histologic features overlap with more common primary thyroid neoplasms, in particular medullary carcinoma. Differential expression of a panel of immunohistochemical markers, including neuro-specific enolase, chromogranin A, synaptophysin, keratin, and S100, can be used to distinguish thyroid-associated paragangliomas from primary thyroid tumors. Intraoperatively, thyroid-associated paragangliomas may be associated with significant intraoperative bleeding and are often densely adherent to surrounding tissues, including the recurrent laryngeal nerve. Interestingly, the aggressive local behavior of these tumors does not correspond to potential for malignancy, as there are no patients with malignant thyroid-associated paragangliomas reported in the medical literature. Therefore, these tumors may be treated with limited resection. Postoperatively, patients with paragangliomas should receive hormonal evaluation for functional disease, imaging evaluation for multicentric and metastatic disease, and genetic counseling.
Conclusion:
Thyroid-associated paragangliomas are an important part of the differential diagnosis of a hypervascular thyroid nodule, especially in a patient with a fine-needle aspiration biopsy suggestive of medullary thyroid carcinoma, but with unremarkable serum calcitonin levels. Consideration of a thyroid-associated paraganglioma also has important operative and postoperative implications for determining the extent of thyroid resection as well as follow-up testing.
Introduction
Review
Origin of thyroid-associated paragangliomas
Paragangliomas adjacent to or inside the thyroid gland are likely a subset of laryngeal paragangliomas and were first described in 1974 by Haegert and colleagues (6). Laryngeal paraganglia are branchiomeric and consist of two, paired structures called the superior and inferior laryngeal paraganglia (Fig. 1). These paraganglia normally reside between the superior edge of the thyroid cartilage and the first tracheal ring (8). Thyroid paragangliomas are thought to arise from the inferior laryngeal paraganglia (glomus laryngicum inferior). The normal inferior laryngeal paraganglia is approximately 0.4 mm in diameter and is located along the recurrent laryngeal nerve at the lateral margin of the cricoid cartilage in the cricothyroid membrane (9). One hypothesis is that as a paraganglioma forms from the inferior laryngeal paraganglia, it is slowly dragged downward and ultimately rests lateral to the thyroid gland. It is also possible that the inferior laryngeal paraganglia may form in the thyroid capsule itself, which could ultimately create an intrathyroidal paraganglioma.
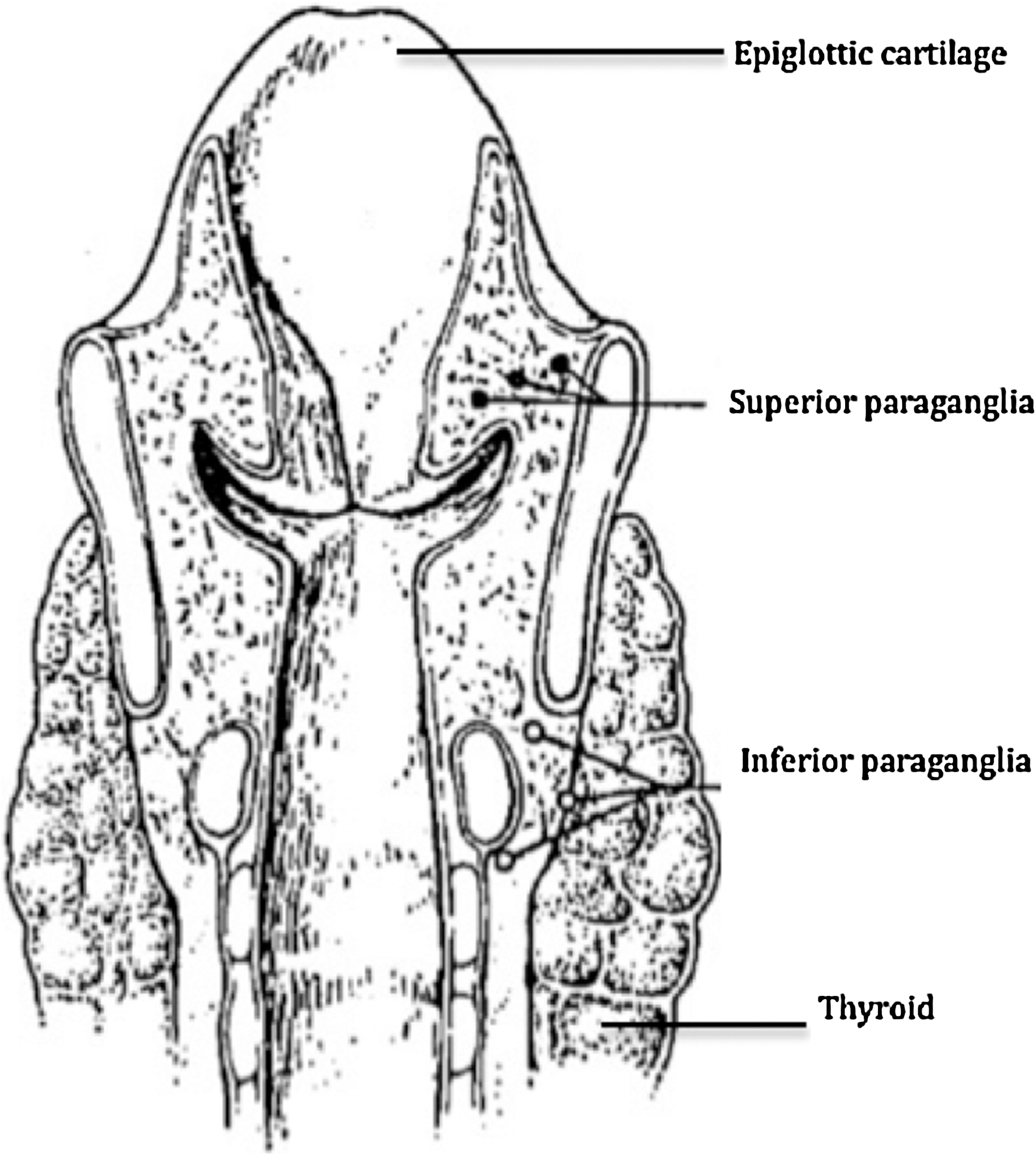
Line drawing of the anatomical location of the superior and inferior paraganglia. Modified with permission from Lawson and Zak (7).
Clinical presentation
Tables 1 through 3 summarize all 28 thyroid-associated paragangliomas described in the English-language published medical literature from 1965 to 2010. Table 1 summarizes the preoperative and intraoperative findings, and postoperative complications of these paragangliomas. In most cases the clinical presentation is characterized as a relatively large (mean tumor size of 3.3 cm, range is 1.5–10.0 cm) thyroid mass with an indeterminate or suspicious fine-needle aspiration (FNA) biopsy. In only one reported case did the preoperative FNA biopsy reveal the final diagnosis (6). The mean age of presentation is 48 years (range is 24–73 years of age) with a female predominance (25 women vs. 3 men) and no difference in laterality. In terms of preoperative biochemical work-up, all patients with reported thyroid paragangliomas are euthyroid (10,15 –19,21,27) with normal calcitonin and carcinoembryonic antigen (CEA) levels (8,21,23,25), and negative antiperoxidase and antithyroglobulin antibodies (21,27). When obtained, thyroid paragangliomas typically appear as a cold nodule on thyroid scintigraphy (10,13,15,16,18). Most importantly, on ultrasonography imaging, thyroid paragangliomas are typically solid, with a hypoechoic structure and remarkable intranodular and peri-nodular vascular flow on color Doppler analysis (8,21,23).
M, male; F, female; R, right; L, left; N/A, not available; MTC, medullary thyroid carcinoma; PTC, papillary thyroid cancer; Hemi, hemithyroidectomy; Total, total thyroidectomy; Subtotal, subtotal thyroidectomy; RLN, recurrent laryngeal nerve.
CH-A, chromogranin A; NSE, neuron specific enolase; TH, tyrosine hydroxylase; S-100, sustenacular; CT, calcitonin; CGRP, calcitonin gene-related peptide; CEA, carcinoembryonic antigen; EMA, epithelial mebrane antigen; CK, cytokeratin; Tg, thyroglobulin; TTF-1, Thyroid transcription factor-1.
MRI, magnetic resonance imaging.
Differential diagnosis of thyroid-associated paragangliomas
Paragangliomas in the region of the thyroid gland are rare tumors that can present a diagnostic challenge for the pathologist by mimicking follicular and c-cell-derived thyroid tumors. The differential cytologic and histologic diagnosis of a thyroid-associated paraganglioma includes medullary thyroid carcinoma, Hürthle cell neoplasm, parathyroid neoplasia, metastatic renal cell carcinoma, hyalinizing trabecular tumor, insular carcinoma, and metastatic neuroendocrine tumors to the thyroid (14) (Table 1).
By light microscopy, paragangliomas are composed of two different cell types, chief cells and sustentacular (structural) supporting cells. These cells form loose nests called “zellballen,” (German for “balls of cells”) that are surrounded by an extensive network of vascular sinusoids. The predominant cell of paragangliomas is the chief cell, a polygonal-shaped cell with delicate oncocytic cytoplasm, round nucleus, and granular chromatin. The microscopic features of paraganglioma overlap with those of other neuroendocrine tumors, particularly medullary carcinoma. However, ancillary immunohistochemical studies can be used to distinguish paraganglioma form other entities in the differential diagnosis. As summarized in Table 2, the chief cells of paragangliomas are typically positive for neuro-specific enolase, chromogranin A, and synaptophysin, and the sustentacular cells are positive for S-100. Paragangliomas are negative for calcitonin, CEA, thyroglobulin, epithelial membrane antigen, and cytokeratins. However, a rare subset of laryngeal paragangliomas have been described that are positive for calcitonin, and medullary thyroid carcinomas that contain S-100 positive sustentacular cells have also been reported (28,29).
Intraoperative findings of thyroid-associated paragangliomas
Intraoperative findings that are consistent with a paraganglioma include a hypervascular thyroid nodule with a trabecular pattern of prominent veins, densely adherent to surrounding tissues, and substantial intraoperative bleeding. In general, it is believed that the blood supply of thyroid paragangliomas stems from the superior thyroid artery (15). The combination of displacement of the normal anatomy and dense adhesions likely explains the higher incidence of bleeding and recurrent laryngeal nerve palsies (Table 1). Interestingly, paragangliomas adjacent to or inside the thyroid gland can show “invasive-like” nerve involvement. However, as highlighted in Table 3, aggressive local behavior does not necessarily correspond to malignant disease as even thyroid paragangliomas with extension into the trachea, larynx, mediastinum, and the esophagus have no evidence of metastatic disease up to 9 years after resection (10 –12,15). The extent of initial surgery for thyroid paraganglioma is unclear, but thyroid lobectomy for disease limited to a single thyroid lobe appears to be sufficient based on our review of the medical literature (15,18).
Postoperative follow-up of thyroid-associated paragangliomas
In general, less than 10% of all paragangliomas are malignant (4). Unfortunately, there are no unequivocal histologic or immunohistochemical markers that distinguish benign from malignant paragangliomas (30). Therefore, it is generally accepted that a paraganglioma is malignant only if it metastasizes to non-neuroendocrine tissues. The most common non-neuroendocrine sites include regional spread to cervical lymph nodes and distant spread to the lung, liver, bone, and skin (3). There are no patients with malignant paragangliomas adjacent to or inside the thyroid gland described in the medical literature, although reported follow-up times have been relatively short (2 months to 8 years) (Table 3). Therefore, no recommendations can be given for follow-up screening to evaluate for recurrence or metastasis.
Paragangliomas are derived from embryonic neural crest cells that are part of the extra-adrenal chromaffin and nonchromaffin cellular system. Therefore, the chief cells of all paragangliomas contain cytoplasmic neurosecretory granules with the potential to exhibit physiological activity through catecholamine excess. However, the reported incidence of hyperfunctioning paragangliomas is only 1%–3% in the head and neck, and there are no reported patients with hyperfunctioning thyroid-associated paragangliomas (Table 3) (31). Nevertheless, it is generally recommended that all patients with a newly discovered paraganglioma should receive a biochemical work-up for catecholamine excess.
Paragangliomas can occur simultaneously in multiple paraganglia in the head and neck, thorax, or abdomen and pelvis. Approximately 14% of patients who presented with a thyroid-associated paraganglioma also had disease in either the carotid body or glomus vagale (Table 3). Therefore, follow-up imaging should include computed tomography (CT) imaging or magnetic resonance imaging of the neck, chest, and abdomen/pelvis. The use of 18F-DOPA positron emission tomography is a relative new imaging modality that has highlighted tumors that may be too small for magnetic resonance imaging (30,32). It also has the advantage of imaging the skeleton to evaluate for bone metastases. Follow-up imaging should occur relatively soon after initial surgery so that concurrent disease can be identified and not confused with metastatic or recurrent disease.
Approximately 10% of patients with paragangliomas are familial and 90% are sporadic. However, up to 30% of all apparently sporadic head and neck paragangliomas are actually caused by a germline mutation on either chromosomes 1 or 11, and are part of a paraganglioma syndrome (30). Paraganglioma syndromes have been classified into four types, each with a corresponding gene mutation in succinate dehydrogenase. Succinate dehydrogenase normally encodes for protein subunits of complex II in the mitochondrial electron transport chain. Mutations in succinate dehydrogenase may activate an angiogenic pathway that ultimately leads to tumorigenesis (33). Because of the important implications of germline mutations in the succinate dehydrogenase genes, all patients with these rare tumors should undergo genetic counseling and possibly genetic testing.
Illustrative Patients
Patient #1
The patient was a 41-year-old Caucasian woman with no significant medical history, who was incidentally noted on routine exam to have a 3.4-cm neck mass most consistent with a left-sided thyroid nodule. The patient was asymptomatic and denied any radiation exposure or family history of endocrinopathies. On examination, the mass was firm and mobile; there was no lymphadenopathy. Thyroid function testing and serum calcium were all within normal ranges. An initial FNA biopsy consisted primarily of blood and was nondiagnostic. A repeat FNA biopsy contained a dispersed population of polygonal cells and was diagnosed as “suspicious for a medullary carcinoma”; however, the patient's serum calcitonin and CEA levels were normal.
The patient was referred to the MGH Endocrine Surgery Unit. A repeat office neck ultrasonography identified a 3.6-cm hypoechoic nodule that appeared to lie adjacent to the left thyroid lobe. An ultrasound-guided FNA biopsy was performed by our group and was diagnosed as “Atypia of undetermined significance,” consisting of plasmacytoid cells present singly in a background of large aggregates of spindled cells and inflammatory cells (Fig. 2A). The patient was consented for an excisional biopsy of the mass with frozen section and possible total thyroidectomy and neck dissection as indicated.
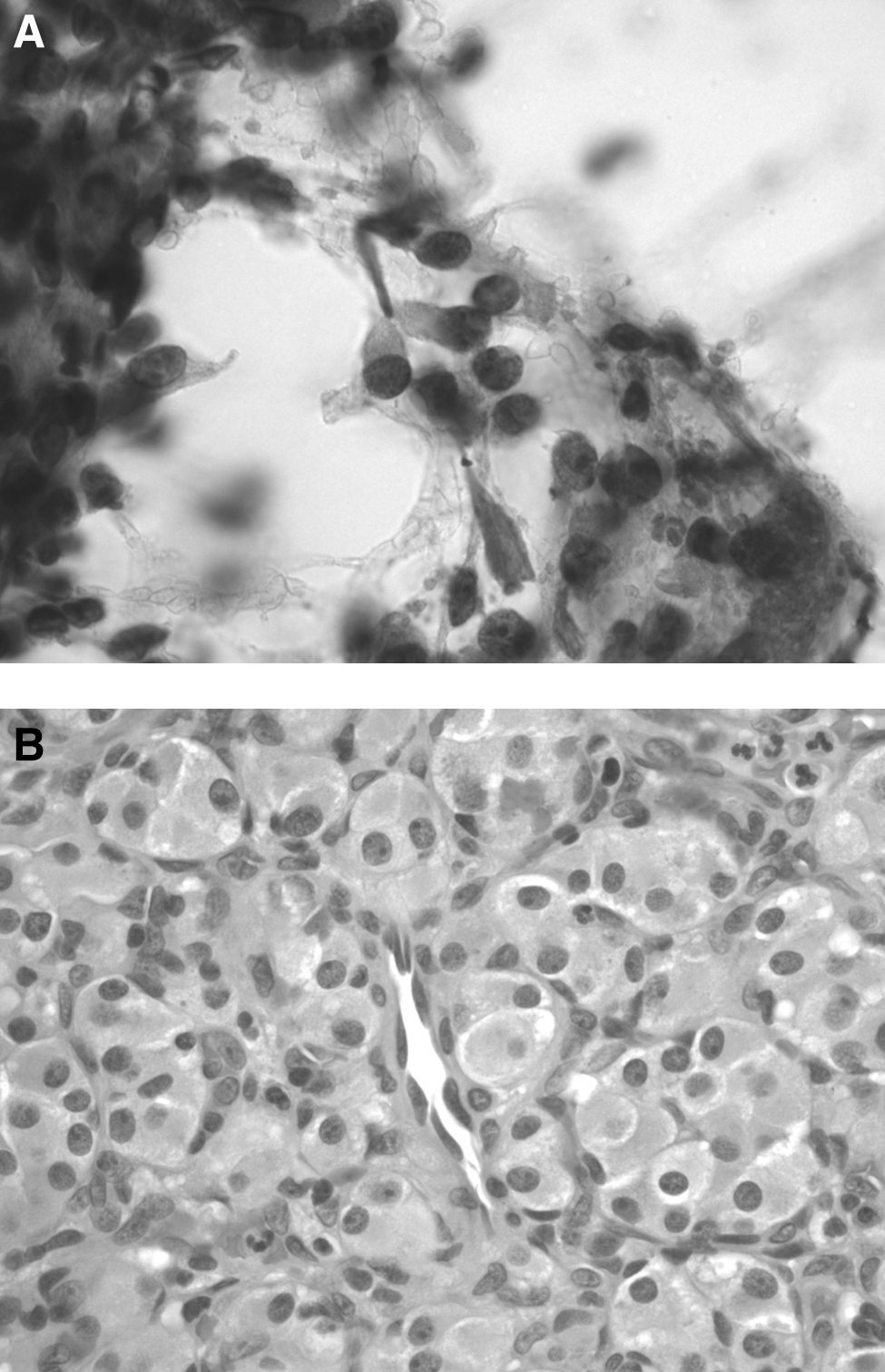
In the operating room, the mass was lateral, deep, and separate from the thyroid gland, lying on the cervical fascia posterior to the carotid artery. The mass was rubbery with a great deal of neovascularization encompassing it. These vessels were individually ligated and the mass was carefully separated from the vagus nerve. Grossly, the mass was well circumscribed, tan, and solid, with several foci of hemorrhage. Intraoperative frozen section was performed and was consistent with a paraganglioma. Histologically, the tumor exhibited a characteristic “zellballen” pattern of growth (Fig. 2B). Immunohistochemical studies showed that the neoplasm was positive for chromogranin A and synaptophysin with sustentacular cells staining for S-100, and negative for calcitonin, keratin, CEA, and TTF-1, supporting the diagnosis of paraganglioma.
Postoperatively, the patient had no complications and was noted to have normal urinary catecholamines, metanephrines, and normetanephrines. A CT scan and repeat ultrasonography of the neck noted no other tumors. Total follow-up time was 14 months.
Patient #2
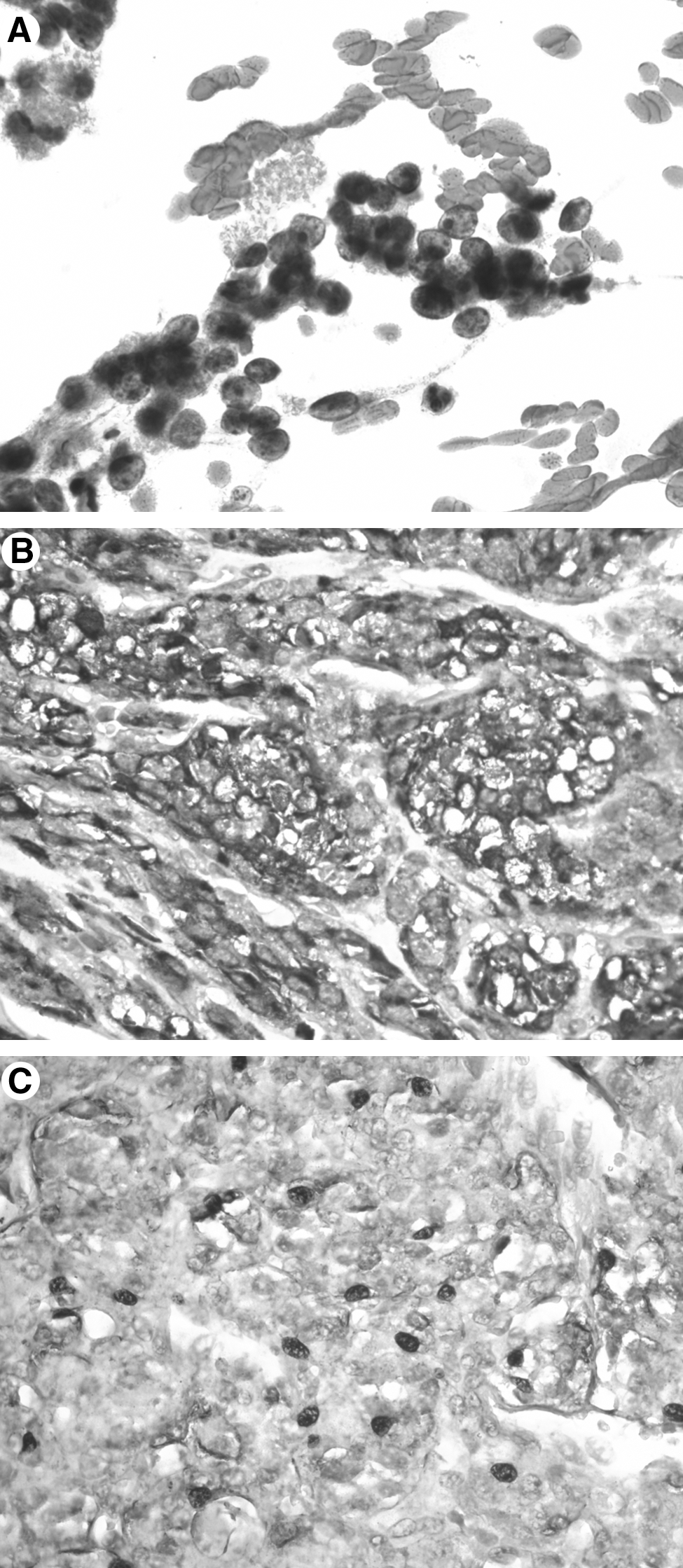
The second patient was a 73-year-old Somali refugee with no significant medical history. She presented to the MGH Thyroid Unit with a 40-year history of a slowly enlarging right neck mass. Thyroid ultrasonography demonstrated partially calcified bilateral thyroid nodules with a dominant, very hypervascular, right-sided nodule measuring 4.0 cm, and no lymphadenopathy (Fig. 3). An ultrasound-guided FNA biopsy of the nodule was reported as “atypia of undetermined significance” and consisted of scant follicular cells with mild cytoarchitectural atypia. A repeat FNA biopsy noted crowded follicular groups with both nuclear atypia and an abnormal cytoarchitectural pattern that was “suspicious for a follicular neoplasm” (Fig. 4A). The patient was asymptomatic from the thyroid nodules, had no history of radiation exposure, and denied any family history of endocrinopathies. Physical examination demonstrated a firm and mobile right thyroid nodule. Given the presence of bilateral thyroid nodules, the patient was offered a total thyroidectomy.

In the operating room, the patient was noted to have a dominant right-sided thyroid nodule extending toward the right upper pole. During dissection of the patient's right upper thyroid pole, diffuse bleeding was noted from the area of the dominant nodule. The upper and lower poles were secured after identifying the upper and lower parathyroid glands, respectively, and the entire thyroid lobe was rotated medially. Dissection of the recurrent laryngeal nerve in the tracheoesophageal groove was very difficult due to persistent diffuse bleeding from the thyroid nodule and dense fibrotic attachments between the recurrent laryngeal nerve and the nodule.
On gross pathological examination, there was a three-centimeter solid, tan, rubbery, well-circumscribed mass in the superior pole extending to the thyroid capsule. Two smaller calcified nodules were noted in the inferior and mid-poles measuring 0.2 and 0.3 cm, respectively. An intraoperative frozen section of the upper right thyroid nodule was highly suspicious for medullary thyroid carcinoma. We elected to not proceed with a completion left thyroidectomy due to the extensive right laryngeal nerve dissection as well as the continuous bleeding from the right side of the neck.
On final pathological examination, the tan mass was separate from the right thyroid lobe. Microscopic examination of the mass revealed a tumor consisting of loosely arranged polygonal chief cells within nests and surrounded by S-100-positive sustentacular cells. Immunohistochemical studies showed that the chief cells were diffusely positive for chromogranin A and negative for thyroglobulin, keratin, calcitonin, CEA, and TTF-1 (Fig. 4B, C). Postoperatively, the patient's thyroid function was normal, but she noted a weak, higher-pitched voice with increasing vocal fatigue throughout the day and aspiration with thin liquids. Direct laryngoscopy demonstrated right vocal fold paralysis. CT imaging of the abdomen and pelvis demonstrated normal adrenal glands and a partially calcified mass in the portocaval region. A CT scan and repeat ultrasonography of the neck noted no other tumors. A 24-hour urine collection for catecholamines, metanephrines, and normetanephrines was normal. She received genetic counseling and subsequent genetic testing was negative for RET or SDH mutations. Total follow-up time was 13 months.
These two patients highlight the diagnostic challenges associated with thyroid-associated paragangliomas. Radiographic, intraoperative, and pathologic findings in both cases were completely consistent with paragangliomas. Also, neither of these patients had evidence of concurrent paraganglioma disease. Their postoperative care highlights the important role of follow-up radiographic studies, as well as biochemical and genetic testing.
Summary/Conclusions
Although paragangliomas of the head and neck and particularly those associated with the thyroid gland are rare, they should be considered in the differential diagnosis of a hypervascular thyroid nodule. Cytologic and histologic features overlap with more common primary thyroid neoplasms, but immunohistochemical studies can be used to aid in the diagnosis. Postoperatively, patients with paragangliomas should receive hormonal evaluation for functional disease, imaging evaluation for multicentric and metastatic disease, and genetic counseling. Finally, local tissue extension of paragangliomas near or in the thyroid does not correspond to malignant disease and can be treated with limited resection.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.