
Abstract
Background:
Ectopic thyroid tissue is a rare finding but has been reported in many thoracic and abdominal locations. It is usually an incidental pathologic finding after an unrelated surgical intervention. When thyroid tissue is found outside the thyroid bed, it is important to rule out thyroid cancer metastasis.
Patient Findings:
We present a case of a 61-year-old African American woman who was incidentally found to have concomitant ectopic thyroid tissue in the adrenal gland and a papillary thyroid microcarcinoma (PTMC) in the right lobe of the thyroid.
Summary:
The concurrent finding of ectopic thyroid tissue and PTMC posed the diagnostic dilemma of whether the extrathyroidal tissue was metastasis or metaplasia, with very different treatment implications. Although many of these incidental micropapillary cancers are indolent, some patients do experience local or distant metastasis. Therefore, it is important to delineate which of these microtumors are likely to metastasize. Some tumor markers and gene mutations have been proposed to help differentiate the more benign tumors from the more aggressive tumors, but there is currently no standard method for determination of metastatic potential.
Conclusions:
Here we present the seventh known case of ectopic thyroid tissue in the adrenal gland and the first case of concomitant incidental PTMC in the setting of this ectopic tissue finding. Using this case, we discuss the diagnostic and therapeutic challenges faced and propose the use of biomarkers to help determine the metastatic potential of these tumors.
Introduction
Patient
A 61-year-old African American woman presented with refractory hypertension, hypokalemia, and metabolic alkalosis consistent with hyperaldosteronism. She underwent aldosterone and renin screening, a saline suppression test, computed tomography (CT) imaging of the abdomen/pelvis, and bilateral adrenal venous sampling. A sub-centimeter left-sided adrenal adenoma was discovered with a 10:1 lateralizing ratio, confirming appropriate aldosterone production. Laparoscopic left adrenalectomy was performed as definitive treatment.
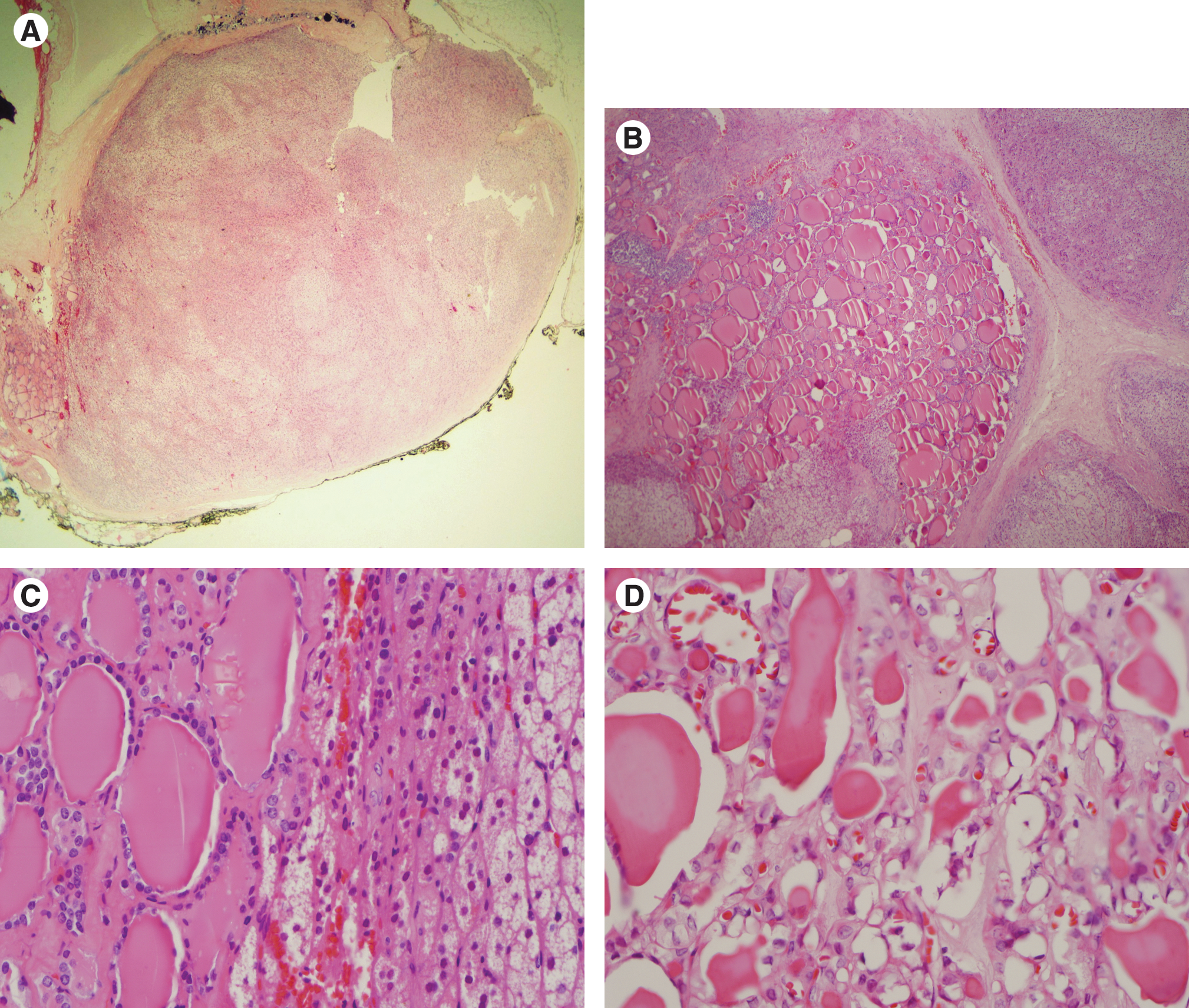
Pathology examination of the lesion revealed a 0.8 cm adrenocortical nodule consistent with a functioning adenoma. There was also an unexpected finding; an adrenal rest consisting of bland thyroid tissue and ossification spanning several millimeters in diameter was found directly adjacent to and within the capsule of the adenoma (Figure 1A, B, C). Immunohistochemical staining of the thyroid tissue with thyroglobulin (Tg) confirmed a thyroid focus.
Because of this unexpected pathologic finding, a work-up was performed to evaluate for thyroid cancer. The patient had no high-risk history, including no history of childhood head or neck irradiation and no family history of thyroid carcinoma. Thyroid function tests were performed and revealed a thyroid-stimulating hormone (TSH) of 1.12 μIU/mL (reference range, 0.550–4.780). Thyroid ultrasonography revealed a multinodular goiter with the following lesions: a right-sided 4.5 × 4.1 × 4.3 mm hypoechoic nodule with rim calcification and minimal circumferential vascularity, a larger 18.2 × 14.2 × 7.8 mm mixed lesion in the isthmus, and two larger nodules in the left lobe (19.6 × 14.8 × 15.0 mm, superior and isoechoic and 19.0 × 13.2 × 17.0 mm, inferior and hypoechoic). None of the nodules had ultrasonography characteristics that were particularly worrisome for carcinoma. Central and lateral neck lymph node evaluation was also done and was negative for abnormal-appearing nodes. In concordance with the American Thyroid Association (ATA) guidelines (1), a fine-needle aspiration (FNA) biopsy of the two left-sided lesions was performed. The left superior thyroid nodule consisted of follicular epithelial cells with focal Hurthle cell change, colloid, and rare histiocytes favoring non-neoplastic goiter. The left inferior thyroid nodule consisted of Hurthle cells, rare pigment-laden macrophages, and multinucleated giants cells and colloid. In both specimens, comment was made of focal Hurthle cell change and rare atypia with possibility of vague intranuclear inclusions and nuclear grooves, which were thought to be artifactual in origin. Still, the pathologist could not completely rule out a neoplastic process. Because of the finding of thyroid tissue in the adrenal gland and the inconclusive outcome of the FNA biopsy, the patient underwent total thyroidectomy with lymph node sampling.
Pathological evaluation of the thyroid gland revealed a 5 mm papillary thyroid microcarcinoma (PTMC), follicular variant, in the right lobe corresponding to the small hypoechoic nodule with rim calcification seen on presurgical ultrasonography. The PTMC was well encapsulated without capsular or vascular invasion and had no other aggressive features (Fig. 1D). The isthmus nodule and the two left-sided lesions that were inconclusive on FNA biopsy were characterized as nodular hyperplasia without atypia.
Immunostaining of the PTMC for Hector Battifora mesothelial antigen-1 (HBME-1) was strongly positive in a significant portion of the nodule. Galectin-3 (GAL3) and cytokeratin-19 (CK19) were negative. Further studies of tumor aggressiveness, including the cyclin D-1 immunostain and the BRAF V600E mutation, were negative.
After thyroidectomy, the patient was placed on levothyroxine replacement therapy. She underwent recombinant human TSH-stimulated whole-body I-131 uptake scan (I-131 WBS) that showed residual thyroid tissue in the thyroid bed but no focus of thyroid tissue elsewhere. Stimulated Tg measured 1.8 ng/mL with simultaneous undetectable Tg antibody.
Both the thyroid PTMC and adrenal thyroid rest were reviewed by consultant pathologists, with unanimous agreement of benign ectopic thyroid tissue located in the adrenal and incidental, unrelated PTMC. The patient was found to have Stage I micropapillary thyroid cancer and treated with suppressive doses of levothyroxine to a TSH goal of 0.1–0.5 μIU/mL. She will be followed with serial ultrasonography and thyroglobulin levels and will not be given I-131 ablative therapy.
Discussion
PTMC: a growing disease burden
The World Health Organization and the ATA describe microcarcinoma of the thyroid gland as any tumor measuring <1 cm in greatest diameter (1,2). This diagnosis is common, as 10%–20% of thyroid cancer diagnosed currently fall under the heading of microcarcinoma (3). In addition, there are likely many more cases that go undiagnosed, with some autopsy studies quoting an incidence of 5%–35% (4 –6). Because of advances in ultrasonography detection of these tumors and other possible undefined reasons, the incidence of thyroid microcarcinoma continues to rise, with most tumors identified as PTMC (7).
Most micropapillary thyroid tumors are not aggressive and can be surgically cured with total or near-total thyroidectomy. Still, local and distant metastases have been described (8 –13), most often to the lymph nodes, lung, and bone. The prevalence of distant metastasis in PTMC is reported at 0.2%–3% with a mortality rate of 0.2%–1% (8,10). Adrenal metastases are rare in larger papillary thyroid carcinoma (14,15), and have never been described in PTMC.
Aggressive characteristics of PTMCs
Several tumor characteristics have been reported to be associated with increased tumor aggressiveness. Unifocal disease has been thought to be less aggressive than multifocal disease, with multiple reports showing an increased risk of lymph node metastases and distant metastases in multifocal tumors (1,8,12). In addition, tumor size <8 mm has been associated with a very low prevalence of metastases (16,17). Cervical lymph node involvement is also predictive of metastatic potential and recurrence (18). Our patient had only one small focus of disease (5 mm) and no evidence of lymph node involvement by preoperative neck ultrasonography, intraoperative direct lymph node observation, or by postoperative thyrogen-stimulated thyroglobulin and I-131 WBS. Other benign features included a well-defined capsule without tumor invasion.
The usefulness of immunohistochemistry in determining metastatic potential of microtumors
There have been multiple reports citing the utility of positive GAL3, fibronectin-1 (FN1), cbp/p300 interacting transactivators with glutamic acid [E] and aspartic acid [D]–rich c-terminal domain, 1 (CITED1), HBME-1, and CK19 immunohistochemistry in determining malignant potential in thyroid nodules (19 –22). One report cited a 95% sensitivity for thyroid cancer (whether papillary, follicular, Hurtle, or anaplastic) if the tumor was positive for co-expression of multiple proteins and a 96% specificity for a benign tumor if all stains were negative (20). The thyroid tissue found in the adrenal gland stained positive for thyroglobulin, but was negative for HBME-1 and GAL3 and equivocal for CK19, making metastatic disease less likely. The PTMC itself stained strongly positive for HMBE-1 but was negative for GAL3 and for CK-19, suggesting a difference in immunophenotype between the two thyroid foci.
Cyclin D-1 immunostaining was also performed on the PTMC to help determine tumor aggressiveness and likelihood of metastatic disease. One study showed that cyclin D-1 protein overexpression helped to predict metastatic behavior in thyroid papillary microcarcinoma (23). Multiple other studies have shown increased tumor aggressiveness with this marker in several other forms of cancer (24 –26). According to their study criteria, tumors were considered positive for cyclin D-1 overexpression if there was moderate to intense nuclear staining (>10% of tumor cells) and if there was diffuse distribution of positive cells within the tumor (23). Our patient's tumor had some faint nuclear staining in <5% of thyroid cells in a localized distribution and, therefore, was considered a negative expressor of cyclin D-1.
BRAF mutations have been linked to more aggressive tumor behavior in papillary thyroid carcinomas, with increased metastatic potential compared to tumors with RET/PTC rearrangements, RAS mutations, or other mutations of the mitogen activated protein kinase pathway (MAPK) (27). Multiple studies examining BRAF mutations (especially the T1799A point mutation) in thyroid carcinoma have reported a significant association with lymph node spread, extrathyroidal invasion, and distant metastasis (28 –31). Our patient's primary PTMC did not have a BRAF mutation.
Current ATA guidelines (1) suggest consideration of these molecular markers (i.e., BRAF, RAS, RET/PTC, Pax8-PPARy, and galactin-3) in patients with indeterminate FNA cytology. It may also be worthwhile to consider expanding the use of these markers to a select group of patients with PTMC, as it may be useful in stratifying risk in the growing number of patients with thyroid microcarcinoma, some of whom may have risk for more aggressive tumors.
Ectopic thyroid tissue: metastasis or metaplasia?
Because of the benign tumor characteristics and negative metastatic work-up, it is highly unlikely that the PTMC found in the adrenal gland was a metastasis and is more consistent with ectopic thyroid tissue. Ectopic thyroid tissue in the adrenal has been described six other times in the Japanese literature, but has never been described in other patient populations (32 –36) (Table 1). One case reported by Hagiuda et al. (36) described ectopic thyroid tissue found after adrenalectomy for an aldosterone-producing adenoma, similar to the one we have presented. Although there may be an association between the two conditions, the apparent association between the two findings may be coincidental as adrenalectomy is most often performed for functional adrenal adenoma.
CT, computed tomography.
Most of the previously reported cases discovered thyroid tissue in a cystic adrenal lesion. Adrenal adenomas with ectopic thyroid rests were either discovered incidentally on imaging and were removed because of their size (3–4 cm), or they were surgically resected after a positive hormonal work-up (with hormonally active lesions found to be smaller in size) (Table 1). Despite finding thyroid tissue outside of the thyroid bed, thyroidectomy was not performed in the work-up of any of the previously reported cases. Instead, the thyroid gland was imaged with MRI, I-123 scintigraphy, CT scan, or ultrasonography, none of which revealed intrathyroidal lesions suggestive of malignancy.
Ectopic thyroid tissue is not unusual in the neck, mediastinum, or anywhere along the pathway of thyroid decent from the base of the tongue to the anterior trachea. Inexplicably, ectopic thyroid foci have also been found below the diaphragm in the abdomen. Ectopic thyroid has been reported in the gallbladder (37), ovary (38), small intestinal mesentery (39), pancreas (40), duodenum (41), vagina (42), inguinal region(43), porta hepatis (44), and the perisplenic area (45). Thyroid tissue found in the adrenal gland or in other intra-abdominal locations is hard to understand as far as currently available embryological information is concerned. For example, the adrenal gland develops from the ectoderm and the mesoderm, whereas the thyroid develops from the endoderm. Past explanations for why thyroid tissue can be found intra-abdominally include metaplasia, choristomatous tissue, over-descent of the hypoglossal duct remnant, or the development of teratoma. The etiology is unknown.
Conclusion
The discovery of concomitant PTMC and intra-adrenal ectopic thyroid tissue presented an interesting and unique diagnostic dilemma. Making the diagnosis was not only an important academic exercise, but was vital in determining the patient's need for radioactive iodine ablation. The latest ATA guidelines (1) for differentiated thyroid cancer treatment classify any subcentimeter intrathyroidal tumor as stage I, with recommendation against radioactive ablative therapy. In contrast, any distant metastasis, regardless of the initial tumor size, is classified as stage IV-C. For stage IV-C disease I-131 ablation is recommended as well as more vigorous and frequent surveillance.
As the prevalence of PTMC increases with improvements in imaging technology, it is likely that more cases of concomitant PTMC and ectopic thyroid tissue will emerge. Therefore, it may be prudent to determine the degree of PTMC aggressiveness with immunohistochemical staining, molecular markers, or other methods to determine whether extrathyroidal foci are likely metastases or simply benign ectopic tissue. Classifying PTMC metastatic potential will also help to guide management and longitudinal follow-up. Further research is needed to determine which markers are most useful in determining the aggressiveness of PTMC.
Footnotes
Disclosure Statement
The authors have no disclosures to declare and no competing financial interests exist. All authors attest to the accuracy and integrity of the article.