
Abstract
Background:
Thyroid and lung cancers, two malignancies with similar immunohistological characteristics, have vastly different biologic behaviors and treatment approaches. As thyroid cancers commonly spread to the lungs, metastatic thyroid cancer should be included in the differential diagnosis of a pulmonary lesion or lesions.
Summary:
A 54-year-old woman with a remote history of stage IV non-small cell lung cancer was found to have FDG avidity in the thyroid and right cervical lymph nodes. Subsequent ultrasonographic findings and FNA cytology led to a total thyroidectomy, bilateral central lymphadenectomy, and right modified radical lymph node dissection for primary thyroid cancer. Reviews and comparisons of the pulmonary and cervical surgical specimens revealed that the patient had been misdiagnosed for the previous 6 years; she had metastatic papillary thyroid cancer to the lung. The patient's original diagnosis of stage IV lung cancer was based upon the original lung biopsy showing positive thyroid transcription factor-1 (TTF-1) immunostaining. The original diagnosis was questioned because of her long survival when she was diagnosed with locally advanced papillary thyroid cancer. Further analyses of the immunohistological characteristics of both surgical specimens—including staining for TTF-1, thyroglobulin, CD57, S-100, and CEA—documented the correct diagnosis.
Conclusions:
A thorough understanding of the natural history and surgical pathology, including immunohistology, of lung and thyroid cancers is necessary for a correct and timely diagnosis and appropriate treatment. Because TTF-1 expression is seen in both thyroid and lung cancers, careful consideration should be given to both malignancies when evaluating patients with thyroid and pulmonary nodules.
Background
Lung cancer is the most common cause of cancer-related death worldwide and is associated with a 5-year overall survival of <15% (1). Even patients with stage IA and IB disease have a poor prognosis with 5-year overall survival of only 61% and 38%, respectively (2). Moreover, 5-year survival among patients with stage IV lung cancer is exceedingly rare; less than 1% of this population is expected to survive a long term.
In contrast, death from advanced differentiated thyroid cancer is uncommon. Five-year cancer-specific survival for stage I papillary and follicular thyroid cancers approaches 100% (3); adjusted 20-year survival for this population exceeds 96% (4). Even patients with stage IV disease have 50% survivorship at 5 years (3,5).
Patient Findings
A 54-year-old woman was referred for evaluation of abnormal FDG avidity in the right lobe of her thyroid gland that was found on a recent 18 FDG-PET/computed tomography scan. Additionally, the scan revealed two FDG-avid lymph nodes in the right lateral neck. Follow-up ultrasound examination of the neck revealed a heterogeneous mass in the thyroid isthmus that measured 22 mm in its greatest dimension and contained fine microcalcifications. In addition, suspicious lymphadenopathy was noted anterior to the right internal jugular vein.
The patient had no symptoms to suggest thyroid dysfunction and denied discomfort, dysphagia, dysphonia, or difficulty drawing a deep breath. She had no personal or familial history of thyroid pathology or radiation exposure. Her medical history was significant for stage IV non-small cell lung cancer (NSCLC), which was diagnosed by open lung biopsy in 2002. Over the next 20 months, she underwent 28 rounds of chemotherapy. In 2005, gefitinib and erlotinib (two monoclonal antibodies against EGFR) were added to her treatment regimen. She did not require radiation therapy.
In addition, she had three prior transient ischemic attacks, hypercholesterolemia, type 2 diabetes mellitus, asthma, renal dysfunction, depression, and dumping syndrome, a side effect of her aggressive chemotherapeutic interventions. Her surgical history included tonsillectomy, cholecystectomy, vaginal hysterectomy, and lumbar laminectomy in addition to the aforementioned open lung biopsy. As a result of her comorbidities, she qualified for and received disability benefits.
Physical examination revealed a firm, immobile 1-cm nodule just to the right of the thyroidal isthmus and a firm, mobile 1.5-cm lymph node high in the right lateral neck. Auscultation over her lung fields demonstrated no wheezes, but was remarkable for diffusely diminished breath sounds. She appeared older than her chronological age and had a Karnofsky performance status of 80% based upon her moderate symptoms with the performance of activities of daily living. Biochemically, she was euthyroid.
Fine-needle aspiration biopsy of the mass yielded cytology consistent with follicular neoplasm, although the possibility of metastatic NSCLC could not be definitively excluded. The patient underwent total thyroidectomy, bilateral central (level VI) lymphadenectomy, and right modified radical lymph node dissection. The surgical specimen revealed a 1.7-cm poorly differentiated papillary thyroid cancer (PTC) with extra-thyroidal and lymphovascular invasion. Fifteen lymph nodes were harvested, of which six (in both the lateral and central compartments) demonstrated metastatic foci of PTC. Her postoperative course was unremarkable, and she was discharged home on the first postoperative morning.
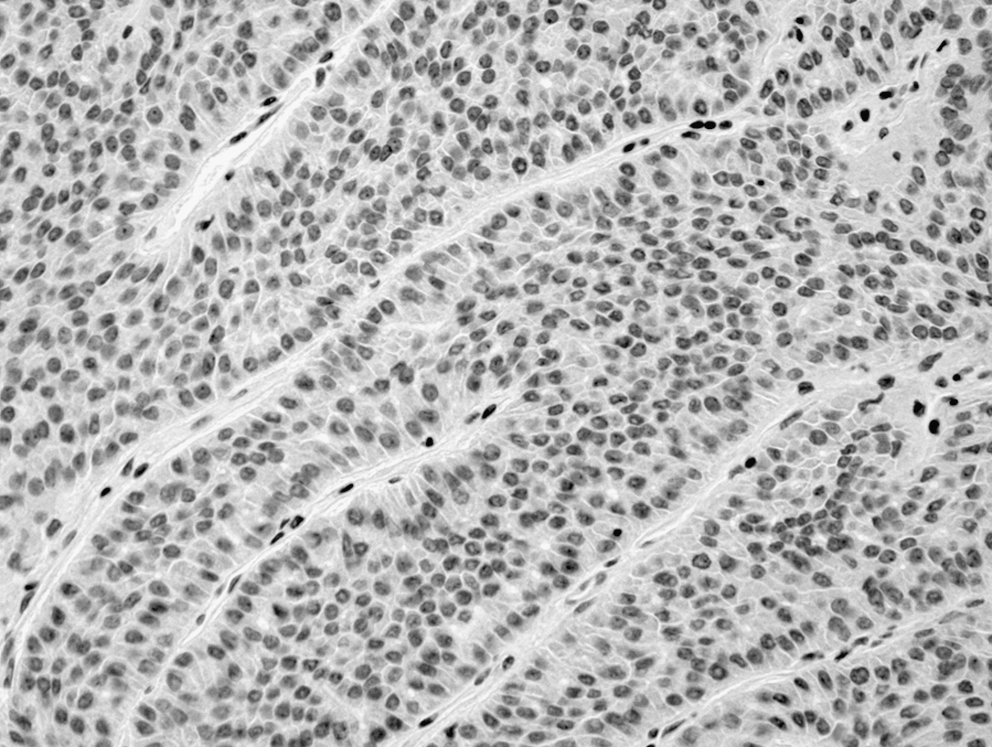
Because it was both extraordinary and unlikely that a patient with stage IV primary lung cancer would survive longer than 5 years and have tumor demonstrating radioiodine uptake, the patient's original diagnosis was questioned and her pathology slides were rereviewed. Slides of her pulmonary specimen were compared with the slides of her thyroid and cervical lymph node specimens and demonstrated clear similarities on hematoxylin–eosin staining (Fig. 1). Thereafter, tissue blocks of the pulmonary specimen were retrieved and stained for immunohistochemical markers, including thyroid transcription factor-1 (TTF-1), thyrogloblin, CD57, S-100, and CEA (Figs. 2 –6). Her TTF, thyrogloblin, and CD57 positivity and CEA negativity confirmed that the patient had originally been misdiagnosed; she did not have stage IV NSCLC but rather metastatic PTC all along.
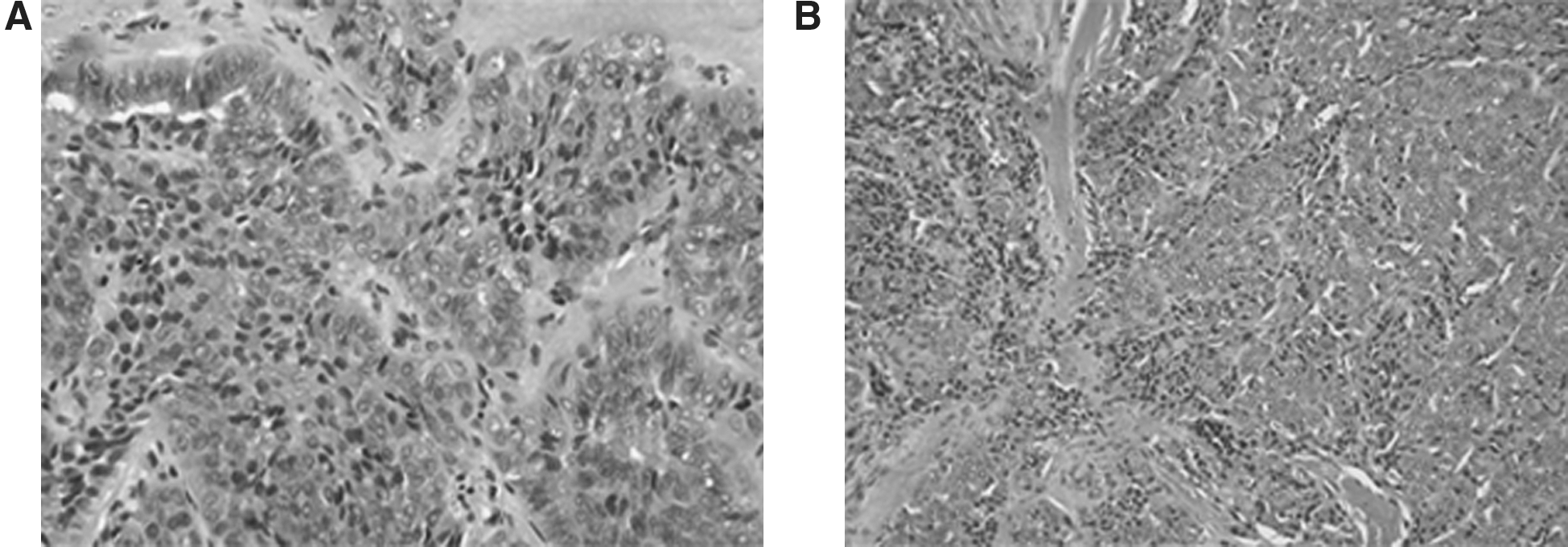
Micrographs of lung (
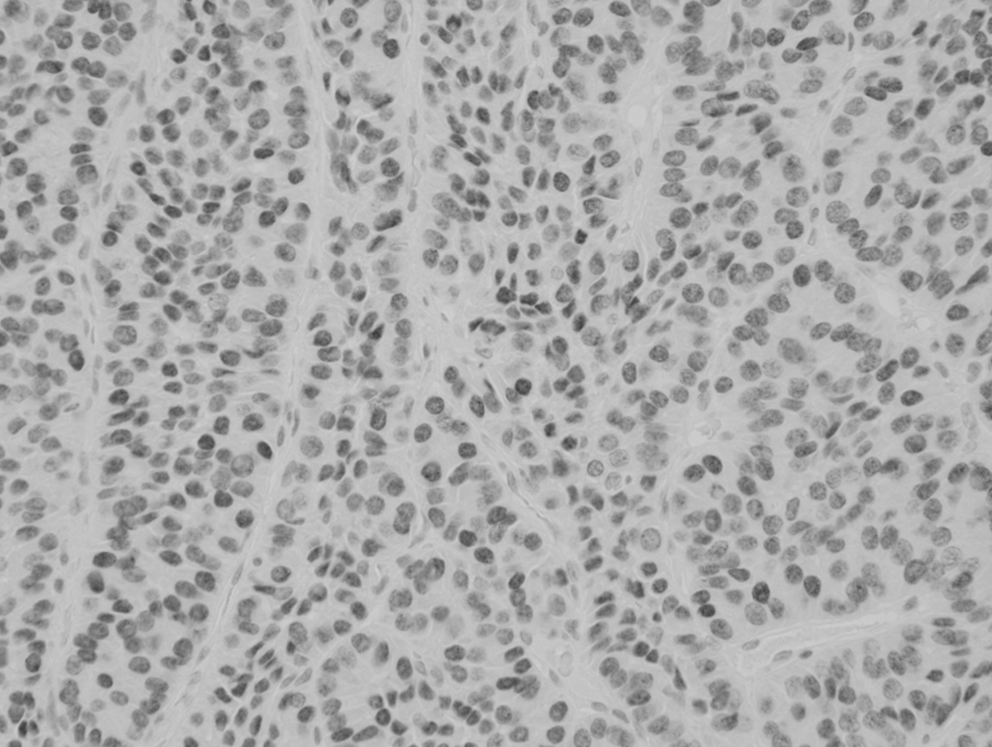
Micrograph of lung specimen (positive nuclear thyroid transcription factor-1 staining; 200 × magnification).
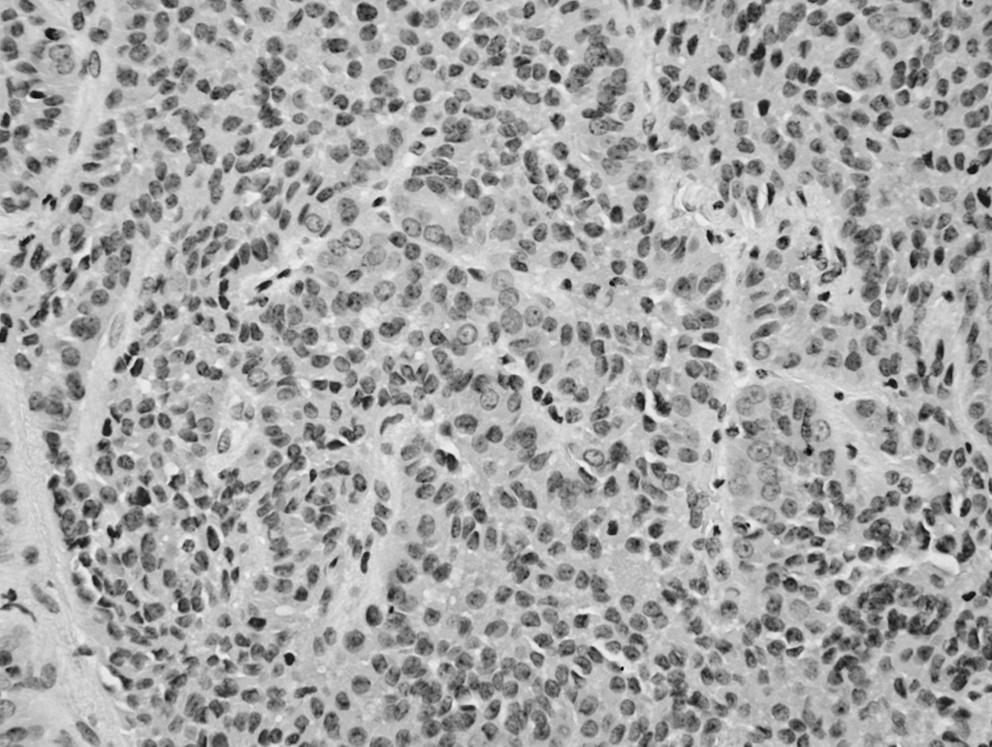
Micrograph of lung specimen (focally positive thyroglobulin staining; 200 × magnification).
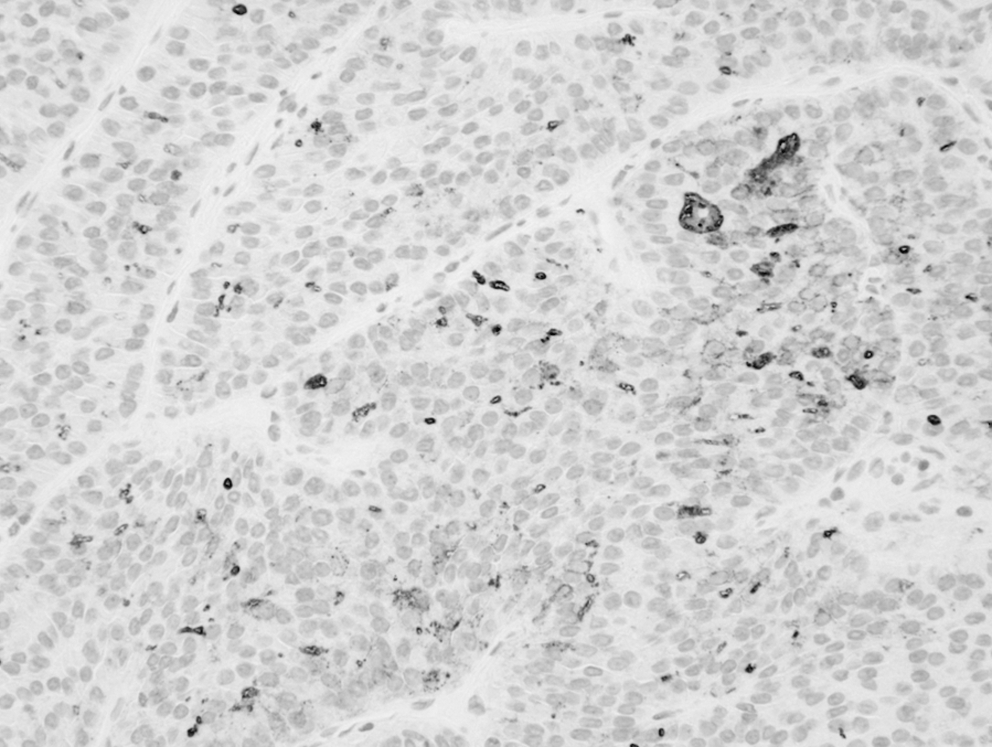
Micrograph of lung specimen (positive CD57 staining; 200 × magnification).

Micrograph of lung specimen (S-100 staining; 200 × magnification).
Micrograph of lung specimen (negative CEA staining; 200 × magnification).
The patient was subsequently treated with 205 mCi 131I. A posttreatment whole-body scan revealed uptake in the superior aspect of the right thyroid bed, but no uptake in the lungs or elsewhere. Serum thyroglobulin levels on levothyroxine suppression ranged from 1195 ng/mL after 131I treatment at 2 years ago to 642 ng/mL most recently. She feels reasonably well. Her ongoing complaints include chronic fatigue that has been attributed to chemotherapy-induced cardiomyopathy and shortness of breath. A recent 18 FDG-PET/computed tomography whole-body scan revealed FDG-avid nodules in both lungs.
Summary
To our knowledge, this is the first report of a patient who was originally diagnosed with a cancer of the lung but actually had metastatic papillary cancer. Using “lung neoplasm or cancer” and “thyroid neoplasm or cancer” as keywords, the Ovid Database was searched for all articles published between January 1996 and October 2010. Restricting the search to humans and the English language yielded 535 references, none of which described a similar case.
Differentiated thyroid cancer is among the most indolent solid-organ cancers known, and regional and distant metastases are not uncommon. Distant metastases develop in approximately 10% of patients with PTC and in up to 25% of patients with follicular thyroid cancer (6). Data from large cohorts of patients with distant metastases from differentiated thyroid cancers reveal that approximately half of these patients will have metastases limited to the lungs; only a 10th will have metastases outside the lung or bone (6,7).
In the presence of metastatic thyroid cancer, patient prognosis is influenced primarily by age, sites and burden of metastases, tumor size and local invasion, and the lesions' ability to concentrate 131I. Survival is longest in patients with diffuse microscopic metastases that concentrate 131I (and are therefore invisible on plain X-ray and only visible on 131I-nuclear imaging). Conversely, patients with macroscopic metastases that are 131I negative and FDG positive have the worst prognosis (8). Survival is intermediate for small, non–131I-avid metastases or large, 131I-avid metastases (7). This patient had a large mass, which was excised by open lung biopsy, and pulmonary uptake of FDG, but not 131I, portending a poor prognosis.
Tumor metastases to the thyroid gland are not uncommon; the most common malignancies to metastasize to the thyroid are renal cell, mammary, pulmonary, gastrointestinal carcinomas, and melanoma (9,10). Indeed, there are numerous reports of patients with lung cancers metastasizing to the thyroid gland (10 –13). Moreover, there are only a few reports of patients with both primary pulmonary and thyroidal primary malignancies, including one report of a primary thyroid cancer that metastasized to a primary lung cancer (14 –16).
The patient's initial diagnosis of stage IV NSCLC and subsequent 6 years of chemotherapy were based upon pathologic evaluation of an open lung biopsy specimen. Careful scrutiny and comparison of the patient's pulmonary and thyroidal specimens allowed for eventual accurate diagnosis. Immunohistological staining played a pivotal role in this course. TTF-1, a homeodomain transcription factor, plays a role in regulating genes expressed by the lung and thyroid, including genes required for the production of surfactant protein and thyroglobulin (17 –19). Therefore, specimens of either pulmonary or thyroidal origin stain positively for TTF-1. Thyroglobulin, on the other hand, is highly specific for the thyroid (20). Likewise, CD57, which is expressed by tumors of neuroepithelial origin, is highly sensitive for PTCs (21). Moreover, although S-100 expression is seen in other malignancies, it is fairly sensitive for PTCs (22). Finally, literature on the diagnostic and prognostic roles of CEA in lung cancer is well established (23). In the present case study, on immunohistochemical staining the patient's open lung biopsy specimen was TTF-1, thyroglobulin, CD57, and S-100 positive and CEA negative. Therefore, we favored primary thyroid cancer.
Conclusion
Careful review of disease presentation, in addition to the comprehensive immunohistochemical analysis of pathology specimens, can prevent misdiagnoses in patients with primary lung and thyroid carcinoma. We propose that all pulmonary biopsy specimens be stained for thyroglobulin in addition to TTF-1 to minimize the likelihood of misdiagnosis and inappropriate treatment.
Disclosure Statement
The authors declare that no competing financial interests exist.