
Abstract
Background:
Although overt thyrotoxicosis is associated with reduced insulin sensitivity (IS), the effects of subclinical thyrotoxicosis (SCTox) (i.e., suppressed serum thyroid-stimulating hormone with free thyroxine and tri-iodothyronine within the reference range) on glucose metabolism are not clear. SCTox may be of endogenous origin or due to ingestion of supraphysiological amounts of thyroid hormone. Our hypotheses were that reduced IS is present in SCTox and that the degree of reduction differs between SCTox of endogenous and exogenous origin.
Methods:
The study population consisted of 125 premenopausal, normal-weight women, divided into four groups: exogenous SCTox due to L-T4 treatment for benign goiter or hypothyroidism (SCTox-ExogG) (n = 53), endogenous SCTox (SCTox-Endog) (n = 12), exogenous SCTox due to L-T4 treatment for differentiated thyroid cancer (SCTox-ExogDTC) (n = 20), and finally euthyroid women (C) (n = 40) as a control group. After a mixed meal challenge, glucose and insulin were determined at baseline and 120 minutes later. IS was assessed by homeostasis model assessment of insulin resistance (HOMA-IR) index, quantitative IS check index (QUICKI), and 2 hours IS Avignon's index amended by Aloulou for mixed food. Secretion by pancreatic B-cells was calculated by HOMA-B index. Comparison among groups was done by analysis of variance followed by Tukey test. Linear regression analysis of T3 versus HOMA-IR was calculated.
Results:
IS was reduced in all types of SCTox when compared with C. All SCTox groups had significantly higher levels of insulin (baseline and postmeal) and HOMA-IR and lower values of QUICKI and Aloulou when compared with controls. SCTox-Endog, however, had higher baseline insulin levels and HOMA-IR and a lower QUICKI index than the rest of the SCTox groups. Although within the normal range, total T4, free T4, and T3 levels were also significantly higher in the SCTox groups than in euthyroids. In SCTox-Endog, T3/T4 ratio was increased above the rest of SCTox groups. A moderate linear relationship between T3 and HOMA-IR was found in the whole population.
Conclusions:
IR is associated with SCTox of either endogenous or exogenous origin. However, based on our findings of lower IS compared with the rest of the SCTox groups, the endogenous subclinical form might have an even larger metabolic impact.
Introduction
Subclinical thyrotoxicosis (SCTox) has been also associated with IR (7,8) in some but not all studies (9). Part of this controversy, despite a common biochemical definition, might lie in the heterogeneous nature of SCTox. Although suppressive thyroid-stimulating hormone (TSH) treatment with levothyroxine (L-T4) aimed at benign goiter shrinkage is of uncertain value, exogenous SCTox from this treatment is still frequently encountered. On the other hand, some differentiated thyroid cancer (DTC) patients do not have any alternative to L-T4 suppressive treatment. Further, the previously reported (10,11) positive relationship between DTC and IR may add to this lack of consensus. Finally, endogenous SCTox, resulting from longstanding autonomous nodular goiter or Graves' disease, also represents a potential source of IR with an unrecognized clinical impact.
As data about a possible association between SCTox and IR are controversial, we performed a study to look for differences in insulin sensitivity (IS) among euthyroid subjects, patients with SCTox of endogenous origin, and patients with goiter and thyroid cancer who had SCTox of exogenous origin.
Materials and Methods
Population
This study included 125 women who were nonobese (body mass index [BMI] <30), 18–55 years of age, and lived in an area that was currently iodine sufficient (12). They had consulted at our Endocrinology Center at Mendoza in the period from 2004 to July 2009. Exclusion criteria were pregnancy, smoking, severe liver or kidney disease, major depression, psychosis, treatment with metformin, lithium, beta blockers, amiodarone, antithyroid drugs, tri-iodothyronine, TRIAC, or iodine and women treated at doses below 50 μg per day of L-T4 (13). Women with known diabetes or those with fasting glucose serum levels greater than 125 mg/dL (14) or postprandial blood glucose greater than 150 mg/dL (15) were also excluded.
The population was divided into four groups: exogenous SCTox due to L-T4 treatment for benign goiter or L-T4 overdosage (SCTox-ExogG) (n = 53), endogenous SCTox (SCTox-Endog) (n = 12), exogenous SCTox due to L-T4 treatment for (SCTox-ExogDTC) (n = 20), and euthyroid women (C) as a control group (n = 40). The C group was composed of individuals undergoing evaluation for irregular menses (n = 6), health checkup (n = 10), pseudogoiter (n = 2), friend's advice (n = 5), excessive perspiration (n = 4), weight control (n = 9), hirsutism (n = 2), edema (n = 2) who were found to not have ongoing thyroid dysfunction, thyroid autoimmunity, or goiter. We defined SCTox as TSH levels <0.3 mU/L, free T4 <1.8 ng/dL, total T4 <12.0 μg/dL, and T3 <180 ng/dL.
After a mixed meal test, glucose and insulin were determined at baseline and 120 minutes later. IS was assessed by homeostasis model assessment of IR (HOMA-IR) index (16), quantitative IS check index (QUICKI) (17), and 2 hours IS Avignon's index amended by Aloulou for mixed meal (18,19). Secretion by pancreatic B-cells was calculated by the index of β-cell function derived from the homeostatic model (HOMA-B) (16).
This study was approved by the ethics committee of our institution. Written informed consent was obtained from all subjects before initiating the study.
Clinical and biochemical measurements
A clinical history and physical examination that included anthropometric measurements was performed in all participants. Patients were barefoot when weight and height were assessed. BMI was calculated as weight over height squared (kg/m2). All study patients had total T4, free T4, T3, TSH, and antithyroperoxidase (ATPO) levels assayed within 7 days before entry into the protocol. To make the diagnosis of goiter, an ultrasonogram was performed and thyroid volume was calculated. Thyroid volumes larger than 12 mL (20) and mixed or solid nodules larger than 5 or 3 mm in diameter, respectively, met the criteria for goiter.
After measuring baseline glucose and insulin levels, a standard mixed breakfast (812 calories, 66% from carbohydrate, 11% protein, and 22% fat) (15,21,22) was taken by the subjects. After breakfast the subjects rested until blood glucose and insulin were measured again at 2 hours after this meal. Insulin sensitivity and secretion were calculated using the following equations:
Aloulou index:
where SG = serum glucose (mg/dL) and SI = serum insulin (μIU/mL), measured at baseline (0) and 2 hours (2h).
Both QUICK (17) and HOMA-IR (16) are considered surrogates of central IS (23) and we used them to assess IR in the liver. Aloulou index, which takes into account the values of postprandial glucose and insulin levels, was used to assess peripheral glucose sensitivity (22, 23).
Normal values of postprandial blood glucose were considered to be 112 mg/dL or less. Glucose intolerance was defined by glucose levels of 113–150 mg/dL at 2 hours after the standard mixed breakfast (22). All blood samples were drawn after 12 hours of fasting without any medication. Except for the determination of glucose that was performed immediately, serum samples were frozen and stored until assay at −20°C.
Total T4, free T4, and T3 were all measured with a competitive chemiluminescent enzyme immunoassay method in solid phase (IMMULITE®; Siemens, Los Angeles, CA). Reference values for total T4 were 4.5–12.5 μg/dL; they were 0.7–1.8 ng/dL for free T4 and 90–180 ng/dL for total T3. TSH was measured with a noncompetitive chemiluminescent enzyme immunoassay method in solid phase (IMMULITE). Reference values for serum TSH were 0.3–4.5 mU/L. ATPO and antithyroglobulin (anti-TG) antibodies were assessed by a sequential enzyme immunometric assay chemiluminescent solid phase (IMMULITE). Reference values were less than 20 IU/mL for both TPO and TG antibodies. Insulin was measured by enzyme immunometric assay with a two-site chemiluminescent solid phase (IMMULITE). Reference values for 2 hours postprandial insulin were less than 10.0 mIU/mL. Glucose was measured by an enzymatic method using glucose oxidase/peroxidase (Roche Diagnostics, Mannheim, Germany); reference values were 70–110 mg/dL. The measurement of glucose was performed in collected plasma from blood with EDTA/fluoride, so as to avoid errors by enzymatic destruction of blood glucose (glycolysis).
Statistical analysis
Statistical analysis was performed with SPSS software package (SPSS, Chicago, IL). Values are presented as mean ± SD. Comparison among groups was done by analysis of variance (ANOVA) followed by Tukey test. Transformations were used to achieve homogeneity of variance: “log” in the case of basal serum insulin and “ranks” for postprandial serum glucose and insulin levels and HOMA-IR, QUICKI, and Aloulou indexes. Weighted least squares were used for TSH and T3/T4. Linear regression analysis of T3 versus HOMA-IR was calculated. Differences were considered significant at p less than or equal to 0.05.
Results
The SCTox-ExogG group was comprised of 20 patients with “multinodular goiter,” and of them, fine-needle aspiration biopsy (FNAB) was reported as colloid or follicular lesion. They were being treated with L-T4 in doses that suppressed serum TSH. Their classification as meeting criteria for SCTox was confirmed at baseline and 3 months later when they were taking the same dose of L-T4. There were 13 patients with “diffuse goiter” who were assigned and met the same criteria for SCTox, with whom we proceeded in the manner described earlier, but without requirement of FNAB, and 19 patients who were “hypothyroid without goiter” who were under suppressive doses of L-T4 at presentation and, despite being counseled a reduction of L-T4 dose, 3–6 months later still had TSH levels that were suppressed. In the SCTox-Endog group, none of the patients was on L-T4, antithyroid drugs, or amiodarone. The underlying etiology of endogenous SCTox was Graves' disease (thyrotropin receptor antibody+) (n = 6), toxic nodular goiter (n = 1), and toxic multinodular goiter (n = 2) or Hashi-thyrotoxicosis (n = 3). SCTox-ExogDTC patients had been under suppressive doses of L-T4 for a variable period of >3 months. Eighty percent of this group had a pathological diagnosis of papillary cancer, whereas only 20% had a follicular type.
There were no significant differences in age or BMI among the four studied groups. Age and BMI were, respectively, 40.0 ± 10.7 years and 24.8 ± 2.03 for SCTox-ExogG, 36.0 ± 5.44 years and 24.9 ± 2.1 for SCTox-Endog, 40.8 ± 10.5 years and 24.1 ± 2.6 for SCTox-ExogDTC, and 39 ± 10 years and 25.1 ± 2.7 for C.
TSH levels were significantly decreased in all SCTox when compared with euthyroids. Although total T4, free T4, and T3 levels were within normal parameters, all SCTox groups had significantly higher hormone levels than the euthyroid group. The T3/T4 ratio was analyzed and the SCTox-Endog group showed a significantly higher ratio than SCTox-ExogG and SCTox-ExogDTC groups (p < 0.05) (Table 1). L-T4 dose was 120 ± 31 μg/day in the SCTox-ExogG group and 148 ± 35 μg/day in SCTox-ExogDTC.
p < 0.05 between the control group and the SCTox groups by Tukey post hoc analysis.
p < 0.05 between the SCTox-Endog group and the rest of the SCTox groups by Tukey post hoc analysis.
SCTox-ExogG, subclinical thyrotoxicosis due to levothyroxine (L-T4) treatment for benign goiter or L-T4 overdosage; SCTox-Endog, endogenous subclinical thyrotoxicosis; SCTox-ExogDTC, exogenous subclinical thyrotoxicosis due to L-T4 treatment for differentiated thyroid cancer; C, euthyroid women; ANOVA, analysis of variance.
Table 2 shows baseline and postprandial blood glucose and insulin levels as well as IS parameters: HOMA-IR, QUICKI, and Aloulou indexes and the insulin secretion variable (HOMA-B) of all groups. All studied parameters were significantly different by ANOVA (Table 2). According to Tukey's post hoc test, except for HOMA-B and for baseline and postprandial glycemia (only for SCTox-ExogG), the rest of the variables were significantly different between the SCTox groups and the control group (Table 3). SCTox-Endog, however, had higher baseline serum insulin and HOMA-IR and lower QUICKI levels than the rest of the SCTox groups (Table 3).
p < 0.05 between the control group and the SCTox groups by Tukey post hoc analysis.
p < 0.05 between the SCTox-Endog group and the rest of the SCTox groups by Tukey post hoc analysis.
HOMA-IR, homeostasis model assessment of insulin resistance; QUICKI, quantitative insulin sensitivity check index; ns, not significant.
B, baseline; Pp, postprandial.
The regression analysis suggested a moderate linear relationship between T3 and HOMA-IR in the whole population (r: 0.54, r 2: 0.29, p < 0.0001; Fig. 1). If we excluded DTC patients, the association was stronger (r: 0.66, r 2: 0.44, p < 0.0001).
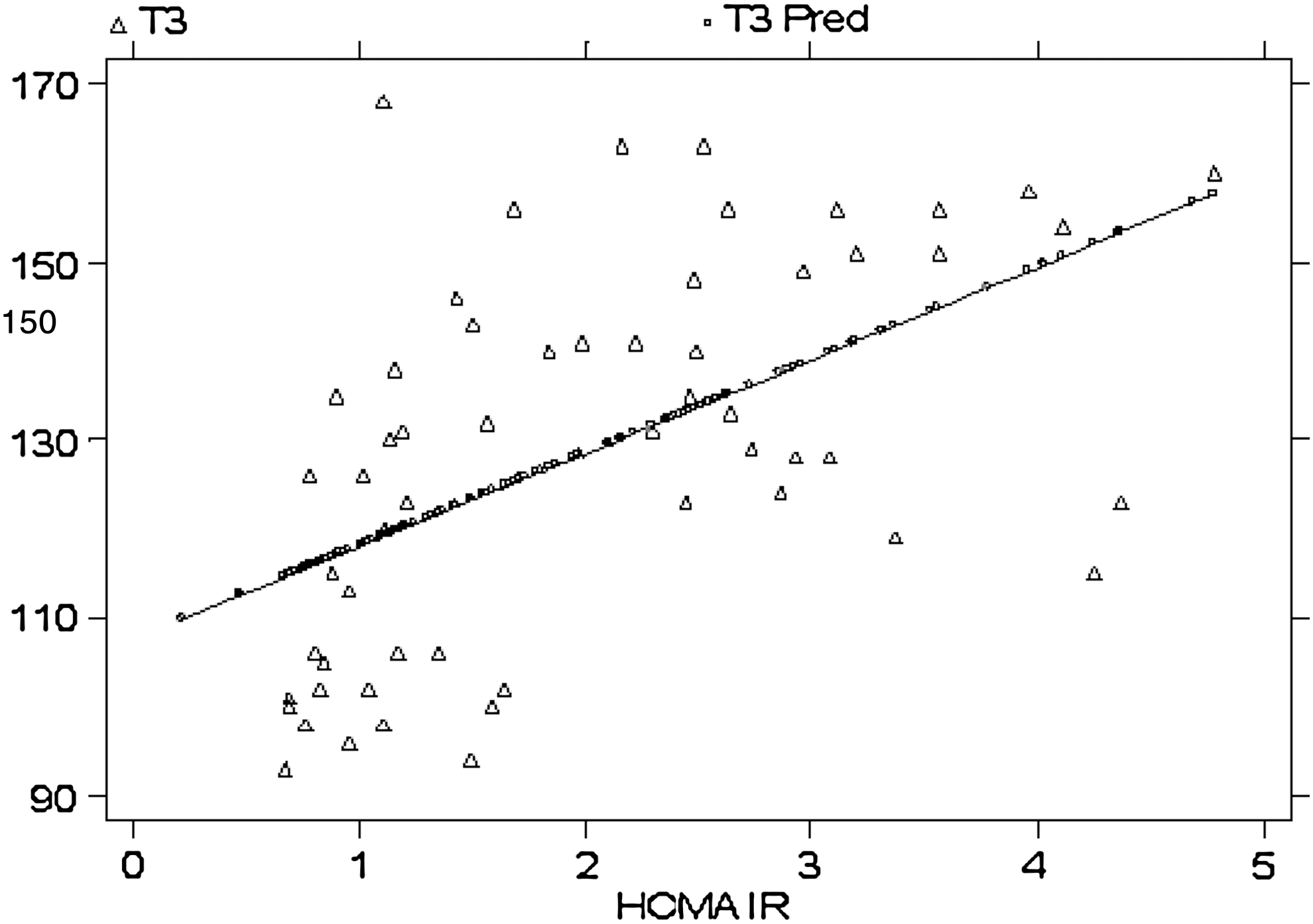
Linear regression of T3 versus homeostasis model assessment of insulin resistance for all patients. Observed values (T3) and predicted values (T3 pred) are plotted.
Discussion
Our findings confirm that SCTox is characterized by lower IS, as it had been formerly described for overt thyrotoxicosis (24,25). Further, all types of SCTox share this pattern.
Yavuz et al. (7) have reported that whole-body IS during an oral glucose tolerance test (OGTT) is significantly decreased in patients with euthyroid multinodular goiter after 24 weeks of suppressive doses of L-T4. In line with their findings, we observed that treatment of nodular goiter or L-T4 overdosage in hypothyroid patients results in both decreased central and peripheral glucose sensitivity when compared with euthyroid controls. Conversely, insulin secretion by pancreatic B-cells is preserved as reflected by similar HOMA-B levels between the groups.
With regard to SCTox in thyroid cancer patients, all IS parameters were also in a deteriorated state in comparison with the euthyroid group. In contrast, Heemstra et al. (9) found that restoration to euthyroidism in DTC patients with previous L-T4-induced SCTox had no influence on glucose metabolism. They postulated that long-term L-T4 treatment (>10 years) can bring along an adaptative state. This concept of adaptation is not consistent with our previous observation in DTC patients in whom the proportions of IR (defined as HOMA-IR >2.5) at diagnosis and several years (>5) thereafter were similar (10). An alternative explanation, both to their negative findings within a group of DTC with differential treatment and also to our results in the present study, is that some thyroid cancer patients may be insulin resistant per se and not only as a consequence of L-T4 treatment. In support of this idea we found that, after excluding DTC patients, the association between T3 and HOMA-IR became stronger. Several lines of research have confirmed that IR is associated with cancer (26) and that this concept also holds true in DTC (10,11).
We also found more IR in the SCTox-Endog group of patients compared with the euthyroid group. No strong background for IR studies in endogenous SCTox exists in the literature. Very recently, however, Maratou et al. (8) reported that the sensitivity of glucose metabolism in endogenous subclinical thyrotoxic patients to insulin in vivo (measured by an OGTT) and in vitro (by measuring insulin-stimulated rates of glucose transport in isolated monocytes) was lower than a euthyroid control group. Our results, with a mixed meal test, a physiologic stimulus to assess insulin secretion and action, agree with these findings.
Probably, the most interesting aspect of our study is that we were able to compare the effects on glucose metabolism of SCTox according to etiology. Although both exogenous and endogenous SCTox were related to lower IS when compared with euthyroid condition, it was SCTox-Endog the most affected group. As mentioned earlier, thyrotoxicosis is linked to IR. According to the higher T3/T4 ratio found in these patients and the moderate linear relationship encountered between T3 and HOMA-IR in the whole population, it could be hypothesized that the tissues of the patients with endogenous SCTox were relatively more thyrotoxic.
In conclusion, IR is present in all subclinical thyrotoxic patients. L-T4 suppressive treatment for nodular goiter and DTC, or iatrogenic SCTox, can all lead to IR. Endogenous SCTox is, however, the most delicate situation.
Footnotes
Disclosure Statement
The authors have nothing to disclose.