
Abstract
Background:
Whole-body scans (WBSs) based on diagnostic or therapeutic doses of I-131 can visualize metastatic lesions in thyroid cancer patients who have undergone total thyroidectomy. However, a variety of unusual lesions may cause false-positive results, and therefore, careful evaluation of abnormal scans is imperative to avoid unnecessary surgical removal or high-dose radioiodine treatment. Here, we report a patient with pulmonary aspergilloma mimicking metastasis of thyroid cancer on WBS.
Summary:
A 53-year-old woman with papillary thyroid cancer stage III (T1N1aM0) who had undergone total thyroidectomy and 150 mCi of radioiodine treatment for remnant ablation was found to have focal intense radioiodine accumulation in the left lung field by WBS, suggestive of pulmonary metastasis, at 5 days after I-131 administration. Whole-body F-18 fluorodeoxyglucose (FDG) positron emission tomography (PET)/computed tomography (CT) and Tc-99m methoxyisobutyl isonitrile scans showed no remarkable tracer accumulation at the pulmonary nodule. An enhanced chest CT scan demonstrated a nonenhancing pulmonary nodule with an air-crescent sign suggestive of pulmonary fungus ball. A subsequent blood test for precipitating antibodies to Aspergillus antigens produced a result of 29.9 U/mL (reference range: 0–8 U/mL). The patient was clinically diagnosed as having pulmonary aspergilloma based on serologic test and radiologic imaging results.
Conclusion:
Extreme caution should be exercised when interpreting abnormal radioiodine WBS findings when the serum thyroglobulin is normal and imaging characteristics indicate a benign condition. Pulmonary aspergilloma is a cause of a false-positive lesion when radioiodine WBSs are performed.
Introduction
Whole-body scan (WBS) with diagnostic or therapeutic doses of I-131 can visualize metastatic lesions in thyroid cancer patients who have undergone total thyroidectomy. However, a variety of unusual lesions may cause false-positive results, and therefore, abnormal scans must be carefully evaluated to avoid unnecessary surgical removal or high-dose radioiodine treatment (3 –7).
Here, we present a case of papillary thyroid cancer with pulmonary aspergilloma mimicking metastasis, which demonstrated unusually high radioiodine accumulation.
Patient
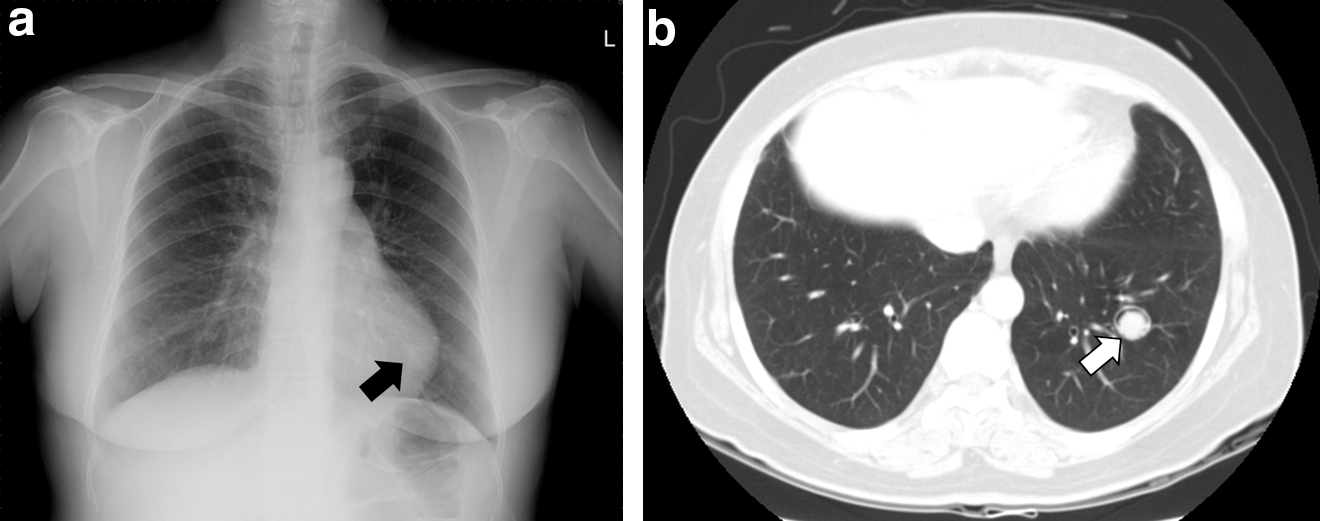
A 53-year-old woman was referred to our nuclear medicine department for high-dose radioiodine ablation. She had previously had a total thyroidectomy and histologic evaluation had revealed a 3-mm papillary microcarcinoma with multiple metastases to cervical lymph nodes (Delphian, isthmic, and left cervical level VI lymph nodes). Her primary disease stage was III (T1N1aM0). After 5 weeks of thyroid hormone withdrawal, thyrotropin was 51.9 μIU/mL, triiodothyronine 0.2 ng/mL, free thyroxine 0.1 ng/dL, thyroglobulin 0.6 ng/mL, and antithyroglobulin antibody 113.8 U/mL (reference range: 0–35 U/mL). At the time serum thyrotropin was elevated, she took a single I-131 capsule of 150 mCi for ablation purposes. A WBS at 5 days after I-131 administration revealed physiologic radioiodine accumulations in the thyroid bed, oral cavity, and liver. These were considered to be related to, respectively, I-131 accumulation in the thyroid remnant and salivary glands and metabolism of radioiodinated thyroglobulin in the liver. In addition to these usual uptakes, intense focal uptake of radioiodine was observed in the left lung field, suggesting pulmonary metastasis from the papillary thyroid cancer (Fig. 1). Whole-body F-18 fluorodeoxyglucose (FDG) positron emission tomography (PET)/computed tomography (CT) visualized a 14-mm nodule without significant FDG uptake in the left lower pulmonary lobe, and a whole-body Tc-99m methoxyisobutyl isonitrile (MIBI) tumor scan showed no remarkable tracer accumulation at the pulmonary nodule (Figs. 2 and 3). Enhanced chest CT demonstrated a 17-mm cavitary lesion with a 13-mm, nonenhancing mural nodule in a dependent portion of the cavity, which produced the pathognomonic air-crescent sign of pulmonary aspergilloma (Fig. 4). A subsequent blood test for precipitating antibodies to Aspergillus antigens produced a result of 29.9 U/mL (reference range: 0–8 U/mL). Although she had a history of hemoptysis, the patient had no respiratory symptoms, such as a cough or sputum production. Without histologic confirmation, the patient was clinically diagnosed to have pulmonary aspergilloma based on radiologic features coupled with serologic evidence of precipitating antibodies to Aspergillus species.
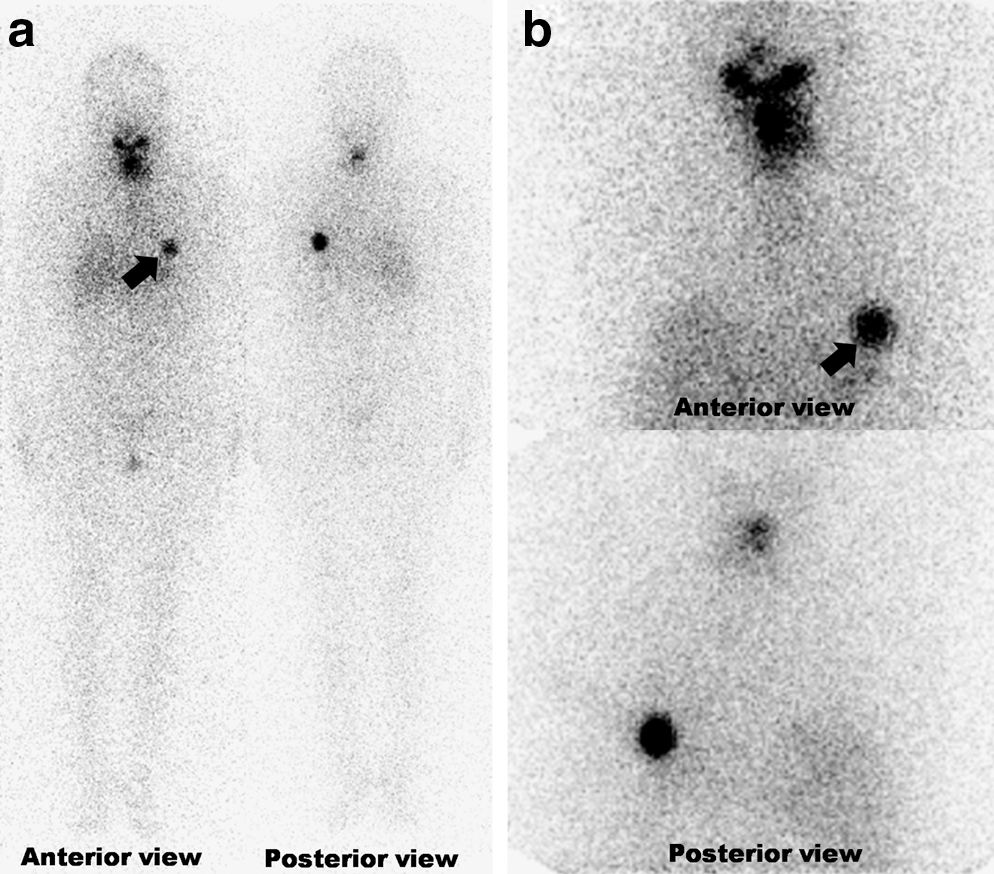
Whole-body scan obtained at 5 days after oral administration of I-131 (150 mCi) showing physiologic radioiodine accumulations in the thyroid bed, oral cavity, and liver, and pathologic intense radioiodine accumulation (arrow) in the left lung field, suggesting pulmonary metastasis from papillary thyroid cancer.

Whole-body F-18 fluorodeoxyglucose (FDG) positron emission tomography (PET)/computed tomography (CT) scan showing a nodule without significant FDG uptake (arrow) in the left lower pulmonary lobe.

Whole-body Tc-99m methoxyisobutyl isonitrile tumor scan showing physiologic tracer accumulations in myocardium, gall bladder, kidney, and bowels, but no remarkable abnormal tracer uptake in the left lung field.
Discussion
Differentiated thyroid cancers arising from follicular cells not only retain the appearance of thyroid follicular cells but also retain their iodine trapping function, and thus, WBS based on a diagnostic or an ablation I-131 dose provides information about residual thyroid tissue and distant metastatic lesions (3).
The correct interpretation of radioiodine WBSs is crucial for the proper management of patients with differentiated thyroid cancer. Misinterpretations of physiologic or benign pathologic uptakes of radioiodine or contamination as being metastatic lesions of thyroid cancer could lead to unnecessary surgery or the administration of therapeutic I-131 resulting in unnecessary fruitless radiation exposure (3,5,7). Many false-positive findings have been documented in radioiodine scans, but radioiodine uptake by fungus balls related to aspergilloma is extremely rare and typically the subject of single case reports (4,8).
Iodine uptake by aspergilloma has been attributed in part to the endotoxins or enzymes released locally by the fungus, which cause cellular damage to the inner lining of the fungus ball cavity (8). Manka-Waluch et al. reported that they misdiagnosed pulmonary aspergilloma (finally confirmed by histologic study) as lung metastasis from thyroid cancer. They administered therapeutic dose of I-131 three times to their patient and interestingly found that the size of the aspergilloma reduced (4). Rumbak et al. applied nonradioactive iodine to aspergilloma cavities to control hemoptysis in patients with pulmonary aspergilloma and observed radiographic clearance in 3 of 12 cases (9). These findings indicate that iodine can interact directly with or even enter aspergilloma.
Park et al. reported that in 6.3% of functioning metastases from differentiated thyroid cancer, the serum thyroglobulin level was normal, but there was radioiodine uptake in the WBS (10). However, even though some patients with recurrent thyroid cancer can have a normal thyroglobulin level with a positive radioiodine WBS, it is particularly important that the reason for the positive WBS be determined carefully and with additional imaging procedures in patients with this combination of findings, to avoid inappropriate treatment (8,10).
The typical radiographic appearances of pulmonary aspergilloma are of a rounded mass sitting inside a thick-walled cavity with surrounding air, which is responsible for the so-called “air-crescent sign” (11,12). Because diagnostic CT findings of Aspergillus-related lung lesions can be compromised by the complex conditions caused by aspergilloma or other pulmonary aspergilloses (12), these diseases should be considered when a lung lesion shows radioiodine uptake by radioiodine WBS.
A variety of benign pathologies, such as inflammatory processes and benign tumors, can accumulate FDG, and cancers with a low glucose metabolic rate (e.g., bronchoioloalveolar carcinoma and mucinous adenocarcinoma) and cancers with poor avidity for FDG (e.g., prostate cancer and hepatocellular cancer) may show minimal or no FDG accumulation (13 –15). Although F-18 FDG PET/CT has the inherent limitations of false-negative and false-positive findings for the detection of malignant lesion, its sensitivity and specificity are high enough in a number of malignancies, which include thyroid cancer, and thus, it has rapidly become a widely used imaging modality for initial staging, therapy monitoring, and the detection of metastasis and the surveillance of recurrence (15 –17). In our patient, the FDG PET/CT result was true negative for malignancy.
Tc-99m MIBI scans can also detect metastases from thyroid cancer with high sensitivity. Campenni et al. suggested that this modality should be viewed as a first-level diagnostic procedure, along with serum thyroglobulin determination and neck ultrasonography, for the early postsurgical evaluation of differentiated thyroid cancer patients before radioiodine therapy (18). In our patient, the Tc-99m MIBI result was true negative for malignancy.
Our case emphasizes that extreme caution is needed when interpreting abnormal radioiodine WBS findings in thyroidectomized thyroid cancer patients with a normal thyroglobulin level and benign characteristics on imaging studies. Further, we advocate that pulmonary aspergilloma be considered a cause of a false-positive lesion for radioiodine WBS.
Footnotes
Acknowledgments
This work was supported by the Nuclear Research & Development Program of National Research Foundation of Korea (NRF) funded by Ministry of Education, Science, and Technology (MEST) and the Grant of the Korean Ministry of Education, Science, and Technology (The Regional Core Research Program/Anti-aging and Well-being Research Center).
Disclosure Statement
The authors have nothing to disclose and claim that no competing financial interests exist.