
Abstract
Background:
Invasive fibrous thyroiditis (IFT) is the rarest form of thyroiditis, and reports are often limited to case reports and small case series. In this study, we aimed to summarize our institutional experience with IFT since 1976.
Methods:
We retrospectively reviewed the cases of all patients with IFT evaluated at Mayo Clinic, Rochester, Minnesota, from 1976 through 2008, with special emphasis on clinical presentation, associated risk factors, associated comorbid conditions, complications, and treatment.
Results:
Twenty-one patients met our inclusion criteria of (i) IFT confirmed by pathologic review at our institution and (ii) evidence of extension of fibrosis outside the thyroid capsule. Most patients (17, 81%) were women (mean age, 42 years). Presenting symptoms included pain (24%), dysphagia (33%), vocal cord paralysis (29%), and tracheal narrowing (48%). Three patients had associated hypoparathyroidism. Sixteen (76%) had a history of tobacco use, and 10 (48%) were current smokers. Fibrosing mediastinitis was present in four, orbital fibrosis in one, retroperitoneal fibrosis in three, and pancreatic fibrosis in one (38% had extracervical fibrotic processes). Eighteen patients had partial thyroidectomy, 7 (39%) of whom had surgical complications involving vocal cords and parathyroid. Two required tracheostomy. Thirteen had corticosteroid therapy; six received tamoxifen. There was no cause-specific mortality, and the fibrotic process stabilized or partially resolved in all patients.
Conclusions:
IFT often is associated with a systemic extracervical fibrotic process and tobacco use. Attempted thyroid resection often results in postoperative complications. Long-term follow-up showed no deaths from IFT and showed stability of the thyroiditis.
Introduction
The cause of IFT remains unclear. A clear association has been observed, however, between IFT and autoimmunity (5,6). Many authors have suggested that IFT and similar disorders—such as retroperitoneal fibrosis, fibrosing mediastinitis, and orbital pseudotumor—are manifestations of the same underlying systemic disease, because various manifestations frequently occur in the same patient (7). Multifocal idiopathic fibrosclerosis is among several terms used to describe this systemic process. IFT has no standardized treatment, although most patients are treated with corticosteroids (8), tamoxifen (more recently) (9), or both (8). Objective data on these treatments, however, are lacking.
As a referral institution, Mayo Clinic has experience with a relatively large group of patients with IFT. Here, we summarize our experience with all cases of IFT evaluated at our institution since 1976, with special emphasis on clinical presentation, associated risk factors, associated comorbid conditions, treatment, and complications of both disease and treatment.
Methods
Case identification
After obtaining Mayo Clinic Institutional Review Board approval, we screened our patient database for cases of all Mayo Clinic patients with IFT from 1976 through 2008. All included patients had appropriate research authorization. Paper records were screened using HICDA (hospital adaptation of the International Classification of Diseases) billing codes for Riedel thyroiditis, chronic thyroiditis, thyroiditis nonspecified, and fibrosis. The codes were cross-referenced with the keywords “fibrosis,” “fibrous,” “sclerosing,” and “thyroid,” to further limit the results. Requirements for patient inclusion in the study were (i) a diagnosis that was confirmed by open biopsy and (ii) having appropriate authorization to participate in research. Patients who received a diagnosis at an outside facility were included if their diagnosis was confirmed by review of specimens by a pathologist at our institution. Only cases with fibrosis extending outside the thyroid capsule were included.
Data extraction and analysis
From the medical records, we extracted data on clinical presentation, results of physical examination, comorbid conditions, results of laboratory and imaging studies, treatment, and disease outcomes. We recognized that certain outcomes such as thyroid, parathyroid, and vocal cord function could be affected by surgical intervention at the time of diagnosis, and therefore we analyzed these types of parameters both before diagnosis and during the subsequent follow-up period. Descriptive statistics were used to summarize the data. Follow-up period was calculated from the first and last Mayo Clinic visits.
A total of 38 patients met our initial search criteria. Of these, 17 patients were excluded: one patient had indeterminate pathologic findings; three did not have pathologic review at Mayo Clinic; and 13 were excluded after chart review did not support a definite diagnosis of IFT. Of these 13 patients, 6 had been referred for possible IFT, but the pathologic review and the clinical scenario indicated an alternate diagnosis: 1 patient each had histiocytosis X, combined papillary and squamous cell carcinoma, Graves' disease, and papillary thyroid cancer, and 2 had fibrotic lymphocytic thyroiditis or Hashimoto's thyroiditis, 1 of whom had localized neck fibrosis with Hashimoto's thyroiditis but no definite intrathyroidal IFT.
Results
Of the 21 patients included for analysis, 17 (81%) were women. The mean age at diagnosis was 42 years (range, 23–65 years). Mean follow-up was 9.5 years (median, 4.5 years). Diagnosis was made at a mean (SD) of 10.2 (10.6) months after onset of symptoms and 23.4 (29.9) months after onset of observable signs, which included goiter. Details of presenting signs and symptoms were variably reported. Symptoms included pain in five patients (24%), pressure symptoms in five (24%), dysphagia in seven (33%), and dyspnea and airway compromise in nine (43%). Three patients (14%) reported a fever, and six (29%) had vocal cord paralysis. Ten patients (48%) had tracheal narrowing by imaging. On initial examination at Mayo Clinic, all 21 patients had a palpable, enlarged, firm, fixed thyroid.
Association with smoking
Data on prior smoking history were available for 20 patients, and data on current smoking habits were available for 19 patients. Only four patients lacked a smoking history. Sixteen patients (76%) had a smoking history, and 10 patients (48%) were current smokers at the time of diagnosis or during follow-up. In contrast, history of tobacco use was 23% among patients with Hashimoto's thyroiditis during the same time period (10). The frequency of positive smoking history did not differ between patients with initial diagnosis before 1990 and those with diagnosis after that period. Four patients, all of whom were current smokers, required more than one course of corticosteroids because of severe and progressive processes. Of the four patients who were still on corticosteroids at last follow-up, two were documented to be current smokers and the other two had a smoking history. Of the four patients with no smoking history, one had insufficient treatment data, one did not require treatment with corticosteroids, one received one course of corticosteroids for extrathyroidal disease but not for thyroid disease, and one received two successful courses of corticosteroids (one for retroperitoneal fibrosis and one for IFT). None of the patients who never smoked were still taking corticosteroids at the end of follow-up.
Thyroid and parathyroid function and thyroid autoimmunity
Data on thyroid autoimmunity were variably available from the time of presentation (Table 1). Fifteen patients had measurement of antibodies to thyroid peroxidase during follow-up; 12 of the 15 had positive titers. Data regarding thyroid function were available for 20 patients at some time during the observation period and for 19 patients at the time of presentation (Table 1). At presentation, none were hyperthyroid, 5 were euthyroid, and 14 were hypothyroid, although 1 of these 14 patients had a prior history of Graves' hyperthyroidism treated with methimazole. One additional patient was treated with levothyroxine, without sufficient data to determine whether the treatment aim was thyroid suppression or supplementation.
Per number tested.
TG, antithyroglobulin antibody; TPO, antithyroid peroxidase antibody; TSI, thyroid-stimulating immunoglobulin.
Three patients (14%) had evidence of spontaneous hypoparathyroidism at the time of presentation on the basis of serum calcium and phosphorous measurement. The spontaneous hypoparathyroidism resolved in one patient after corticosteroid and tamoxifen therapy.
Additional laboratory findings
Erythrocyte sedimentation rate was measured in 11 patients at different stages of disease course and treatment; mean (SD) value was 65 (43) mm/h (range, 6–142 mm/h). Serum IgG4 levels were measured in two patients. Serum IgG4 was low in one patient (7.6 mg/dL; reference range, 8.0–140.0 mg/dL), but the other IgG subclasses were within normal limits. Her thyroid specimen, which was obtained before treatment, showed “a few IgG4-positive plasma cells” with immunoperoxidase staining. Serum IgG4 level was normal in the other patient. For this patient, staining of thyroid tissue, obtained before treatment, was “moderately positive” for IgG4.
Fine-needle aspiration biopsy
Of eight more recent patients who underwent fine-needle aspiration (FNA) biopsy of the thyroid, results in six were nondiagnostic. One patient, who also was positive for anti–thyroid peroxidase antibody, showed chronic lymphocytic thyroiditis, and the other patient showed “mixed inflammation and reactive thyroid epithelial cells.”
Imaging characteristics
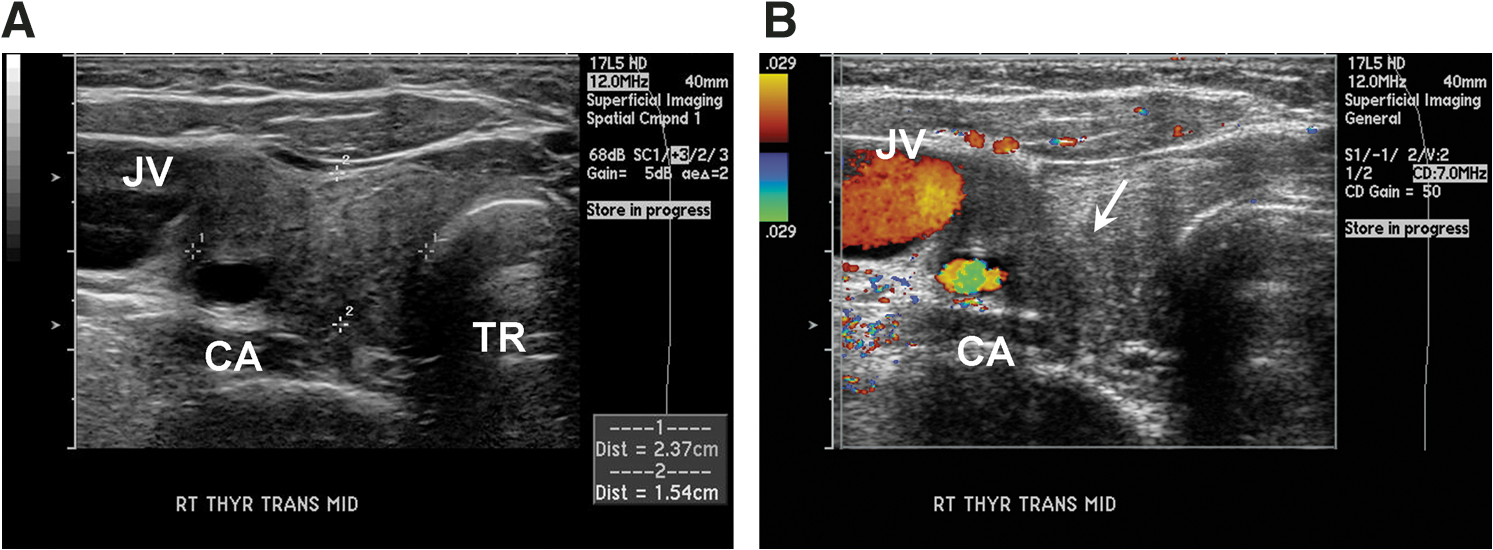
Ultrasonography of the neck was performed in 10 patients. In all, the thyroid showed heterogeneous hypoechoic texture with areas of lack of penetration of sound. The pattern was different from the hypervascular and “Swiss cheese” appearance usually seen in Hashimoto's thyroiditis. Doppler flow showed low vascularity, as opposed to what is seen in Graves' disease and Hashimoto's thyroiditis (Figs. 1 and 2). Calcified spots with shadowing were noted in four patients. Tracheal narrowing could be demonstrated in three patients. The carotid artery was encased in two patients and narrowed in three (Fig. 2). Cervical venous occlusion was noted in one patient. In the other patients, vascular compromise could not be demonstrated. In three patients, repeat ultrasonography at 1–4 years showed disease stability.
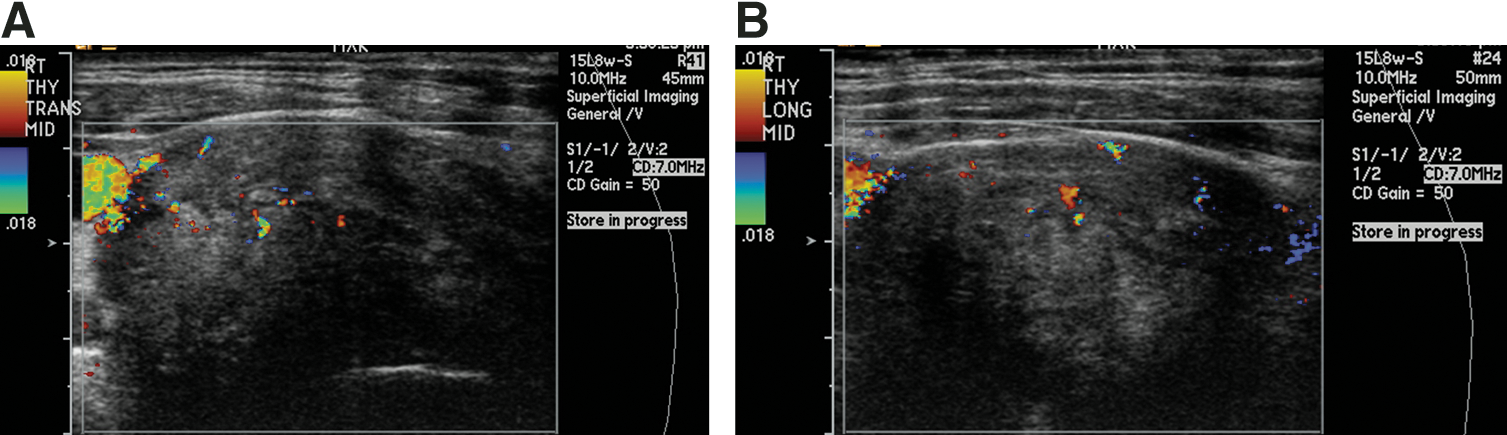
Doppler ultrasonography of the right lobe of the thyroid in a patient with invasive fibrous thyroiditis (IFT) shows heterogenous echo texture and low vascularity.
Ultrasonography (transverse views) of the right lobe of the thyroid in a patient with IFT.
Computed tomography (CT) of the neck was available in 12 patients. CT was a better imaging study for evaluation of tracheal narrowing and airway compromise (Fig. 3). Tracheomalacia and direct invasion of the trachea were not noted. Encasement or narrowing of major neck vessels, in particular the common carotid artery, was noted in seven patients. One patient had obstruction of the common carotid artery with direction of blood to the internal carotid artery through collaterals. The internal jugular vein was encased or narrowed in four patients. The inferior vena cava near the innominate vein was compressed in one patient.

Computed tomography of the neck shows significant tracheal narrowing (arrow) in a patient with IFT who had respiratory distress and pain and required isthmectomy to relieve pressure on the trachea.
Magnetic resonance imaging (MRI) was available in three patients and did not supply additional information. In one patient, MRI confirmed obstruction of the common carotid artery, which was also noted on CT of the neck. Of the 12 patients who had imaging results available, 7 had evidence of major neck blood vessel involvement, by ultrasonography, CT, or both.
Extrathyroidal fibrosis
Eight patients had disease occurring in one or more extrathyroidal locations. Four patients had fibrosing mediastinitis: at the time of IFT diagnosis in 3, and 10 years later in one. Three had retroperitoneal fibrosis. This developed 1, 2, and 3 years, respectively, after diagnosis of IFT. One patient each had orbital fibrosis (6 months after diagnosis of IFT), pancreatic fibrosis, and epidural space fibrosis documented by biopsy. One patient had subcutaneous chest mass in the area of a ventroperitoneal shunt placed for hydrocephalus (8 years after diagnosis of IFT); on biopsy, fibrous tissue similar to IFT was found. Of interest, hydrocephalus was diagnosed in two patients within 1 year after diagnosis of IFT. Its relationship to multifocal systemic fibrosis was not clear. One patient who had mediastinal fibrosis, IFT, and retroperitoneal fibrosis at age 34 years had myocardial infarction. During coronary artery bypass grafting surgery, he was found to have fibrosis involving the left anterior descending coronary artery resulting in coronary obstruction without evidence of an atherosclerotic process. This patient died 20 years later of unrelated causes.
Other associated conditions
Three patients had Graves' disease, two with associated Graves' ophthalmopathy. In one patient who had left thyroid lobe IFT, and who was the subject of a previous report (11), Graves' hyperthyroidism involving the right lobe developed 4 years later. One patient who previously had hyperthyroidism with ophthalmopathy became hypothyroid when IFT developed. One patient had pseudotumor cerebri before the diagnosis of IFT. Other associated conditions included giant cell arteritis in one patient, ankylosing spondylitis several years after diagnosis of IFT in one patient, and keratoconjunctivitis sicca syndrome diagnosed after IFT.
Treatment
Surgical excision of at least part of the thyroid was performed for 18 patients, 7 of whom had predominantly isthmectomy. Three patients had only open biopsy. Complete excision of the sclerotic mass was not possible in any of the patients. Treatment regimens and outcomes are summarized in Table 2.
Measured from the time of diagnosis.
F, female; M, male.
Seven patients had complications from thyroid surgery, ranging from transient to permanent vocal cord paralysis to severe hypoparathyroidism. Two patients had tracheostomy intraoperatively.
Thirteen patients were treated with prednisone. These were more recent patients with severe disease. The mean (SD) starting dose was a prednisone equivalent of 73 (31) mg. The mean duration of treatment was 163 weeks. Four patients required more than one course of corticosteroids. At the end of the follow-up period, four patients were still on corticosteroids for an average treatment duration of 370 weeks.
Six patients seen in the last decade of the study period were treated with tamoxifen; of these, four patients were treated with prednisone simultaneously. One additional patient was treated with a course of tamoxifen for retroperitoneal fibrosis, before the development of IFT. Three patients had progression of their disease while taking tamoxifen. One was also taking corticosteroids at the time of progression.
Outcome
After a mean follow-up of 9.5 years, the fibrotic process, according to clinical assessment and imaging studies, had improved or partially resolved with management in 11 patients, and 7 patients had stabilization. Three patients did not have long-term follow-up and had progression of the disease process in short-term follow-up. No cause-specific mortality was observed. At last follow-up, 17 of 21 patients (81%) were hypothyroid, 2 (10%) were euthyroid, and 1 (5%) was hyperthyroid with a diagnosis of Graves' disease.
Discussion
Etiology and pathogenesis
The etiologic mechanisms underlying IFT are unclear. The prevailing view is that it is part of a generalized fibroinflammatory process commonly involving other organs. Several histologic and serologic features in patients with IFT support the autoimmune mechanisms, including the presence of mononuclear cells within the fibrosclerotic process and the detection of autoantibodies against thyroid-specific antigens (5,6). An association between IFT and Hashimoto's thyroiditis has been suggested (12). In two of our previously reported patients (5), IFT evolved from antecedent Graves' disease, documented by the presence of thyroid dysfunction, ophthalmopathy, and high levels of thyrotropin receptor-stimulating autoantibodies.
IgG4-positive plasmocytes have been demonstrated in several other fibrotic conditions, including multifocal systemic sclerosis (13), which is similar to IFT, and retroperitoneal fibrosis and idiopathic autoimmune pancreatitis, which may also be associated with IFT (14). In two of our patients, tissue staining was positive for IgG4.
Association with tobacco use
The association of IFT in our patients with current and previous smoking and the association of smoking with more severe disease are of interest and have not been previously reported. History of tobacco use was present in 76% of our patients, and 48% were current smokers at the time of diagnosis. None of the never-smokers were using corticosteroids at the end of follow-up. The percentage of smokers was similar in patients seen in the most recent decade and those seen in previous decades. This observation requires confirmation but has similarities to the association of tobacco use with severe extrathyroidal complications of Graves' disease: smokers are more likely to have severe Graves' ophthalmopathy (15). In a previous report, we documented a high percentage of smokers among patients with thyroid dermopathy and acropachy (16); in comparison, the percentage of smokers among patients with Hashimoto's thyroiditis was the same as in the general population during the same time interval (10). Because fibroblast activation is also present in extrathyroidal manifestations of Graves' disease, it is theoretically possible that use of tobacco augments immune processes and activates fibroblasts. The established association of tobacco use with the severity of extrathyroidal manifestations of Graves' disease (17,18) and the present observations related to IFT and tobacco use may indicate similar phenomena. However, the exact cause remains unclear.
Presentation and diagnosis
In our patients, IFT presented as pressure symptoms in the neck, respiratory distress, dysphagia, or pain, or as symptoms of hypothyroidism or hypoparathyroidism. In most of our cases, IFT presented with neck mass, neck discomfort, and pain or respiratory distress. Hypoparathyroidism may be a presenting symptom in some cases. Several reports have described IFT in association with hypoparathyroidism not related to complications of surgery (19 –21). Three of our patients had hypoparathyroidism before surgical intervention. In one of these patients, hypoparathyroidism resolved after treatment of IFT.
Clinicians should suspect IFT if a stony, hard, neck mass is present along with compressive symptoms out of proportion to the size of the goiter. However, open biopsy is needed to demonstrate the extension of fibrosis outside the thyroid capsule. In our cases, diagnosis was not possible by FNA biopsy; tissue diagnosis and evidence of extrathyroidal extension of fibrosis was needed for diagnosis of IFT in our series. Conditions such as fibrotic Hashimoto's thyroiditis, sarcoma of the thyroid (22), and anaplastic carcinoma may mimic IFT (23,24). Diffuse sclerosing papillary thyroid cancer may have histologic similarities and should be ruled out (25). Diagnosis currently requires the presence of a fibroinflammatory process of the thyroid with extension into surrounding tissues, an inflammatory infiltrate without giant cells, lymphoid follicles, oncocytes, or granulomas, occasional evidence of an occlusive phlebitis, and absence of a thyroid neoplasm (4).
Imaging
Similar to previous reports (26,27), ultrasonography of the neck in our cases showed hypoechoic structure with very low or absent vascularity by Doppler imaging. If IFT is suspected on the basis of respiratory distress, associated hypoparathyroidism, or vocal cord paralysis in the presence of a fixed, hard, neck mass, the best imaging modality, particularly for evaluation of tracheal status, is CT with contrast, which shows the extent of disease and status of the vascular structures in the neck. If associated hyperthyroidism is present, with the possible need for radioactive iodine therapy, contrast should be avoided. MRI shows heterogeneous hypointensity on both T1- and T2-weighted images and shows mild enhancement after administration of gadopentetate dimeglumine. MRI was performed for three of our patients, but it added no new information to ultrasonography and CT.
Positron emission tomography (PET) with 18F-fluorodeoxyglucose (FDG) also may be helpful. In one study, follow-up PET after 2 weeks of corticosteroid treatment showed a 60% decrease in the uptake of FDG in the thyroid (28). This indicates that FDG metabolic activity can also be used to assess a patient's response to therapy in IFT. Sites of multifocal fibrosclerosis can be demonstrated by FDG-PET. FDG-PET can help to establish the diagnosis of multifocal fibrosclerosis and evaluate the activity of and patient response to corticosteroid therapy (29). PET was not used for any patients in our series.
Association with Graves' disease and Hashimoto's thyroiditis
Hyperthyroidism followed by a diagnosis of IFT has been reported (19). Three patients in our series, who had Graves' disease (2 had Graves' ophthalmopathy) with anti-TSH receptor antibodies, have been previously reported from our institution (5,11).
Several cases of antecedent or coincident Hashimoto's thyroiditis have been reported with IFT (5,30). Several reviews have noted a high incidence of positive thyroid antibody titers in patients with IFT (31). However, the strength of the association and causality remain uncertain. Of 15 patients in the present series who had antibody measurement, 12 (80%) had positive antithyroid antibodies.
Multifocal systemic fibrosclerosis and other conditions
Orbital sclerosing fibrosis and orbital pseudotumor can be seen in conjunction with IFT as part of the multifocal fibrosclerosis (32). Orbital fibrosis can be associated with involvement of the lacrimal gland (33).
In the present series, 38% of our patients had extracervical fibrosis such as mediastinal and retroperitoneal fibrosis. IFT can occur years after or at the same time as retroperitoneal fibrosis (34,35). Follow-up is essential to monitor for involvement of other areas of localized fibrosis such as autoimmune pancreatitis, retroperitoneal fibrosis, tubulointerstitial nephritis, and autoimmune hypophysitis, all of which show IgG4 involvement in their pathogenesis. One of our previously reported patients (36) had hydrocephalus and hypoparathyroidism and a ventriculoabdominal shunt that was later obstructed by localized subcutaneous fibrosclerosis of the anterior chest wall. The cause of hydrocephalus in two of our patients was not clear, but epidural fibrosis in another of our patients raises the possibility of fibrosis as a cause. A case report of IFT with multisegmental leptomeningeal fibrosis supports the association (37).
Chance association of IFT with follicular cancer was described in one case report (38). A case with pathologic evidence of giant cell arteritis in the thyroidectomy specimen also has been reported (39). One of our patients had development of giant cell arteritis. In the present series some of the complications were related to associated systemic fibrosis such as vena cava obstruction and coronary artery obstruction.
Treatment
Of 18 patients in our series who had surgery, 7 had complications including hypoparathyroidism or vocal cord paralysis. Two required tracheostomy. Complete excision was not possible in any. Attempt at thyroidectomy was associated with a high degree of surgical complications and should be approached with caution. The best approach is to resect the isthmus to relieve pressure on the trachea. In most cases, only open biopsy for diagnosis is needed, followed by medical therapy. More radical procedures have no advantage. Surgery in IFT requires special expertise, and intraoperative nerve monitoring is recommended (40).
Patients treated before 1995 received corticosteroid monotherapy, and the more recent six cases received corticosteroids in combination with tamoxifen. Although long-term stability of the fibrotic process was noted in all patients and some had substantial early response, evidence for the comparative effectiveness of these medical therapies remains anecdotal.
In our group, six patients received therapy with tamoxifen. Since four of those were also receiving corticosteroid therapy, the effectiveness of monotherapy with tamoxifen cannot be evaluated. Of note, three of these patients had progression of disease despite 6 months of tamoxifen therapy. Tamoxifen therapy has been used for retroperitoneal fibrosis and for IFT with good results (41). Complete resolution after 1 year of therapy with 20 mg twice daily tamoxifen was noted in one case of IFT (9). The beneficial effects of tamoxifen are not related to antiestrogen activity. Tamoxifen decreases the expression of transforming growth factor-β, with the consequent inhibition of both fibroblast proliferation and collagen production (42). Because of the small number of patients using tamoxifen in our series and the lack of uniform response to this therapy, the effectiveness of tamoxifen from the present data remains unclear.
In a recent report of 28 patients with retroperitoneal fibrosis, combined prednisone (40 mg/d tapered over 6 months) and mycophenolate mofetil (1000 mg twice daily, for a mean of 24.3 months) resulted in resolution of symptoms in all patients and at least a 25% decrease in lesion mass in 25 patients (89%) (43). Since IFT and retroperitoneal fibrosis have a similar pathogenesis, it may be reasonable to try similar therapies for IFT.
Limitations
The current study was limited by its retrospective chart review design and the small size of the study population, which is not surprising given the low incidence of the disease. We did not have the opportunity for long-term follow-up in some cases. A detailed account of the initial presentation was not always available for cases in which the initial diagnosis was made at outside facilities. In some cases, we were unable to distinguish between the lack of documentation and the lack of occurrence of a particular symptom, treatment detail, or outcome. In addition, our patient population may be biased toward those who have more severe manifestations, and milder cases may not have been referred.
Conclusion
IFT is a systemic autoimmune fibroinflammatory disorder that is associated with involvement of other organs in 38% of patients. Long-term follow-up shows that almost half of patients have either improvement or resolution of disease with a combination of surgical decompression and medical therapy, and the remainder achieve stabilization. In the present series we did not encounter any cause-specific mortality. IFT may follow Hashimoto's thyroiditis or be associated with Graves' disease and Graves' ophthalmopathy. In our study, the disease showed a high association with tobacco use. Open biopsy is needed for diagnosis because FNA biopsy is usually nondiagnostic or cannot distinguish IFT from Hashimoto's thyroiditis. When decompression is needed, isthmectomy is usually adequate. Attempt at extensive excision is associated with a high rate of complications and should be avoided. There is fair evidence for the effectiveness of isthmectomy, corticosteroid therapy, and tamoxifen. Almost all patients will become hypothyroid eventually, either spontaneously or as a result of thyroidectomy. Hypoparathyroidism may be present at IFT presentation and is assumed to be due to compression or destruction of parathyroid glands by the invasive fibrosclerotic process.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.