
Abstract
Background:
Although fine-needle aspiration biopsy (FNAB) is considered the standard for preoperative evaluation of thyroid nodules, the value of this has been questioned for large thyroid nodules. Here, we evaluated the diagnostic accuracy of ultrasound-guided FNAB (US-FNAB) for thyroid nodules that were 3 cm or larger as well as the sonographic differences between benign and malignant nodules in this size group.
Materials and Methods:
There were 661 thyroid masses equal to or larger than 3 cm who underwent US-FNAB from February 2002 to December 2006 and were included in this study. The cytology and surgical pathology readings in these patients were reviewed along with the ultrasonography features, the last from the retrospective review by one radiologist. Histopathology was used to calculate accuracy parameters for the US-FNAB cytology readings. In addition, the likely diagnoses for patients with a benign cytology reading were ascertained.
Results:
Thyroid surgery was performed for 206 of the 661 nodules in the same number of patients (31.2%). All subjects who had inadequate, indeterminate, or suspicious for malignancy cytology readings had thyroid surgery. All of the patients who did not have thyroid surgery were considered likely to have benign disease because of their initial cytology reading and follow-up, and finally, 587 (88.8%) were benign and 74 (11.2%) were malignant. When considering malignant, suspicious for malignancy, and indeterminate cytology readings as positive and benign cytology as negative, the sensitivity was 96.7%, specificity 85.9%, positive predictive value 76.6%, negative predictive value 98.2%, and accuracy 89.4%. Ultrasonography features of malignancy were more prevalent in thyroid nodules that were malignant compared with those that were benign or considered likely to be benign (70.3% vs. 1.2%, p < 0.001), and ultrasonography features of a benign nodule were more prevalent in thyroid nodules that were benign or considered likely to be benign than those that were malignant (94.9% vs. 29.7%, p < 0.001).
Conclusion:
In this study, US-FNAB appeared to be a relatively accurate method to evaluate thyroid nodules larger than 3 cm, with false-negative rates of about 2%. Much larger series would be required to determine its utility in this setting.
Introduction
Materials and Methods
Patients
This retrospective study was approved by the institutional review board, and informed consent was waived. From February 2002 to December 2006, 15,574 patients underwent US-FNAB for initial diagnosis of thyroid nodules in our institution. Among them, 987 patients who had thyroid masses 3 cm or larger in the longest diameter on ultrasonography were initially evaluated because of the study that highlighted the problem of relatively high false-negativity for malignancy rates in thyroid nodules that were 3 cm or larger (6). Cytologic results of the 987 masses were as follows: inadequate in 118 (12.0%), benign in 773 (78.3%), indeterminate in 24 (2.4%), suspicious for malignancy in 19 (1.9%), and malignant in 53 (5.4%). Of the 161 masses diagnosed as inadequate, indeterminate, or suspicious for malignancy on cytology, only those which had thyroid surgery were included in this study. There were 17 patients with nodules with an inadequate cytology reading who had thyroid surgery, 18 with indeterminate cytology reading who had thyroid surgery, and 15 with a suspicious cytology reading who had thyroid surgery. Among the masses diagnosed as benign on cytology, 215 masses were excluded because of loss of follow-up or follow-up interval of <1 year. The remaining 558 lesions were included in the study population. A total of 661 masses were finally included in this study. Of the 558 nodules with a benign cytology reading and who were included in the study, 112 had thyroid surgery, and of the 53 nodules with a malignant reading and who were included in the study, 44 had thyroid surgery. All of the nodules with an inadequate, indeterminate, and suspicious cytology reading who were included in the study had thyroid surgery (Table 1). Medical records of these patients were retrospectively reviewed for clinical information.
One case of follicular variant PTC and two of conventional PTC.
One case of follicular variant PTC.
US-FNAB, ultrasound-guided fine-needle aspiration biopsy; PTC, papillary thyroid carcinoma; AH, adenomatous goiter; MNG, multinodular goiter; FA, follicular adenoma; HCA, Hürthle cell adenoma; AC, anaplastic carcinoma; FC, follicular carcinoma; HCC, Hürthle cell carcinoma.
Imaging methods and analysis
Ultrasonography was performed with 8–15-MHz (Acuson Sequoia; Siemens Medical Solutions), 7–15-MHz (HDI5000; Philips Medical Systems), and 5–12-MHz linear array transducers (iU22; Philips Medical Systems). Compound imaging was obtained in all images with an HDI5000 or iU22 machine.
Ultrasonography features of the 661 thyroid masses were retrospectively reviewed by one radiologist (J.H.Y.), without acknowledgment of the histopathologic diagnosis. Each mass was described according to the ultrasonography features: internal components, echogenicity, margin, calcifications, and shape. Internal components were divided into solid, solid and cystic, that is, mixed echoic nodules with >50% of solid contents, mixed echoic nodules with <50% of solid contents, and cysts. Marked hypoechogenicity (decreased echogenicity compared with the adjacent strap muscle), microlobulated or irregular margins, microcalcifications or mixed calcifications, and taller-than-wide shape were features that were classified as suspicious based on the previously published criteria (10). The taller-than-wide shape was a greater anteroposterior dimension than transverse dimension in either the transverse or longitudinal ultrasonography plane. Masses having one or more of the described features above were classified as suspicious for malignancy on final ultrasonography assessment. When the thyroid mass showed none of the features described above, they were classified as probably benign.
Tissue sampling and cytologic analysis
Real-time ultrasonography and subsequent FNAB were performed by one of the five board-certified radiologists with 1–13 years of experience of thyroid imaging. US-FNAB was performed on the most solid-appearing areas of the thyroid mass with direct visualization of the needle tip within the nodule. If cystic components consisted of the majority of the mass, fluid aspiration was performed prior to the biopsy, which was targeted to the remaining solid portion of the mass. Informed consent was obtained from all patients before US-FNAB.
US-FNAB was performed with a 23-gauge needle attached to a 20-mL disposable syringe using an aspirator or a 23-gauge needle attached to a 2-mL disposable syringe without an aspirator depending on the radiologists' preference. Local anesthesia was not routinely applied during procedures. Samples obtained were expelled on glass slides, smeared, and immediately placed in 95% alcohol for Papanicolaou staining. The remaining material in the syringe was rinsed in saline for cell block processing. Cytopathologists were not present during US-FNAB. Additional special staining was performed on a case-by-case basis at the request of the cytopathologist (11).
One of the five cytopathologists specializing in thyroid cytology interpreted the smears obtained from US-FNAB. During the study period, cytology reports were divided into the following five categories in our institution (11): (i) malignancy, (ii) suspicious for papillary thyroid carcinoma (PTC), (iii) indeterminate cytology, (iv) benign, and (v) inadequate for diagnosis. Malignancy indicates that the specimen contains abundant cells of unequivocal cytological features of malignancy. Specimen categorized as suspicious for PTC refers to those exhibiting cytological atypia, that is, crowded, overlapping, pleomorphic, and enlarged nuclei (11), but with insufficient cellularity for diagnosis of malignancy (12,13). Indeterminate cytology includes follicular neoplasm or Hürthle cell neoplasm, meaning the cytological features demonstrate monotonous cellular population and scanty colloid, but lack typical papillary carcinoma features (14). Benign cytology includes colloid nodules, nodular hyperplasia, lymphocytic thyroiditis, Graves' disease, and postpartum thyroiditis. Inadequate cytology refers to specimen showing less than a minimum of six groupings of well-preserved thyroid cells, which consists of <10 cells per group (11,15), insufficient for accurate diagnosis. But specimens having abundant colloid material but lacking the required number of follicular cells to be interpreted as adequate were diagnosed as benign.
Statistical analysis
In patients who had thyroid surgery, the histopathologic reading of the surgical specimen was the reference criteria for the final diagnosis. In nodules that were not removed by surgery, the repeat FNAB cytology and findings on follow-up ultrasonography for at least 1 year were the reference criteria for the final diagnosis. There were 206 (31.2%) of the 661 patients that met the final inclusion criteria in the study who had thyroid surgery. Of the remaining 455 (68.8%) patients, the FNAB cytology reading and the follow-up ultrasonography was used to make the final diagnosis.
The diagnostic performances (sensitivity, specificity, positive predictive value [PPV], negative predictive value [NPV], and accuracy of the cytology readings) in thyroid nodules that were removed by surgery were calculated with the exception of those readings in which the cytology was inadaquate. For this, 206 nodules removed by surgery were divided into two groups based on the cytology readings of US-FNAB according to the following: considering malignant, suspicious for malignancy, and indeterminate cytology readings as positive and benign cytology reading as negative. The false-negative rate of US-FNAB was defined and calculated as lesions having a benign cytologic result in which the nodule is later diagnosed as malignant on surgical pathology. This was done for comparison with a previous study (6,8). False-positive rate of US-FNAB was defined and calculated as lesions having a suspicious for PTC or malignant cytologic results in which the nodule is later diagnosed as benign on subsequent surgery.
Chi-square test or Fisher's exact test was used to compare the ultrasonography features of benign and malignant masses. All statistical analyses were performed with SAS version 9.1 (SAS, Inc.), and p < 0.05 was considered statistically significant.
Results
Patient demographics
Of the 661 patients, 117 (17.7%) patients were men and 544 (82.3%) were women. The female-to-male ratio was 4.6:1. The mean age of the patients was 48.0 years, ranging from 15 to 89 years. Three hundred sixty-two (54.8%) patients had single thyroid lesions, while the remaining 299 (45.2%) had multiple lesions with nodules <3 cm in other regions of the thyroid. The mean size of the thyroid nodules was 3.9 cm, ranging from 3 to 15.0 cm (median: 3.6 cm). Nodules with size ranging from 3 to 4 cm made up 76.2% of all the nodules in the study.
Thyroid nodules for which surgery was performed
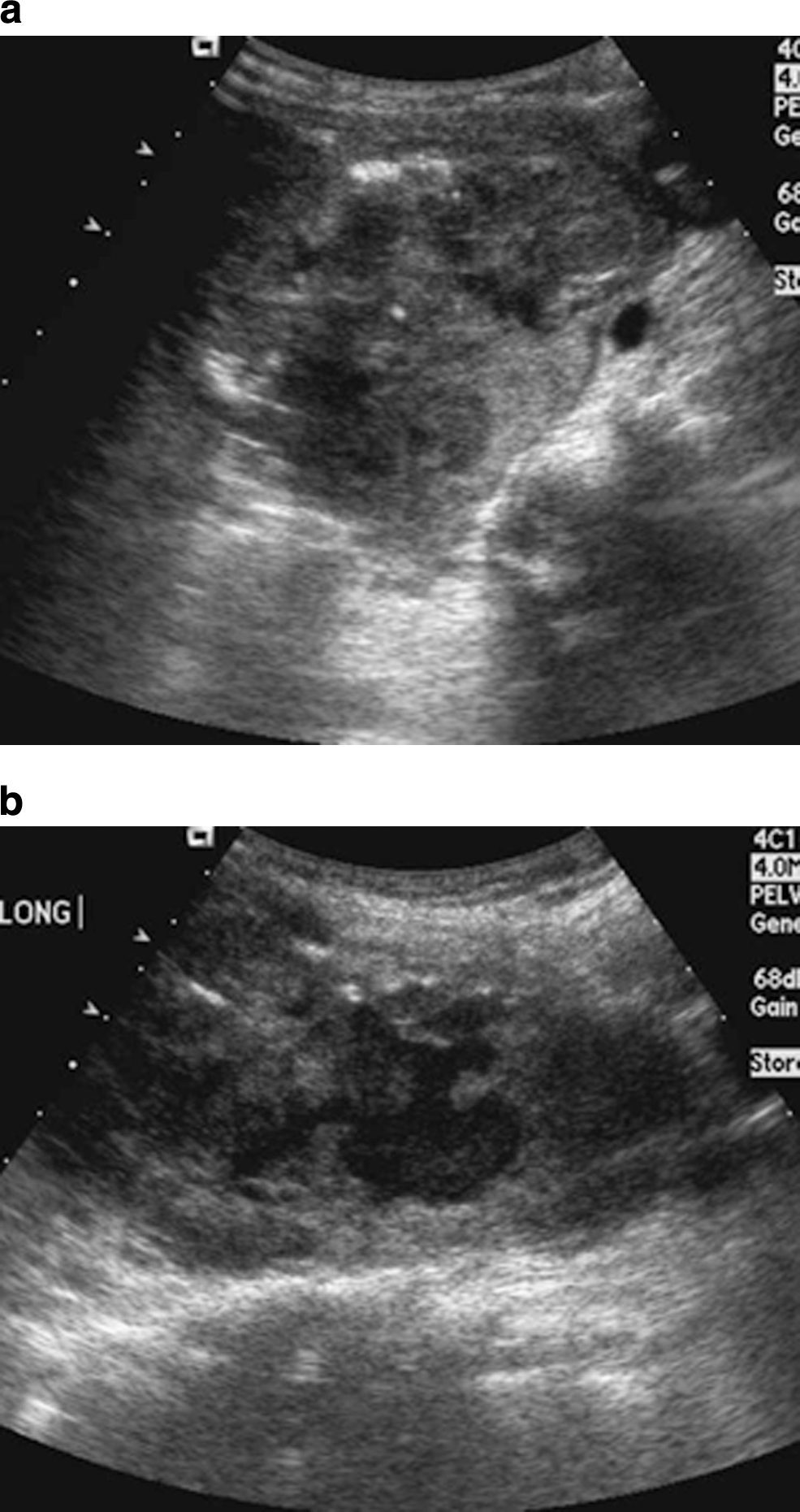
Table 1 shows the cytology readings and histopathology readings for the 206 thyroid nodules for which thyroid surgery was performed. The extent of surgery was based on their cytology results and thyroid ultrasonography. A lobectomy, subtotal thyroidectomy, or total thyroidectomy was performed if the cytology reading was malignant or suspicious for PTC or if the ultrasonography reading was suspicious for malignancy in nodules with benign cytology readings. A lobectomy or subtotal thyroidectomy was performed if the cytology reading was benign. If the cytology reading was inadequate or indeterminate, the extent of thyroid surgery was based on the frozen section reading during surgery. Ninety-four (45.6%) masses were subjected to thyroid surgery for readings of inadequate (n = 17), indeterminate (n = 18), suspicious for malignancy (n = 15), or malignant (n = 44). There were 112 (54.4%) masses that were read as benign on cytology, but were subject to thyroid surgery for various reasons such as the presence of symptoms, increasing size or suspicious ultrasonography features, indeterminate cytology on follow-up US-FNAB, other malignant lesions, altered thyroid function, and surgeons' recommendations. Most of these patients had a thyroid operation because of signs or symptoms of a palpable or protruding neck mass, tracheal displacement from the large mass (29.5%, Fig. 1), or increased size on follow-up (27.7%).
Benign: A 44-year-old female patient had a palpable mass in the right lower neck area. Ultrasonography
The final histopathologic diagnoses of the 206 for which thyroid surgery was performed are summarized in Table 1. When considering malignant, suspicious for malignancy, and indeterminate cytology readings as positive and benign cytology reading as negative, the sensitivity was 96.7%, the specificity was 85.9%, the PPV was 76.6%, the NPV was 98.2%, and the accuracy was 89.4%.
Of the 206 masses for which thyroid surgery was performed, 112 were diagnosed as benign on preoperative US-FNAB. Two of these were read as malignant on surgical pathology, and the rest were read as benign. Therefore, the false-negative rate of US-FNAB was 1.8% (2/112). There were also 59 nodules that were diagnosed as suspicious for malignancy or malignancy by cytology. Six of these were benign on surgical pathology and the rest were malignant. Therefore, the false-positive rate for a cytology reading of suspicious for PTC or malignancy was 10.2% (6/59).
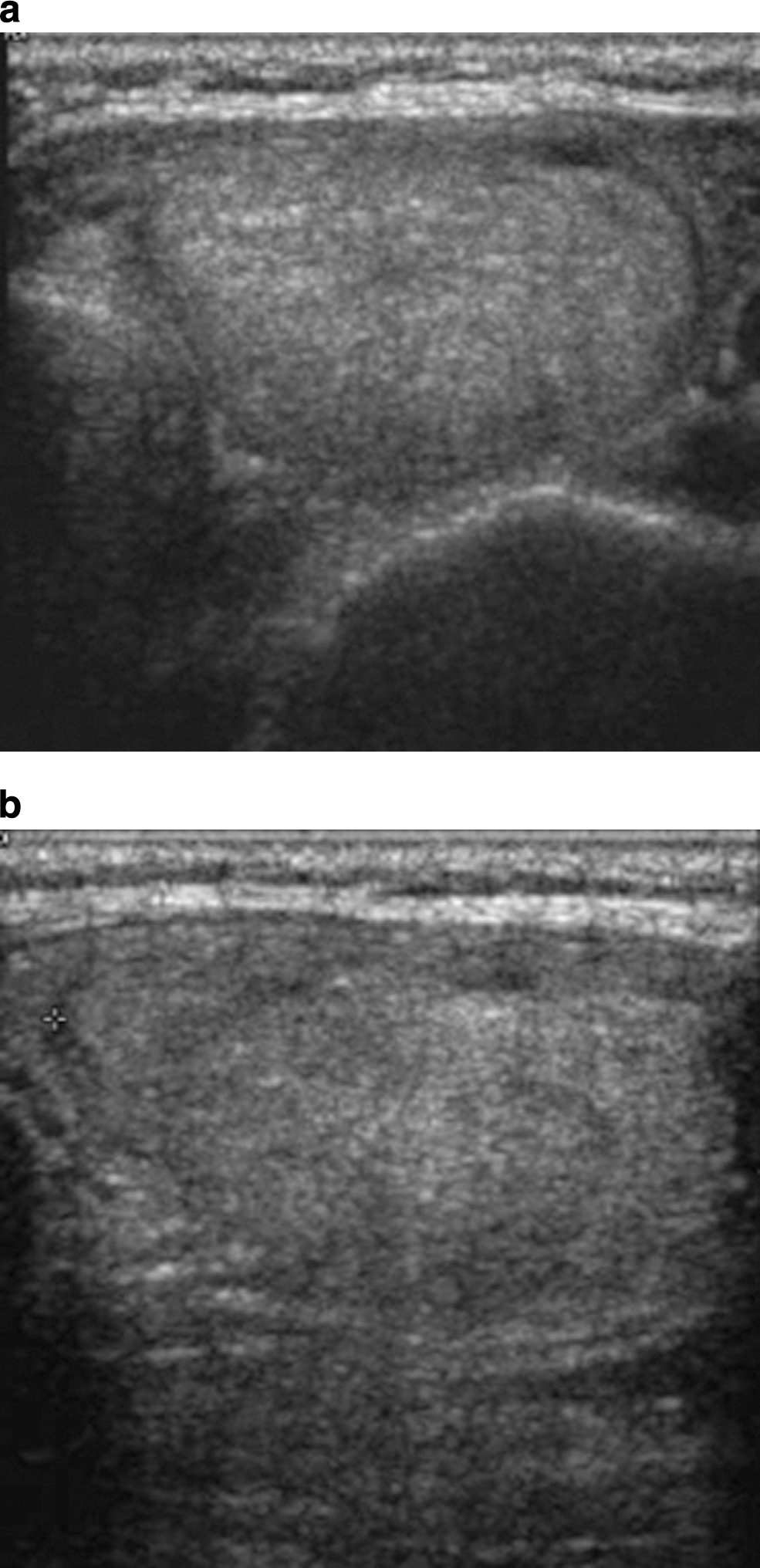
Among the 65 thyroid nodules that were malignant on surgical pathology, there were 4 that were diagnosed as inadequate on cytology, 59 were diagnosed as indeterminate or suspicious for malignancy or malignancy on cytology, and 2 were diagnosed as benign on cytology (Table 1). Of the two thyroid lesions diagnosed benign on cytology but malignant on surgical pathology, one was considered to be a benign mass on thyroid ultrasounds and the other had suspicious ultrasonography features (Fig. 2). Both of these lesions were anaplastic thyroid carcinoma by surgical pathology. The benign-appearing mass underwent US-FNAB twice, each time having benign or inadequate cytology.
Malignant: A 89-year-old female patient had a palpable mass with recently increased size in the left neck. Ultrasonography
Thyroid nodules read as benign on cytology for which surgery was not performed
Among the 446 thyroid nodules that were read as benign on cytology and for which surgery was not performed, there were 157 (35.2%) for which repeat US-FNAB was performed. In the readings for the repeat biopsy, 135 (86.0%) were read as benign and 22 (14.0%) as inadequate. None was read as indeterminate or suspicious for malignancy or malignancy.
The remaining 289 (64.8%) thyroid nodules that did not have repeat US-FNAB have been followed up for at least 1 year, with a mean interval of 30.1 months (range: 12–69 months). Among them, 222 (76.8%) did not show significant size changes or tumor characteristics during follow-up, 64 (22.1%) decreased in size, and 3 (1.0%) increased in size. Of the 64 masses having a decrease in size, 38 were mainly cystic, and from them fluid was aspirated at the beginning of the US-FNAB procedure. The three thyroid nodules that increased in size appeared to have an increase in the cystic components of their nodule. Taking all thyroid nodules that were considered to be benign based on either surgical pathology or the initial cytology with follow-up, the malignancy rate for these was 0.4% (2/558).
Thyroid ultrasound differences between benign and malignant lesions
The ultrasonography features of the 661 thyroid masses are summarized in Table 2. Mixed echoic masses with cystic components (41.6% vs. 27.0%), cysts (18.8% vs. 0.0%), well-defined margins (99.1% vs. 48.6%), isoechogenicity (69.3% vs. 23.0%), no calcifications (93.0% vs. 41.9%), parallel shape (99.7% vs. 95.9%), and no metastatic LNs (100.0% vs. 73.0%) were more prevalent in the 587 thyroid nodules that were considered benign based on surgical pathology, or initial cytology without thyroid surgery or follow-up, and initial cytology without thyroid surgery but with follow-up, compared with the 74 malignant nodules (p < 0.05). In the 74 thyroid nodules that were malignant on thyroid histopathology, there was a greater prevalence of either solid to mainly solid character (12.2% vs. 4.3% and 58.1% vs. 35.3%), microlobulation (36.5% vs. 0.7%), ill-defined margins (14.9% vs. 0.2%), hypo- (68.9% vs. 29.5%) to markedly hypoechogenicity (6.8% vs. 0.2%), macro- (39.2% vs. 6.0%) or microcalcifications (18.9% vs. 1.0%), nonparallel shape (4.1% vs. 0.3%), or the presence of metastatic appearing lymph nodes (27.0% vs. 0.0%) compared with 587 thyroid nodules that were considered benign (p < 0.05). Ultrasonography features of malignancy were more prevalent in thyroid nodules that were malignant compared with those that were benign or considered likely to be benign (70.3% vs. 1.2%, p < 0.001) and ultrasonography features of a benign nodule were more prevalent in thyroid nodules that were benign or considered likely to be benign than those that were malignant (94.9% vs. 29.7%, p < 0.001).
Discussion
Controversy remains in considering tumor size as a risk factor of thyroid malignancy. Although there are several reports in which increased size is not an independent factor for predicting malignancy (16 –18), many others concluded that large size indeed leads to increased risk for malignancy (4,19 –21), and therefore, a surgical recommendation is needed regardless of the preoperative cytology results. US-FNAB has proven excellent diagnostic performances, but has its limitations of being dependent on the skills of the operator/interpreting cytologist, false-negative results from faulty sampling in small nodules, and the diagnosis of follicular neoplasm (5). Most importantly, US-FNAB has been reported to have limited value in the accurate diagnosis of large thyroid nodules, specifically nodules larger than 3 cm (4,5,7). But diagnostic performances were similar or higher for thyroid masses larger than 3 cm included in this study, compared with a report comparing published series of >200 cases of thyroid FNAB (22), supporting the efficacy of US-FNAB in large masses as well as those smaller than 3 cm. For comparison, the false-negative rates of thyroid nodules larger than 3 cm reported in the literature are summarized in Table 3. In 1995, Meko and Norton reported a false-negative rate of 11%, which increased to 30% in larger, cystic/solid thyroid nodules with a higher probability of cancer (6). Several recent studies showed similar results in that the prevalence of malignancy is high in larger thyroid nodules, also with high false-negative US-FNAB results ranging from 13% to 50% (1,4). McCoy et al. reported a false-negative rate of 13% in nodules larger than 4 cm, ranging up to 16% when including multifocal micropapillary carcinomas (4). In contrast, one study showed a false-negative rate of 0.7% in US-FNAB of nodules larger than 3 cm and concluded that the diagnosis of benign is reliable in thyroid nodules regardless of size (8). Our results were more similar to this last study; the false-negative rate was 1.8% in the surgically proven thyroid nodules. We agree with the latter report in that US-FNAB is an accurate diagnostic tool that can be used regardless of size when performed under precise ultrasound guidance. As in the study previously mentioned (8), all FNAB procedures performed in our study were done with visualization of the needle tip with ultrasound during aspiration. This helps in reducing sampling errors (8), improving the diagnostic accuracy of US-FNAB regardless of lesion size. In addition, the false-positive rate in our study was 10.2%, and all nodules with false-positive results were diagnosed as suspicious for PTC on US-FNAB. None of the nodules diagnosed as malignancy on cytology showed false-positive results. The malignancy rate of the nodules diagnosed as suspicious for PTC on US-FNAB was 60.0%, lower than the 70%–85% reported in other studies (5,23,24), but this may have been affected by the inclusion of large masses in our study and the various cytology reporting systems in different institutions.
Increased to 30% in larger, cystic/solid thyroid nodules.
Increased to 16% when including multifocal micropapillary carcinomas.
NA, not applicable; Op, operation.
Adding to the false-negative results, our study shows that about 14.3% (16/112) of follicular neoplasm are misinterpreted as benign on cytology. This is within the rates reported (up to 30%) in other studies (5,25,26), and none of the two nodules with false-negative results proved to be follicular carcinoma. Large follicular neoplasms are known to contain areas of intratumoral heterogeneity, thereby misleading to benign interpretations. Differentiation of benign or malignant follicular neoplasm is impossible with cytology alone. Diagnostic lobectomy is essential in the definite diagnosis of follicular lesions, especially when considering the increased malignancy rates in follicular neoplasm of larger size (19,26,27).
As in smaller thyroid nodules, suspicious ultrasonography features were significantly associated with malignant masses in this study. Although suspicious ultrasonography features were significantly associated with malignancy, 29.7% of the malignant masses were assessed as benign on ultrasonography. Also, 48.6% of the malignant masses showed well-defined margins, 41.9% showed no calcifications, and 95.9% showed parallel shape. Histopathologic type of the malignant lesion may be of cause of the benign ultrasonography features, but PTC was the diagnosis in 83% of the 65 proven malignant masses in our study. These features may indicate eccentric malignant foci within a large benign mass or rather a slow growth rate with less aggressiveness for malignancies of large size; further evaluation with a larger number of malignant masses measuring 3 cm or larger is needed for clarification.
The malignancy rate of masses with inadequate cytology was 23.5%, which correlates with the previously reported broad range of malignancy rate in nondiagnostic cytology from 2% to 37% (28 –30). Selection bias may have an effect on the malignancy rate of surgically proven masses with inadequate cytology, as nodules with more suspicious features or high cancer risk factor are more likely to be treated surgically than by follow-up.
In the recent decade, many studies have focused on molecular testing that may provide additional information in the diagnosis of thyroid nodules (31). The presently popular BRAF, RET/PTC, and RAS mutations may be used in the differential diagnosis of large thyroid nodules, especially those diagnosed as suspicious for PTC on US-FNAB, when considering the false-negative or -positive results. Studies proving the efficacy of molecular testing, specifically used in the diagnosis of large thyroid masses, are anticipated.
There are several limitations in this study. First, the majority of patients underwent surgery because of the presence of symptoms or changes in lesion characteristics on ultrasonography. This may have brought about selection bias, which may have an effect on the false-negative rates of FNAB. Second, nearly 30% of the patients who were initially diagnosed with masses larger than 3 cm were excluded. When considering the initial cytologic diagnosis, 86% (101/118) and 28% (215/773) of masses initially showing indeterminate and benign cytology were excluded. This may have had an effect on the diagnostic performances, especially the false-negative rates in this study. Third, in patients with follow-up ultrasonography or US-FNAB, different radiologists with different experiences were involved in imaging interpretation, which may have provoked variability in assessment of these nodules. Strict size measurement criteria were not applied in the evaluation of size change among performers, so variability among performers may be present. Also, variability between the five cytopathologists in cytology interpretation was not considered. Fourth, only one radiologist retrospectively reviewed the images of thyroid nodules included, mostly to reduce the observer variability that may exist during review of US images. Different results may have been derived if two or more radiologists were involved. Last, not all the benign masses included in this study were confirmed with surgery.
In conclusion, US-FNAB appeared to be a relatively accurate method to evaluate thyroid nodules larger than 3 cm, with false-negative rates of about 2% or possibly somewhat higher for a benign diagnosis. Ultrasonography provides diagnostic information but the utility of ultrasonography cannot be ideally assessed from this study as we excluded patients who had inadequate, indeterminate, or suspicious for malignancy cytology readings but did not have thyroid surgery. Although ultrasonography flagged one of the two patients with a false-negative benign cytology, much larger series would be required to determine its utility in this setting.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.