
Abstract

While this study (1) is a large series relating to VCP post-thyroidectomy, the efficacy and safety of such injection are supported by the work of others (2 –4). Such vocal cord injection can be done as a transcutaneous or transoral office procedure, typically without antibiotics or steroids. The patient is observed for about 15–20 minutes after the procedure and then maintains voice rest for a period of time. In recent years there has been a substantial expansion of such in-office procedures, including laser laryngeal treatment, Botox laryngeal injection, laryngeal biopsy, and transnasal esophagoscopy (5). In the past, injection of polytetrafluoroethylene (Teflon) fell from favor due to problems of migration and granulomatous reaction. Certainly other treatment options exist for repair of postoperative VCP, including formal open thyroplasty, which involves a cervical skin incision, partial thyroid cartilage removal, and placement of silastic implant or other spacer material lateral to the vocal cord. This procedure may be combined with arytenoid adduction whereby the arytenoid cartilage is repositioned through suture placement to modify the desired vector of force on the repositioned paralytic cord so as to optimize the voice. Simpler and less invasive injection thyroplasty may be less suitable for patients with large posterior glottic gaps and may be less durable. The simplicity, safety, and effectiveness of injection thyroplasty have resulted in recent gains in its popularity. Lee and colleagues' work (1) emphasizes the importance of recognition and treatment of postoperative voice changes.
Reported Prevalence of Recurrent Laryngeal Nerve Paralysis
The reported prevalence of recurrent laryngeal nerve (RLN) injuries after thyroid surgery varies widely. A recent analysis of 27 articles reviewing over 25,000 patients undergoing thyroidectomy found the average temporary VCP rate was 9.8%. The rate of permanent VCP varied 10-fold, according to the method of examining the larynx, and ranged from 0% to 18.6% (6). With the advent of nationwide surgical outcome databases we have broad cross-sectional perioperative information, which may give insight into these issues. The Scandinavian quality register (SQR) for thyroid and parathyroid surgery, reporting in 2008 on 40 endocrine surgical units from Sweden and Denmark specializing in endocrine surgery, noted an immediate VCP rate of 4.3% (7). In the national U.K. British Association of Thyroid and Endocrine Surgeons (BAETS) audit a VCP rate of 2.5% was found (8). One must keep in mind that both Scandinavian and British quality registers derive from surgeon-reported data without routine postoperative laryngeal exam. For the SQR, the rate of VCP doubled when patients were subjected to routine laryngeal exam as opposed to postoperative laryngoscopy that was performed only in patients with persistent and severe voice changes. Administrators of these two national databases deem the rates of temporary and permanent RLN palsy to be severely underestimated (7,8).
Low rates of VCP quoted to patients preoperatively by surgeons and endocrinologists are often derived from reported series of patients treated at high volume expert centers with favorable and publishable results. It should be noted that in the United States 50% of thyroid surgery is performed by surgeons who perform fewer than five such procedures per year (9,10). It is therefore likely that the true incidence of VCP and severity of voice morbidity are underestimated.
Voice is a very personal attribute. Therefore paralytic dysphonia (and its accompanying paralytic dysphagia) is distressing and can trigger legal litigation. Surgeons operating on the thyroid may find the JAMA editorial “Moral Wounds: Complicated Complications,” which details the patient's perspective of post-thyroidectomy vocal cord paralysis, informative (11). A 6-year review of jury verdict reports of endocrine malpractice litigation from the U.S. Civil Court system showed that 50% of adverse events were related to thyroid surgery, of which 70% involved RLN injury. Mean plaintiff verdict award for RLN injury was $1 million and the maximum award was $2.5 million (12). Analysis of 30 cases retrieved from a U.S. computerized legal database covering 1987–2000 showed that seven out of nine patients with RLN injuries claimed a lack of informed consent (13).
Anatomy of the Larynx and Its Two Nerves
The larynx is composed primarily of the upper shield-shaped thyroid cartilage (which has a left and right lamina) that rests on the lower ring-like cricoid cartilage through the cartilaginous cricothyroid joint posteriorly. The midline notch in the thyroid cartilage represents the “Adam's Apple.” The vocal cords are two folds of epithelium-covered muscle projecting into the laryngeal lumen and are located approximately halfway down the thyroid cartilage. The two arytenoid cartilages, right and left, sit on the cricoid's posterior lamina and are the posterior attachments of the vocal cords. These insert anteriorly into the inner surface of the midline thyroid cartilage. The basic motion of the arytenoids is rotation. When rotating laterally, they cause abduction of the vocal cord; when rotating medially, they cause adduction of the vocal cord. Figure 1 shows the thyroid and cricoid cartilages of the larynx and the upper cervical trachea with the left thyroid cartilage lamina removed. Laryngeal musculature can be divided into those muscles that result in vocal cord adduction and those that cause vocal cord abduction. The thyroarytenoid muscle is also known as the vocalis muscle. It represents the main muscular substance of the vocal cord. It is one of the adductors while the posterior cricoarytenoid muscle is the main abductor. The cricothyroid muscle on the outer surface of the lower larynx is the only laryngeal muscle present within the thyroid surgical field. In this position the cricothyroid muscle, when active, acts to tilt the thyroid cartilage forward on the underlying cricoid cartilage and in this way tenses the vocal cord allowing for higher vocal registers and voice projection (Fig. 2).
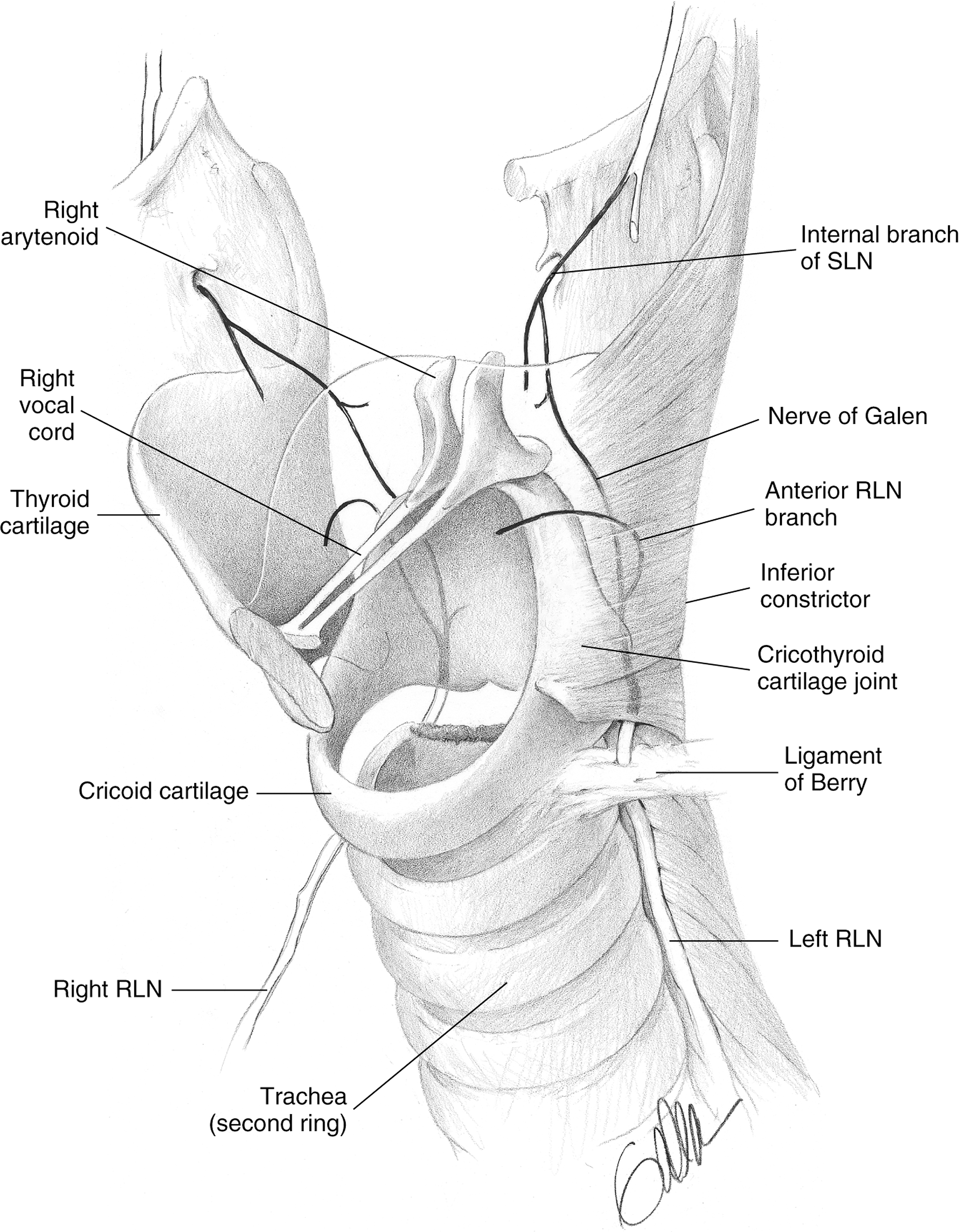
Laryngeal and recurrent laryngeal nerve (RLN) anatomy. SLN, superior laryngeal nerve. (Reprinted with permission: Randolph G [Ed] Surgery of the Thyroid and Parathyroid Glands 2003; Elsevier.)
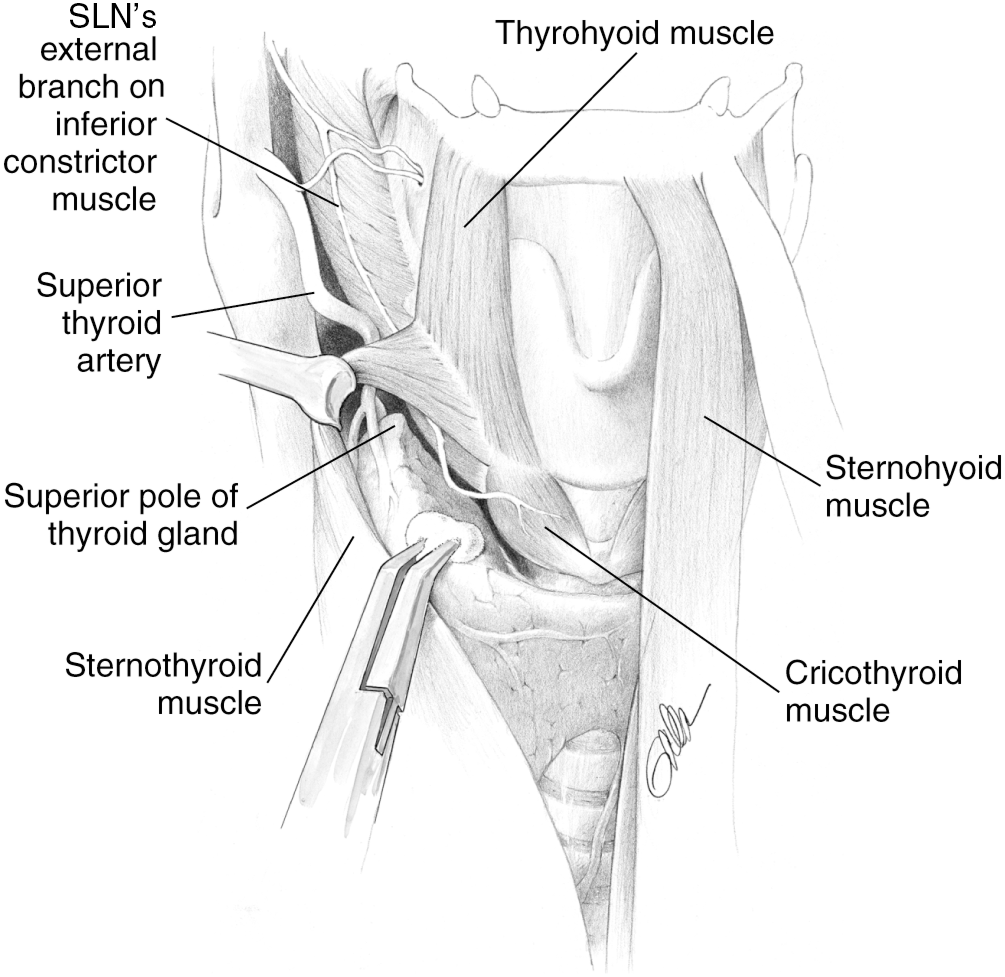
Superior laryngeal nerve (SLN) anatomy. (Reprinted with permission: Randolph G [Ed] Surgery of the Thyroid and Parathyroid Glands 2003; Elsevier.)
The RLN carries motor fibers to all intrinsic laryngeal muscles (except for the cricothyroid muscle) as well as to the inferior constrictor muscle of the pharynx, cricopharyngeus muscle, and sensory fibers from the larynx, upper esophagus, and trachea. It ascends the neck in the tracheoesophageal groove on the left and somewhat more obliquely on the right to the larynx in close relation to the posterior thyroid capsule (Fig. 1). The superior laryngeal nerve (SLN) branches from the vagus nerve in the upper neck and divides into an internal branch, which provides afferent supply for the supraglottic larynx. It descends further inferiorly as the external branch of the SLN (Extbr SLN) and is in close association to the thyroid superior pole, providing motor fibers to the cricothyroid muscle (Fig. 2).
Voice represents the passage of air exhaled through the partially closed and tensing vocal cords. The movement of exhaled air sets up an epithelial vocal cord cover oscillation known as the cord's mucosal wave. Higher registers are also controlled through cricothyroid muscle contraction, which slides the thyroid cartilage forward relative to the cricoid cartilage, which tenses the vocal cords. Any disruption in the luminal surface of the vocal cord results in a disruption of this process and a coarse change to the voice that is termed loosely “hoarseness.” The characteristic change that occurs from poor vocal cord apposition during phonation, as occurs with VCP, is more a breathy quality to the voice rather than true hoarseness. Laryngeal exam typically reveals an immobile cord which may be bowed/atrophic and laterally displaced to a variable degree typically described as paramedian. The resultant persistent glottic gap results in both air escape during phonation as well as, to variable degree, salivary and ingested liquid aspiration. The correction of this gap, as with injection medialization, can improve voice, swallowing, and effectiveness of cough (Fig 3).
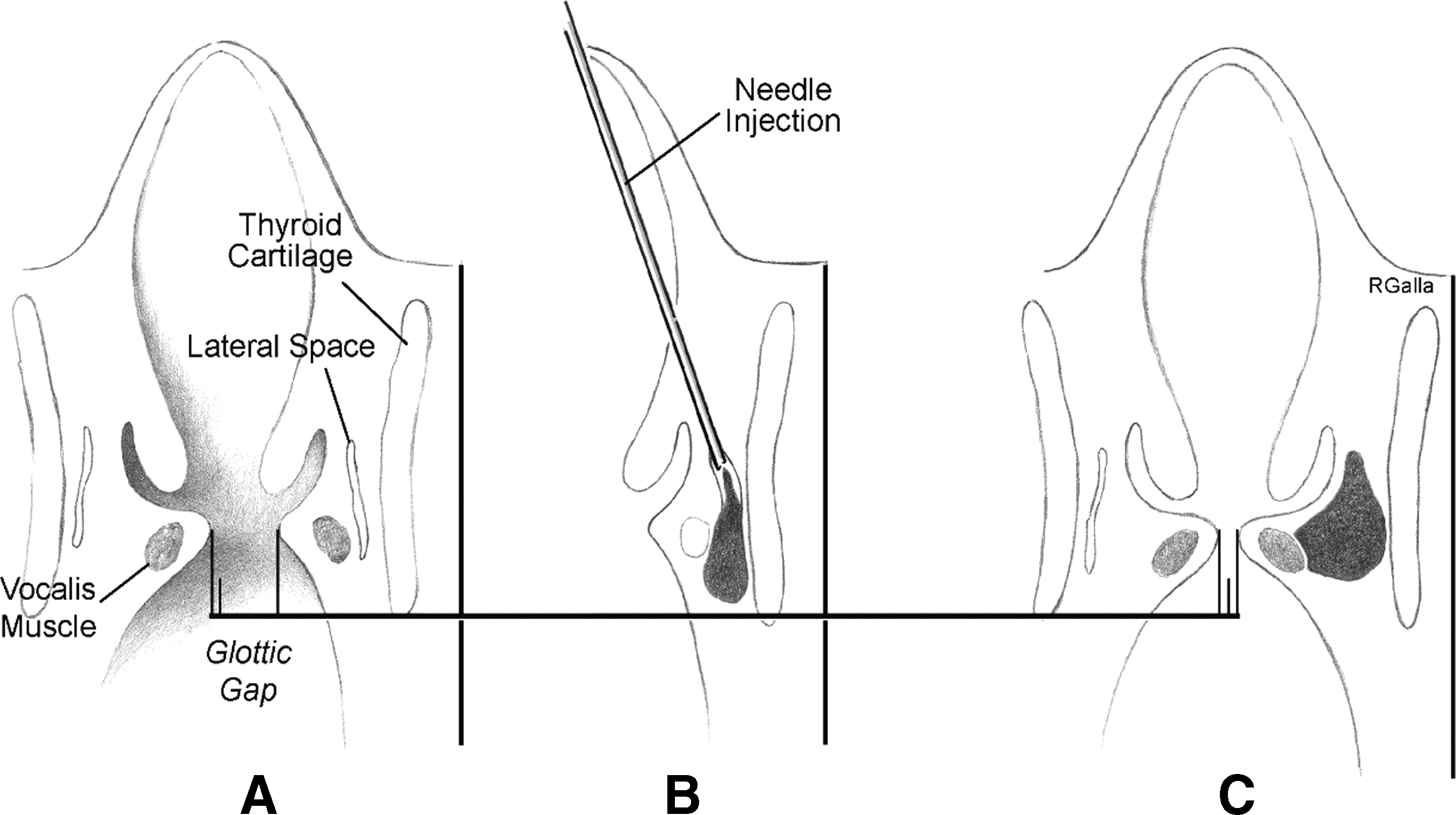
Vocal cord injection medialization.
Because of the Extbr SLN's role in projection and higher vocal registers it is also termed the “nerve of Amelita Galli-Curci” after the famous operatic soprano whose career in 1935 was brought to a ruinous end as a result of thyroid surgery under local anesthesia. The media wrote that postoperatively “the surprising voice is gone forever. The sad specter of a ghost replaces the velvety softness,” although details are controversial (14). Endoscopic laryngeal findings may be quite subtle in external branch injuries and must be confirmed through cricothyroid muscle electromyographic studies.
Voice and Glottic Exam
It is centrally important to recognize that in both preoperative and postoperative settings, VCP may be present without significant vocal symptoms. This basic fact is the rationale for the inclusion of glottic exam in all patients both preoperative and postoperative. The divergence of glottic function on laryngeal exam and voice symptoms is due to several factors including variable remaining cordal function, variability in paralytic cord position, and variability of contralateral cord compensation. It is common to observe improvement in symptoms in a patient with a stable VCP. Such improvement could be falsely interpreted by the less experienced observer as an indication that VCP has resolved. The correlate is also true that change in voice may derive from many sources and does not necessarily imply VCP. It is only the laryngeal exam that can accurately identify VCP.
Voice Symptoms with Intact Vocal Fold Mobility
It is well recognized that both subjective and objective postoperative voice changes commonly occur in patients after thyroidectomy with intact vocal fold motility (i.e., without VCP). Typical symptoms are often transient and may consist of voice fatigue and difficulty with high pitch. Objective findings typically include decrease in voice fundamental frequency and vocal range (15,16). Typically there is progressive normalization within 3–6 months postoperatively (17).
In several large studies of patients without VCP after thyroidectomy, subjective voice complaints occurred in 30–80% of patients (18 –22). Also, a variety of objective voice analysis alterations, including alteration in fundamental frequency and decrease in maximum sound pressure, can be seen transiently without vocal cord paralysis in these patients (23). Some of these changes may in fact be long lasting. One retrospective analysis (24) at a mean of 4 years after uncomplicated thyroidectomy (i.e., without VCP) in a cohort of 60 patients identified a high prevalence of nonspecific voice changes (28%) and impaired swallowing (15%). The proposed mechanisms for voice alteration despite grossly normal RLN function include partial/subclinical RLN dysfunction and unrecognized, partial/subclinical Extbr SLN dysfunction. Other factors that may be etiological include endotracheal tube–associated vocal cord/laryngeal injury, direct cricothyroid muscle injury, regional surgical effects such as strap muscle denervation and regional scarring/laryngeal tethering, as well as coincident voice change from nonthyroid pathology. In addition to voice changes, subjective nonspecific upper aerodigestive symptoms including dysphagia are common after thyroidectomy but are infrequently recorded or reported. A swallowing impairment score developed as a subjective self-evaluation questionnaire demonstrated that swallowing problems occur in the first week in over half of patients undergoing thyroid surgery and may last for more than 3 months (23). Possible discrete injuries to the perithyroidal neural plexus, including afferent fibers innervating the pharyngeal and laryngeal structures, might underlie such symptoms.
Vocal Cord Paralysis Without Voice Symptoms
It is common for early postoperative endotracheal tube–associated vocal cord edema to offset VCP symptoms in the early postoperative period. In the later postoperative period VCP can be asymptomatic due to variable remaining cordal function, variability in paralytic cord position, and variability of contralateral cord compensation. It is common, for example, that with permanent VCP, symptoms improve due to contralateral cord compensation, falsely suggesting that the VCP has resolved (25,26). In a recent study of 98 patients with VCP, voice was normal in 20% and improved to normal in an additional 8%. Overall nearly one third of patients with VCP were or became asymptomatic (27). The fact that the surgical mishap was asymptomatic does not lessen its significance as a potential source of learning for the surgeon who seeks to relate the surgical conduct of that case to its postoperative outcome. There is also significance of asymptomatic VCP in terms of swallowing and potential for increased respiratory morbidity if the contralateral nerve is operated on in the future.
Preoperative Vocal Cord Assessment: The Rationale
There are several reasons in favor of routine preoperative performance of laryngeal exam. First, as noted, given that nearly one third or more of patients with unilateral RLN paralysis are asymptomatic, voice changes cannot be relied on as predictor of vocal cord function. Two recent studies (26,28) investigating preoperative voice changes and VCP found sensitivity of voice change predicting VCP ranging from 33% to 68% and a positive predictive value in one study of only 38%. In one of these studies (26) the presence of preoperative RLN palsy had an excellent predictive value for finding invasive thyroid cancer at surgery (sensitivity 76%, specificity 100%). The importance of knowing there is invasive disease preoperatively may allow for more appropriately aggressive surgical planning (as it relates to the airway and regional nodal basins), more detailed preoperative imaging, and more specific preoperative patient counseling. Aside from its significance in detecting invasive disease many studies document a low but significant number of patients undergoing surgery (even with benign disease) with preoperative idiopathic VCP (29). Such nerve injuries not detected preoperatively will likely be considered as resulting from the ensuing thyroid surgery on postoperative review. Also, preoperative recognition of VCP is essential in planning the procedure since management of the RLN found invaded at surgery is based in part on knowledge of its preoperative function (26). The surgeon is empowered in the operating room by knowledge of preoperative laryngeal function. Finally, if one is committed to accurate quality assessment through postoperative vocal cord exam, then the rational interpretation of such postoperative assessment implicitly requires preoperative examination.
Despite this information, the SQR indicates that preoperative laryngeal exam was performed in only 54% of patients in its database. For patients scheduled for thyroid cancer surgery, this figure was only slightly higher at 63%. Only 60% of patients undergoing revision thyroid surgery had preoperative laryngeal exam (7). The BAETS audit found preoperative laryngeal exam was performed in only 38% of patients prior to thyroid surgery (8). In Hundahl and colleagues' well-known report (30) from the U.S. and German Thyroid Cancer Study Group of 5563 patients undergoing thyroid cancer surgery, preoperative hoarseness and voice change were noted in 8.2% of patients. Preoperative laryngeal exam, however, was performed in only 6.1% of the 5563 patients. Not surprisingly, one of the study's main recommendations was that preoperative laryngoscopy be performed more frequently (30). National Comprehensive Cancer Network (NCCN) guidelines describe preoperative vocal cord paralysis as a “highly suspicious factor” for cancer and need for surgery. NCCN guidelines recommend preoperative laryngeal exam for patients with papillary follicular, Hürthle cell and medullary cancers but not for patients with anaplastic cancer (31). British Thyroid Association (BTA) guidelines recommend preoperative laryngeal exam for patients with preoperative voice abnormalities and for patients undergoing surgery for cancer (31). The most recent 2009 American Thyroid Association (ATA) revised guidelines for management of thyroid nodules and thyroid cancer make no reference at all to laryngeal exam assessment or assessment of vocal cord paralysis in thyroid nodule work-up or in preoperative or postoperative management for patients with thyroid cancer (32).
Postoperative Vocal Cord Assessment: The Rationale
Given the clear-cut divergence in voice symptoms and objective vocal cord function, it appears that routine postoperative laryngeal exam is required in all patients undergoing thyroid surgery if surgeons are to have accurate information regarding their surgical outcomes. We know that symptomatic assessment of postoperative patients is inadequate as a neural postsurgical outcome measure. The SQR data show the documented postoperative rate of VCP doubles if postoperative laryngeal exam is performed routinely as compared to when only symptomatic patients are examined (7). Despite the importance of postoperative laryngeal exam in surgical outcome quality analysis, the BAETS audit showed that postoperative laryngeal exam was only performed in 21.5% of patients (8). Postoperative VCP has significant implications for patients' swallowing function and in patients for whom contralateral surgery may become necessary, for cancer recurrence, for example. While the BTA guidelines recommend postoperative laryngeal exam only in the setting of voice disturbance of greater than 2 weeks' duration postoperatively, there is no mention of laryngeal exam postoperatively in either the NCCN or ATA thyroid cancer guidelines (31 –33).
Conclusions
Traditionally the risk for recurrent laryngeal nerve injury after thyroidectomy quoted to patients derives from limited expert series and likely does not reflect the true prevalence in many clinical settings. The true rate of neural injury in various clinical settings cannot be known unless each surgeon with his or her unique practice mix examines the larynx on all patients pre- and postoperatively as a standard routine for quality. Moreover, voice changes are in fact quite common, but they cannot be distinguished from nerve injury without routine pre- and postoperative glottic and laryngeal exam.
To optimize surgical learning and provide valid accurate surgical outcome data to patients, preoperative and postoperative laryngoscopy should become part of the current quality assessment of all patients undergoing thyroidectomy, in line with modern trends towards improved postoperative surgical outcome quality assessment, improved transparency, and accountability. This is the only reliable way that the true prevalence of RLN injury can be accurately determined. The glottis needs to be examined if we are to know how we have done. We need to know how we have done in order to learn how to do better. The larynx is centrally important in modern thyroid surgical practice.