
Abstract
Background:
Adverse drug reactions (ADRs) rank as one of the top 10 leading causes of death in the developed world, and the direct medical costs of ADRs exceed $100 billion annually in the United States alone. Pharmacogenomics research seeks to identify genetic factors that are responsible for individual differences in drug efficacy and susceptibility to ADRs. This has led to several genetic tests that are currently being used to provide clinical recommendations. The Canadian Pharmacogenomics Network for Drug Safety is a nation-wide effort established in Canada to identify novel predictive genomic markers of severe ADRs in children and adults. A surveillance network has been established in 17 of Canada's major hospitals to identify patients experiencing specific ADRs and to collect biological samples and relevant clinical history for genetic association studies. To identify ADR-associated genetic markers that could be incorporated into predictive tests that will reduce the occurrence of serious ADRs, high-throughput genomic analyses are conducted with samples from patients that have suffered serious ADRs and matched control patients.
Summary:
ADRs represent a significant unmet medical problem with significant morbidity and mortality, and Canadian Pharmacogenomics Network for Drug Safety is a nation-wide network in Canada that seeks to identify genetic factors responsible for interindividual differences in susceptibility to serious ADRs.
Conclusions:
Active ADR surveillance is necessary to identify and recruit patients who suffer from serious ADRs. National and international collaborations are required to recruit sufficient patients for these studies. Several pharmacogenomics tests are currently in clinical use to provide dosing recommendations, and the number of pharmacogenomics tests is expected to significantly increase in the future.
Adverse Drug Reactions
An ADR is an undesirable effect associated with a medication that occurs with normal use (2). ADRs may be evident within minutes or years after exposure and may range from minor reactions such as self-limited skin rash to more serious and life-threatening events such as heart failure or liver injury. Severe ADRs have accounted for a significant number of drug withdrawals from the market; however, the ADRs may not be recognized for years after a drug has been on the market (3). Without a means to identify patients at risk for developing an ADR, market withdrawal can leave those patients who would have benefited from these drugs without access to potentially effective therapies. Indeed only a year ago the Food and Drug Administration (FDA) issued a warning of risk of severe liver injury, including liver failure, and death with use of propylthiouracil (PTU) in adult and pediatric patients (4). PTU was approved 63 years ago for the treatment of Graves' disease, and is still commonly used. Moreover, in certain situations it is the preferred medication for Graves' disease, for example, in patients in their first trimester of pregnancy or in patients who are allergic to methimazole. The FDA identified 32 cases (22 adults and 10 children) that developed liver injury with PTU; of the 22 adult cases 12 deaths and 5 liver transplants were identified, and of the 10 pediatric cases, there was 1 case of death and 6 liver transplants.
The debilitating and potentially lethal consequences of serious ADRs are ranked as the fourth leading cause of death in the United States, claiming 100,000–218,000 lives and causing >2 million severe reactions annually in the United States (5 –7). The health care costs of ADRs exceed $100 billion each year in the United States alone (5 –8). For most medications ADRs are rare, but collectively account for an alarming 7% of all hospital admissions (6,9).
ADRs can have terrible consequences for patients, including death, permanent disability, treatment cessation, or reduced adherence to medications. However, the risk factors for severe ADRs remain largely unclear, and the selection of specific drugs for an individual patient is often an empiric exercise (10). This highlights the fact that one of the most difficult issues faced in clinical practice is deciding which drug and which dose is best for each patient.
The Genetic Component of ADRs
Individual response to medication is influenced by many factors such as age, organ function, and drug interactions. In addition to these factors, genetic differences between patients also account for a significant proportion of drug response variability (8,10 –13). In many cases, drug toxicity is concentration dependent, and is determined by the agent's concentration both at its target site and in plasma. The effective concentration of a drug depends on its absorption, distribution, metabolism, and elimination. Genetic variation in drug-metabolizing enzymes and drug transport systems may lead to large differences in drug exposure between individuals, resulting in toxicity or ineffective drug treatment (14,15). Genetic contributions to variability may also be caused by pharmacodynamic alterations, such as receptor density or affinity. Unlike other factors influencing drug response, inherited determinants remain stable throughout a person's lifetime and therefore provide health care professionals with reliable diagnostic means to predict and prevent ADRs.
The culmination of landmark advances in genetics such as sequencing the human genome (16), the International HapMap project (17), and the development of innovative new technologies for high-throughput genotyping and DNA sequencing are improving the ability to identify genetic factors associated with drug toxicity. The goal of pharmacogenomics is to identify the genetic factors involved in an individual patient's reaction to a medication to avoid ADRs and maximize drug efficacy. Pharmacogenomics studies often compare subjects treated with a specific drug to identify genetic variants that are associated with drug response or the occurrence of an ADR. Once a pharmacogenetics variant is identified and validated, a diagnostic test for the presence of the variant can be developed to predict a patient's response to the specific drug. Pharmacogenomics may improve the benefits and reduce the risks of medications by determining which patients are most likely to respond favorably to a specific medication and by predicting in whom there is a greater risk for an ADR (18).
Examples of diagnostic tests to guide pharmacotherapy and prevent severe ADRs include tests for UGT1A1 variants for life-threatening irinotecan-induced toxicity (19,20), thiopurine S-methyltransferase (TPMT) variants azathioprine-related myelosuppression (21,22), CYP2C9 and VKORC1 variants to guide warfarin dosing (23,24), HLA-B*1502 testing for carbamazepine-related Stevens–Johnson syndrome and toxic epidermal necrolysis (25), and HLA-B*5701 testing to predict severe hypersensitivity to abacavir (26 –28). These tests are recommended by the FDA in the United States or are in the process of being introduced into the clinic. “Point of care” testing for these markers may soon be widely available once cost-effective test methodology is developed.
Need for National and International Collaborations and Active ADR Surveillance to Address the Unmet Medical Need of Severe ADRs
The safety of medications is an international concern that has attracted the attention of policy makers and clinicians in the United States, Europe, Canada, and elsewhere. Removing medications from the market that have been associated with serious ADRs is not an optimal long-term solution because this can leave seriously ill patients without therapeutic options. Rather, the solution lies in finding the mechanisms underlying specific ADRs so that these medications can continue to be used in patients for whom there is therapeutic benefit and better manage the risk among those at high risk of an ADR.
The rarity of many drug-induced severe ADRs and the absence of effective regulatory surveillance make it extremely difficult for any one research group to accrue sufficient numbers of patients with a specific rare ADR to study its genetic determinants. Even in countries such as Canada, where ADR reporting is mandatory for pharmaceutical manufacturers, <5%–20% of ADRs are reported (29 –31). Thus, national and international collaborations are critical in identifying sufficient numbers of patients with specific rare ADRs to discover and validate ADR-causal genetic variants.
The Canadian Pharmacogenomics Network for Drug Safety
The Canadian Pharmacogenomics Network for Drug Safety (CPNDS) is a nation-wide multidisciplinary consortium of researchers from hospitals, universities, and research institutes that was established to improve drug safety through the identification of predictive genetic markers of severe ADRs in patients. CPNDS has catalyzed national and international collaborations in ADR research and established an active surveillance network for ADRs across Canada (32). The ultimate goal of CPNDS is to provide additional clinical genetic information to the patient and physician to improve the selection of safer and more effective therapeutic options.
The CPNDS active ADR surveillance network in Canada links 13 pediatric teaching hospitals across the country (Fig. 1), as well as a growing number of adult hospitals in British Columbia and other jurisdictions. This initiative harnesses the unique Canadian advantage of a single public-payer health care system that is internationally respected for delivering high-quality standardized care and provides critical access to patient information. The network relies on CPNDS-employed active ADR surveillance clinicians at each site to identify patients who have developed serious ADRs and enroll these patients in the CPNDS program. Each site also has collaborating site investigators: senior scientists or clinicians who mentor the surveillance clinicians and frequently give presentations or workshops to engage both the local scientific and medical community. In many cases, these site investigators conduct research projects in collaboration with other CPNDS researchers. Overall, the active surveillance system of CPNDS allows researchers and clinicians to capture ADRs in the Canadian population, and provide a more complete picture of ADR trends.
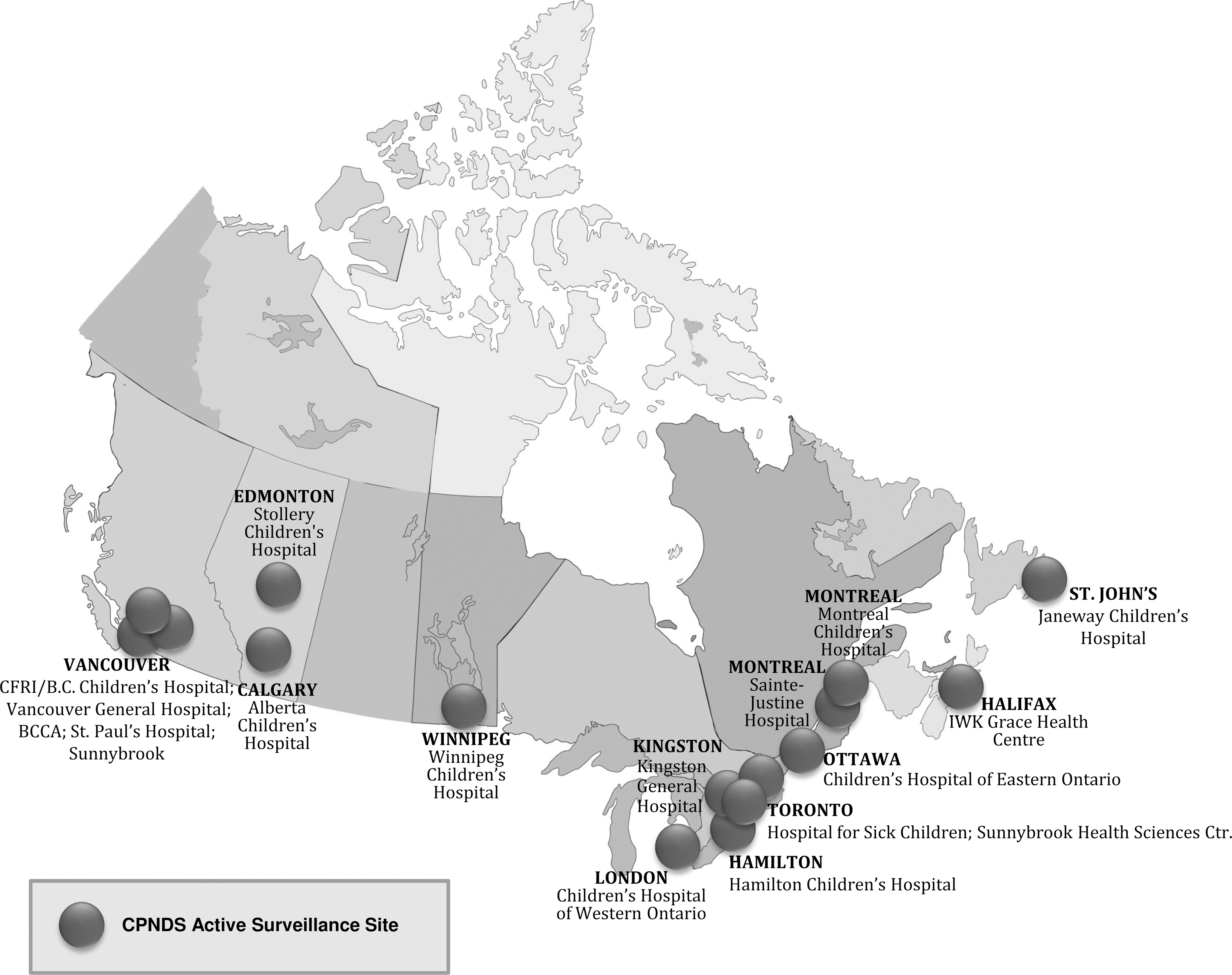
Geographic depiction of the hospitals involved with Canadian Pharmacogenomics Network for Drug Safety (CPNDS) (May 2010).
Training of the ADR surveillance clinicians includes ADR identification and reporting, patient recruitment and enrolment, advertising the project within institutions, linking with other healthcare professionals in the institutions, and how to securely transfer data to the CPNDS database. The ADR clinicians and site investigators are provided with training and reference manuals that outline all of the procedures and protocols for each site, including project advertisement, local laboratory setup for blood draws, DNA sample collection instructions (blood, buccal sponges, or saliva), shipping instructions, instructions for data entry, target drug lists, and an extensive collection of reference publications.
Accurate and detailed clinical data are critical factors in the discovery of ADR-associated biomarkers. CPNDS surveillance clinicians are experienced personnel trained to recognize and document the detailed clinical histories of patients that suffer severe ADRs, including details of the ADR, suspected causative drugs, concurrent medications, past and current medical conditions, ancestry, as well as other relevant patient information. A secure, password-protected database stores the demographic and clinical information on a secure server. The clinical judgment of ADR surveillors and site investigators are relied upon to evaluate possible confounding factors on ADR causality such as disease state or interacting drugs. The causality of ADRs are graded using two methods, the World Health Organization Collaborating Centre for International Drug Monitoring Causality Assessment Algorithm (33) and the Naranjo ADR Probability Scale (34). Previous pharmacogenomics studies have often been limited by the lack of detailed prospective case data, such as missing ancestry information, comorbid conditions, medication doses, or concurrent medication information (35). Importantly, CPNDS ADR surveillance clinicians are trained to collect these critical data in a comprehensive manner to maximize the value of patient samples and to accurately characterize the ADR to ensure correct phenotypes.
CPNDS Pharmacogenomics Drug Targets
As of March 2010, the CPNDS network has identified >2900 cases of severe ADRs, and this number continues to climb as ADR surveillance continues and more national and international collaborating surveillance sites are added. CPNDS pharmacogenomics research has focused on specific ADRs that meet rigorous criteria in a prioritization process that is designed to maximize the benefit from finite research funding sources. Importantly, the ADRs that have been studied thus far include those that confer life-threatening or permanently disabling conditions for which sufficient patients have been recruited. This drug target algorithm also considers other factors, including the likelihood of association between genetic variants and ADR, how well the metabolism of the drug is understood, and the economic and social burden of the ADR, as well as others. Since its inception, CPNDS has identified predictive biomarkers for two severe ADRs: cisplatin-induced hearing loss and codeine-induced infant death. Studies are currently in progress for other severe ADRs of interest.
Cisplatin-induced deafness
Cisplatin is a chemotherapeutic agent that is widely used in both pediatric and adult oncology and is highly effective against solid tumors, including several advanced thyroid cancers. However, it causes severe hearing loss (ototoxicity) in a subset of patients. Cisplatin-induced ototoxicity has been documented to occur in over 50% of children (36 –40) with a significant negative impact on learning and development (38,41). Upon discovering this ADR in patients, cisplatin dosages are typically reduced or halted in an attempt to minimize further hearing loss. To identify potential genetic variants linked to cisplatin ototoxicity, we compared the single-nucleotide polymorphism profiles of over 1900 single-nucleotide polymorphisms in drug-metabolism-related genes in patients who suffered moderate to severe hearing loss (Common Terminology Criteria for Adverse Events grade 2–4) versus patients who did not develop any hearing loss (Common Terminology Criteria for Adverse Events grade 0) after receiving standard doses of cisplatin. We identified two variants in the TPMT gene (rs12201199; odds ratio 17.0, p-value 0.00022) and the catechol O-methyltransferase (COMT) gene (rs9332377; odds ratio 5.5, p-value 0.00018) (42) that were consistently associated with cisplatin-induced hearing loss in two cohorts of patients. Combined, these risk alleles in TPMT or COMT were carried by 48% of cases (odds ratio 12.1, p-value 3.4 × 10−8). These variants are in linkage disequilibrium with low enzyme activity variants in their respective genes. These two methyltransferases both function in the methionine pathway and use the same S-adenosylmethionine methyl donor substrate (35,36). In the presence of cisplatin, this S-adenosylmethionine substrate has been shown to significantly increase the renal toxicity of cisplatin and we hypothesize that this may be related to cisplatin ototoxicity as well (43). Through international collaborations, CPNDS is working to identify additional cisplatin toxicity-related variants and implement clinical tests for the benefit of patients and physicians. Current alternatives to standard cisplatin therapy include the addition of otoprotective agents, cisplatin dose adjustment, and alternative chemotherapies such as carboplatin that are less ototoxic, but often also less effective.
Codeine-induced infant mortality
We previously reported a case of opioid-induced death in an infant caused by codeine. The deputy chief coroner of Ontario, Canada, identified a lethal opioid overdose in a 13-day-old infant after the mother was given Tylenol #3 (a combination of 300 mg acetaminophen and 30 mg codeine) for obstetric pain relief following episiotomy at the time of delivery. Genotyping of the mother revealed a CYP2D6 gene duplication and UGT2B7*2 variant that increased CYP2D6 activity. This resulted in substantially increased levels of active morphine and morphine-6-glucuronide metabolite in the mother's breast milk and the infant's blood, leading to fatal central nervous system depression in the infant (44 –46). A follow-up study of codeine use in 72 mothers confirmed the association between CYP2D6 duplication genotype and central nervous system depression (47). Before this study, codeine had been considered compatible with breast feeding by the American Academy of Pediatrics (48) as well as according to a major reference textbook for drug use in pregnancy and lactation (49). However, following this research, the next edition of this text had changed to include this information with more detailed recommendations (50). More recently, CPNDS investigators identified a fatal case of codeine intoxication in a 2-year-old patient who underwent an elective adenotonsillectomy (51). CYP2D6 genotyping of this patient revealed a functional duplication of the CYP2D6 gene, resulting in the ultrarapid-metabolizer phenotype. CPNDS is working with FDA and Health Canada to raise awareness of this health risk to prevent future cases through press releases by FDA and Health Canada, information warnings on the FDA and Health Canada Web sites, and a change to the codeine drug label. Additional studies are underway to evaluate the benefits of prospective testing to identify patients at risk for this severe ADR.
Future Perspective and Application to Thyroid Diseases
The overarching goals of CPNDS are to identify the mechanisms of serious ADRs and to provide relevant clinical genetic information to the patient and physician to improve the selection of safer and more effective therapeutic options. CPNDS aims to translate clinically important pharmacogenomics findings through ongoing communication with drug regulators (Health Canada, FDA, and the European Medicines Agency). Once genetic variants are identified and developed into predictive diagnostic tests, better risk–benefit therapeutic decision making will be possible for patients at high risk of serious ADRs. In the case of thyroid medications this would have significant implications to the management of thyroid disorders. For example, if a pharmacogenomics test were developed that can predict which patients are likely to develop liver failure when treated with PTU, or which patients are at high risk for agranulocytosis when treated with PTU or methimazole, it will have significant impact on the management of thyrotoxicosis. Discovery of gene variants associated with serious ADRs will also have implications on drug labeling and clinical practice guidelines.
Disclosure Statement
The authors declare that no competing financial interests exist.
Footnotes
Portions of this review were presented at the Spring 2010 Meeting of the American Thyroid Association, “Thyroid Disorders in the Era of Personalized Medicine,” Minneapolis, Minnesota, May 13–16, 2010.