
Abstract
Background:
Personalizing treatment for papillary thyroid cancer (PTC) requires a multidisciplinary approach. The surgical management of PTC has long been based on retrospective studies focusing on endpoints that are of debatable significance. There is considerable debate in the literature regarding the optimal initial treatment for PTC. Many of these issues are discussed in this review. These debates have hindered the development of a tailored treatment strategy.
Summary:
The ability to optimally personalize a surgical plan for the treatment of PTC is ultimately dependent on an understanding of the biological behavior of that individual patient's tumor. We are at the genesis of an age where molecular biology advances endeavor to profile a patient's tumor behavior. This review summarizes current strategies for managing PTC, where we are with personalizing surgery for these patients, and where we hope to go. Thyroid surgery is one of the newest fields for the application of minimally invasive techniques and can now be accomplished endoscopically or with robotic assistance in many patients who therefore may benefit from these alternative approaches.
Conclusion:
When treating a patient with PTC, it seems prudent to weigh the many factors discussed in this review to individualize the most optimal surgical plan.
Introduction
The inability to accurately identify the subsets of patients who are at greater risk for recurrence of PTC before primary treatment has in part spawned these debates and has hindered the development of a tailored treatment strategy. Personalizing treatment for PTC requires a multidisciplinary approach. The available evidence-based data and lack thereof should be well understood by the practitioners caring for a patient with PTC so as to tailor treatment accordingly.
The surgical management of PTC has long been based on retrospective studies focusing on endpoints that are of debatable significance. The ability to optimally personalize a surgical plan for the treatment of PTC is ultimately dependent on an understanding of the biological behavior of that individual patient's tumor. We are at the genesis of an age where molecular biology advances endeavor to profile a patient's tumor behavior to allow for a tailored treatment strategy. This review summarizes where we are with personalizing surgery for PTC and where we hope to go.
Individualizing the Surgical Plan for the Thyroid and Central Compartment in Patients Undergoing Initial Surgery for PTC
The rationale for total thyroidectomy for PTC identified preoperatively includes the frequent multifocal nature of the disease, the ability to reduce the risk of recurrence and to facilitate radioactive iodine treatment, and the use of serum thyroglobulin levels and whole-body radioiodine scans during follow-up. Two Mazzaferri et al. studies support that total thyroidectomy reduces the risk of recurrence for PTC and perhaps improves survival (4,5). Most surgeons agree now that a total thyroidectomy is preferred over a thyroid lobectomy for the majority of patients with known PTC before surgery (6).
Today, the advent of high-resolution ultrasonography and highly sensitive serum thyroglobulin assays as methods employed for follow-up of PTC have helped to create the contention surrounding elective CND. Although most would agree that patients should undergo formal central lymph node dissection as designated by the American Thyroid Association (ATA) consensus statement (7) on CND for clinically apparent lymph node metastases (macroscopic lymph nodes), there is ongoing debate regarding prophylactic central lymph node dissection in the clinically negative central N0 neck, especially for those patients deemed low risk with early stage disease.
Cervical lymph node metastasis occurs commonly in PTC. The prevalence ranges from 20% to 90%, with an average of 60% (7 –10). Lymph node metastasis is thought to be an independent risk factor for local recurrence (11,12). Recurrences rates are high in patients with macroscopic but not with microscopic lymph node involvement. Bardet et al. reported a 10%–30% prevalence of recurrence associated with macroscopic lymph node involvement, whereas those without had a much lower recurrence rate (13). This certainly argues for compartment-oriented nodal dissection when gross nodal disease is present to help reduce the risk of nodal recurrence in the neck. To further confound the situation, despite earlier reports of no adverse effects on survival, emerging evidence from large population-based studies demonstrates an increase in mortality with regional lymph node metastases (14,15). A major limitation is that all of these studies suffer from many confounders that make it difficult to interpret the significance of the findings for and against elective CND.
The ATA published guidelines for thyroid nodules and well-differentiated thyroid cancer in 2006 and recommended routine CND for PTC, but failed to distinguish between therapeutic and elective indications (16). In these guidelines, they indicated that “routine CND should be considered for patients with PTC.” They based this recommendation on the possibility that this might improve survival, might reduce the risk for nodal recurrence, and could be achieved with low morbidity. This aspect of the initial guidelines led to considerable debate. The literature often cited in favor of CND is frequently difficult to interpret due to the failure to distinguish between therapeutic and elective/prophylactic indications and extent of dissection. Due to these issues, the ATA's second edition of these guidelines (6) took a softer stance on the subject. The recommendation now states that therapeutic CND for patients with clinically involved central or lateral neck lymph nodes should accompany total thyroidectomy to provide clearance of disease from the central neck. Prophylactic central-compartment neck dissection (ipsilateral or bilateral) may be performed in patients with PTC with clinically uninvolved central neck lymph nodes, especially for advanced primary tumors (T3 or T4). Near-total or total thyroidectomy without prophylactic CND may be appropriate for small (T1 or T2), noninvasive, clinically node-negative PTCs and most follicular cancer. Further, these guidelines go on to state that these recommendations should be interpreted in light of available surgical expertise. For patients with small, noninvasive, apparently node-negative tumors, the balance of risk and benefit may favor simple near-total thyroidectomy with close intraoperative inspection of the central compartment with compartmental dissection only in the presence of obviously involved lymph nodes. This approach may increase the chance of future locoregional recurrence, but overall this approach may be safer in less experienced surgical hands (6).
The ATA consensus statement on CND (7) emphasizes that it is important to define the terminology used to classify the procedure. An elective or prophylactic lymph node dissection involves removing lymph nodes that are normal on preoperative and or intraoperative assessment (7). A therapeutic lymph node dissection involves removing lymph nodes that are clinically or pathologically abnormal based on examination, imaging, or intraoperative assessment. The goal of defining the terminology and classification scheme for CND is to allow investigators to communicate without ambiguity and compare the efficacy of these interventions. For the first time, this consensus statement defines the extent of CND as unilateral or bilateral. Bilateral CND is preferred as the initial management of clinically involved central nodes with therapeutic intention. However, there is controversy regarding whether the extent of dissection needs to be ipsilateral to the thyroid tumor alone or bilateral (17,18). If any surgical treatment of central neck nodes is considered necessary or appropriate, unilateral CND may be a reasonable alternative to bilateral CND, especially as initial management of the clinically negative central N0 neck to minimize the risk of associated potential complications. The consensus statement outlines and standardizes the boundaries for the CND. In particular, the CND should include levels VI and VII lymph nodes from the cricoid cartilage down to the innominate artery (Figs. 1 and 2). Operative reports should clearly describe the extent (unilateral vs. bilateral) and the intent (elective vs. therapeutic) of CND. Lack of standardized reporting has been partially responsible for the debate regarding the role of elective or prophylactic CND in PTC.
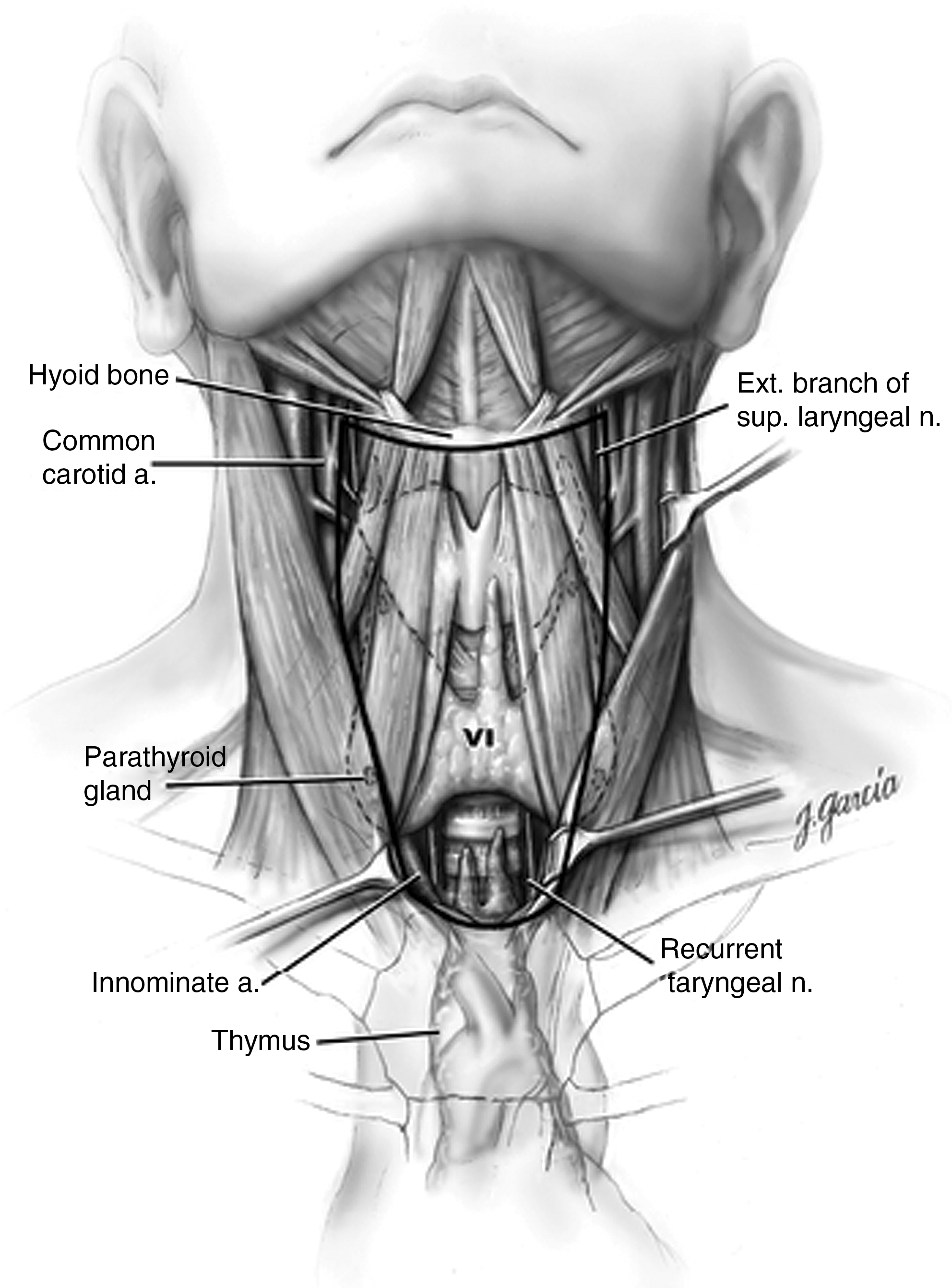
Schematic anterior view of the neck indicating boundaries of the central neck compartment (level VI): level VI is bounded superiorly by the hyoid bone, inferiorly by the sternal notch, laterally by the carotid arteries, anteriorly by the superficial layer of the deep cervical fascia, and posteriorly by the deep layer of the deep cervical fascia. The central compartment dissection as defined by the American Thyroid Association consensus statement uses these boundaries for dissection except that the superior border is defined by the cricoid cartilage and the inferior border the innominate artery to include level VII. Reprinted from ATA Surgery Working Group et al. (7) with permission.
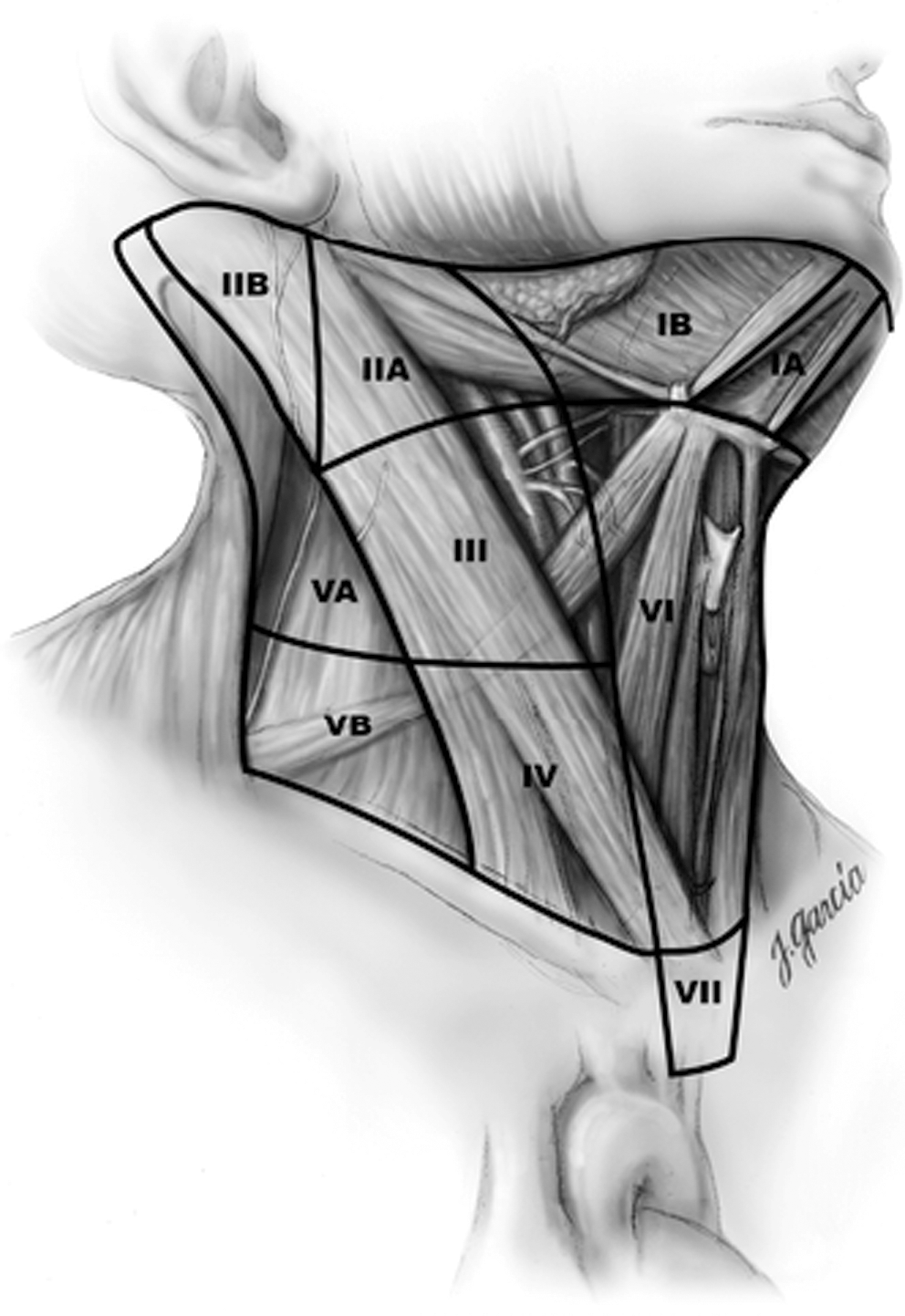
Schematic right anterior oblique view indicating levels of the neck and upper mediastinum (level VII) relevant to neck dissection. Reprinted from ATA Surgery Working Group et al. (7) with permission.
The proponents of elective/prophylactic central lymph node dissection rationalize that the procedure removes potential sources of recurrence, increases the accuracy of staging for radioactive iodine ablation, permits accurate long-term surveillance, and avoids the potential morbidity of a reoperation. Those who oppose elective/prophylactic central lymph node dissection believe that the logic for routine removal of nodes that may harbor subclinical metastases is flawed. If removal of subclinical metastases alone were an indication for surgery without an appreciation for the clinical significance of this disease, which certainly is debatable, then the same should theoretically apply to the lateral neck. Careful review of the literature finds no clear evidence of benefit in terms of lower recurrence or mortality rates for total thyroidectomy with prophylactic/elective CND. The only consistent finding is a higher rate of hypoparathyroidism for this group. Opponents also fear that if prophylactic/elective CND were universally adopted by all surgeons performing thyroidectomy, the risk of hypoparathyroidism and recurrent laryngeal nerve injury may increase in the absence of significant oncologic benefit to the patient (19 –21). Although many very experienced surgeons have published very low complication rates after total thyroidectomy, those results should not be extrapolated to the majority of surgeons doing thyroid surgery who are not routinely performing CND (22). Sosa et al. found that high-volume surgeons (defined as doing >100 cases = 5 years) had 75% fewer complications than low-volume surgeons (4.3% vs. 16.1%) (23). There are no similar comparative studies done for outcomes related to central lymph node dissection.
Lateral Neck Dissection for PTC
In contrast to the controversy over indications for elective CND in PTC, the indications for lateral neck dissection are clearer. Lateral neck dissection for PTC should be performed in a compartment-oriented manner when there is clinical or cytopathologic evidence of PTC in a lateral neck lymph node. Lymph nodes in the lateral neck (levels II–V), level VII (anterior mediastinum), and rarely in level I may be involved by thyroid cancer. For those patients in whom nodal disease is evident clinically on preoperative ultrasound and nodal fine-needle aspiration or thyroglobulin measurement, or at the time of surgery, surgical resection may reduce the risk of recurrence and possibly mortality. Functional compartmental en-bloc neck dissection is favored over isolated lymphadenectomy (“berry picking”) with limited data suggesting improved mortality (6).
What may be less clear is which levels of the neck should be included in the lateral neck dissection. Recent literature has advocated for the routine removal of levels II, III, IV, and VB when there is evidence of nodal disease in the lateral neck. A schematic right anterior oblique view indicating levels of the neck and upper mediastinum relevant to neck dissection are summarized in Table 1 (Fig. 2). Lateral neck dissection can be safely accomplished through a low collar extension of the thyroidectomy incision that is cosmetically more acceptable than perpendicular incisions extending upward to the mastoid tip (24,25).
SCM, sternocleidomastoid.
Tailoring Reoperative Surgery for Persistent/Recurrent PTC
Regardless of the initial treatment paradigm utilized for PTC, some patients will manifest persistent or recurrent disease. Considerations for management of this disease must come from an understanding of its biological behavior. Much of the persistent/recurrent disease today is detected subclinically via surveillance strategies advocated by the ATA guidelines (6,17). Ironically, despite these improvements in surveillance, NCI (SEER database) data demonstrate that in the last 30 years or more, the survival rate for PTC has remained relatively the same. High-resolution ultrasonography and serum thyroglobulin assays with or without thyrotropin stimulation have led to a new category of patients with persistent/recurrent small volume disease of uncertain clinical significance. Many authors have demonstrated that reoperative surgery for this disease, especially in the central compartment, is safe. Efficacy of this surgery depends on what end point is being evaluated (26 –28).
Guidelines for the management of the patient with recurrent/persistent nodal disease are in order. Definitions of microscopic and macroscopic nodal recurrences should help to define which groups of patients could be observed versus those that should be offered surgery. Reasonable and realistic expectations should be set for the practitioners and patients involved. When possible, compartmental dissection of the neck nodal region involved should be performed to reduce the risk of loco-regional recurrence and the morbidity of further reoperation. Many of these patients with persistent disease have undergone multiple surgeries in the central or lateral compartments. Further attempts at formal compartmental dissection must be met with a careful weighing of the risks and benefits to the patient. Perhaps the realistic goal of all reoperative surgery should not be to render the serum thyroglobulin level undetectable but rather to prevent local disease progression in critical areas of the neck. Long-term follow-up of these patients is warranted to determine the optimal surveillance and treatment paradigm.
The preceding controversies could all be rendered moot if we had a way to predict the biological behavior of PTC. The ability to test a fine-needle aspiration biopsy specimen demonstrating PTC for a molecular marker profile that could accurately stratify risk and prognosis would be ideal. This model is becoming more realistic each passing day. Pioneers in this area like Nikiforov et al. and Xing et al. have demonstrated that the BRAF mutation in PTC predicts a poorer prognosis and that a test for the BRAF mutation can be done before any treatment intervention to optimize surgical treatment. This critical data could potentially help to determine which patients with PTC should have elective CND. It also may help to select patients with small PTCs who are able to safely undergo minimally invasive surgery as well. These hypotheses must now be studied prospectively (29,30).
Minimally Invasive Thyroid Surgery, Transaxillary Robotic Surgery, and PTC: Is There a Role?
After nearly a century of performing thyroid surgery essentially the way it was described by Dr. Theodor Kocher, the technique has rapidly evolved in the last few years. Thyroid surgery is one of the newest fields for the application of minimally invasive techniques. It can now be accomplished endoscopically or with robotic assistance in many patients who therefore may benefit from these alternative approaches. The development of thyroid surgery through smaller cervical scars and the axilla may be a step toward better cosmetic outcomes. Minimally invasive approaches were developed to improve cosmetic results, minimize postoperative pain, and potentially reduce the length of the hospital stay. These approaches are a safe and feasible alternative to open thyroid surgery while avoiding the need for a standard cervical collar incision. An improved understanding of the procedures and the appropriate indications for their application will continue to evolve as new technologies emerge.
The most commonly used approach today is the transcervical minimally invasive video-assisted thyroidectomy (MIVAT) technique developed by Miccoli et al. in 2001 (31).
This approach is currently used for both partial and total thyroidectomy. MIVAT is most commonly used for small thyroid nodules. MIVAT is a safe and feasible alternative to open thyroid surgery in appropriately selected cases. A nodule measuring 3.0 cm or less is ideal for this approach. As MIVAT continues to evolve, the indications for the procedure also evolve.
Nodule diameter above 3 cm, malignant nodules, history of thyroiditis, and Graves disease are currently relative contraindications. Some groups have reported that MIVAT can be safely used in patients with the above-mentioned criteria (32 –34).
The indications for this procedure have also expanded to include low- and intermediate-risk PTC (35). Indications and relative contraindications to MIVAT are summarized in Table 2. Long-term follow-up is warranted to assess oncologic efficacy.
MIVAT, minimally invasive video-assisted thyroid surgery.
Robot-Assisted Gasless Transaxillary Thyroidectomy
The use of wristed instruments and the elimination of operator tremor have significantly expanded the applications of the robotic approach to head and neck surgery. Robot-assisted transaxillary thyroidectomy is feasible with proper instrumentation and an experience with robotic surgery. This approach was originally developed in South Korea by Dr. Woong Chung at Yonsei University College of Medicine in Seoul. He reported his experience with 338 patients who underwent robot-assisted endoscopic thyroid operations using a gasless, transaxillary approach (36).
When compared to MIVAT, utilizing the robot in an indirect endoscopic approach provides a significantly broader view of the thyroid bed. The wrist movements of the robot instrumentation provide a greater degree of movement than the use of straight endoscopic instruments, while eliminating operator tremor.
Contraindications to this new approach include enlarged thyroids with Graves disease and advanced thyroid cancer.
Until there is longer-term follow-up for these patients, there must be cautious enthusiasm for the universal adoption and acceptance of these techniques in PTC. We bear an obligation to our patients and society to cautiously and ethically study the implementation of this new technology, especially for the treatment of PTC.
When treating a patient with PTC, it seems prudent to weigh all of these factors discussed in this review to individualize the most optimal surgical plan.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.
Portions of this review were presented at the Spring 2010 Meeting of the American Thyroid Association, “Thyroid Disorders in the Era of Personalized Medicine,” Minneapolis, Minnesota, May 13–16, 2010.