
Abstract
Background:
Many studies have shown an association between thyroid disorders and breast cancer. Among them, diffusely increased thyroid uptake of F18-fluorodeoxyglucose (F-18 FDG) has been associated with chronic lymphocytic thyroiditis. There is little or no information regarding the relationship between treatment of breast cancer and the development of new diffuse thyroid F-18 FDG uptake. Here, we report the frequency of this occurrence and some of the factors associated with it.
Methods:
We performed a retrospective review of the positron emission tomography (PET) computed tomography (CT) database and identified 290 women who had underwent PET-CTs both before and after breast surgery. Of these, 246 were enrolled in this study and 44 were excluded, because before breast surgery they had either a history of prior thyroid disorders including thyroid cancer or abnormal serum free thyroxine and thyroid-stimulating hormone, or other malignancies. Tests for serum antithyroid antibodies were not available before thyroid surgery in all patients. There were 62 patients who did have antithyroid antibody tests before surgery and 27 were positive. They were not excluded from the study.
Results:
Diffuse thyroidal uptake on PET-CT developed in 23 (9.3%) patients during the follow-up period (median=21.1 months; range=3.1–47.3 months). Age (≥55 years; hazard ratio [HR]=0.15; 95% confidence interval [CI]: 0.03–0.65; p=0.012), bilaterality of breast cancer (HR=3.87; 95% CI: 1.02–14.62; p=0.046), and postsurgical radiotherapy (HR=3.06; 95% CI: 1.03–9.16; p=0.045) showed independent association with new thyroid FDG uptake in multivariate analysis. All patients with thyroid FDG uptake met at least one of some criteria related to chronic thyroditis (positive for antithyroid antibodies or cytology findings or ultrasonography findings of Hashimoto's thyroiditis) and were associated with development of hypothyroidism (52.2% vs. 4.5% in patients without uptake; p<0.001).
Conclusions:
Radiotherapy in breast cancer may be an independent predictive factor for the development of new diffuse thyroidal uptake in PET-CT associated with thyroid dysfunction during follow-up. The development of diffuse F-18 FDG uptake is a marker for thyroid abnormalities. Younger women who have radiotherapy after surgery for breast cancer, in particular, are candidates for close follow-up of their thyroid function.
Introduction
F18-fluorodeoxyglucose (F-18 FDG) positron emission tomography computed tomography (PET-CT) is an important imaging modality for detecting recurrences and monitoring treatment outcome in breast cancer (4). Incidental thyroid uptake in F-18 FDG PET-CT is often encountered in daily practice (5). Diffuse FDG uptake in the thyroid has been reported in about 0.6%–3.3% of healthy subjects and patients with incidental thyroid cancer on PET-CT (6 –8). Patients with breast cancer have a relatively high prevalence of this condition (9), perhaps because they have a high prevalence of thyroid disorders (10,11). The incidental finding of diffusely increased F-18 FDG uptake in the thyroid gland is primarily associated with chronic lymphocytic thyroiditis, with or without the presence of hypothyroidism (7,12); some investigators consider such an uptake as normal variant (13,14).
There are a number of studies regarding the prevalence and clinical implications of diffuse FDG uptake in the thyroids of breast cancer patients (9,15). However, there was no previous report on what are the predisposing factors of the diffuse thyroid uptake in F-18 FDG after treatment of breast cancer. The present study was conducted to evaluate predictive factors for the development of new diffuse thyroid uptake in F-18 FDG after treatment of breast cancer patients who had no prior thyroid disorders.
Subjects and Methods
Patients
Between January 2006 and September 2009, 979 patients underwent breast surgery for primary breast cancer at Pusan National University Hospital. A retrospective review of the PET-CT database revealed that 290 female patients underwent PET-CT both before and after breast surgery. All patients had thyroid function tests (free thyroxine [FT4] and thyroid-stimulating hormone [TSH]) before surgery. Of these 290 patients, 247 were enrolled in this study at baseline, and 43 were excluded because of the following reasons: diffuse or focal uptakes on preoperative PET-CT (n=28); history of thyroid disorders (n=10); preoperative thyroid hormone abnormalities (TSH, <0.3 or >5.0 mIU/L; or FT4 <0.8 or >2.1 ng/dL; n=6); preoperative positivity for thyroid antibodies (antithyroid peroxidase [TPO] antibody or antithyroglobulin [Tg]; n=27); concurrent thyroid malignancy (n=6); and other concurrent malignancy (n=1). One patient had focal thyroidal uptake and was diagnosed with thyroid metastasis of breast cancer during the follow-up period, so 246 patients were included in this study.
All patients had thyroid function tests (FT4 and TSH) during follow-up period after surgery. If patients with breast cancer had an abnormality in their thyroid function tests (TSH, <0.3 or >5.0 mIU/L; or FT4, <0.8 or >2.1 ng/dL) or FDG PEC-CT imaging, it was the routine to refer them to the thyroid clinic and perform thyroid ultrasonography (US), thyroid autoantibodies test, and/or cytologic investigation. The US features of chronic thyroiditis include fibrous, enlarged, and lobulated glands with ill-defined hypoechoic heterogeneous areas or micronodulation (16). Hypothyroidism (over or subclinical) was defined as a TSH level greater than 5.0 mIU/L. As previously noted, those patients with abnormal thyroid function tests were not included in this study. Among the patients who were included in the present study, there were 54 that had thyroid US, 78 that had tests for anti-TPO antibodies, 64 that had tests for anti-Tg antibodies, and 27 that had biopsy of thyroid gland for cytology during follow-up. The thyroid dysfunctions related to chronic thyroiditis were defined by the following criteria: (i) positive for anti-TPO antibody or anti-Tg antibody, (ii) cytologic confirmation of Hashimoto's thyroiditis, and (iii) the US findings of chronic thyroiditis.
Immunohistochemical analyses for the estrogen receptor (ER), progesterone receptor (PR), and c-erb-B2 (proto-oncogene) were performed using specific monoclonal antibodies. Hormone therapy consisted of an ER antagonist or an aromatase inhibitor. Chemotherapy and radiotherapy were used to treat patients with widespread or life-threatening disease and ER-negative patients.
This study was approved by the Institutional Review Board of Pusan National University Hospital, and all subjects gave their informed consent to participate in the study.
F-18 FDG PET-CT imaging analysis
F-18 FDG PET-CT images were obtained with a dedicated PET-CT scanner (Gemini; Philips, Milpitas, CA) consisting of a dedicated germanium oxyorthosilicate full-ring PET scanner and a dual slice helical CT scanner. Standard patient preparation included at least 8-hour fasting and a serum glucose level of <120 mg/dL before F-18 FDG administration. PET-CT imaging was performed 60 minutes after injection of F-18 FDG (mean dose, 383.7±47.4 MBq; range, 314.5–488.4 MBq). Sixty minutes after administration of F-18 FDG, low-dose CT (30 mAs, 120 kV) covering the area from the base of the skull to the proximal thighs was performed for the purpose of attenuation correction and precise anatomical localization. Thereafter, emission scan was conducted in a three-dimensional mode. Emission scan time per bed position was 3 minutes; nine bed positions were acquired. PET data were obtained using a high-resolution whole-body scanner with an axial field of view of 18 cm. The average axial resolution varied between 4.2 mm full width at half maximum in the center and 5.6 mm at 10 cm. The average total PET/CT examination time was 30 minutes. After scatter and decay correction, PET data were reconstructed iteratively with attenuation correction and reoriented in axial, sagittal, and coronal slices. The row action maximum-likelihood algorithm was used for three-dimensional reconstruction.
F-18 FDG PET-CT images were reviewed by two experienced nuclear physicians on a workstation (Extended Brilliance Workstation; Philips Medical Systems, Miltipas, CA) as maximum intensity projection and coronal, sagittal, and axial images visually and quantitatively. Findings were recorded by consensus. A third reviewer was assigned to resolve differences in visual interpretation. The nuclear physicians were blinded to all other clinical imaging information. In F-18 FDG PET-CT images, thyroid uptake was considered to be present when there was increased uptake in the thyroid gland above physiologic background (less or above the liver uptake). Diffuse thyroid uptake is defined as uniform distribution of tracer above background throughout both lobes. To calculate maximal standardized uptake values (SUVmax), manually defined regions of interest were drawn over both lobes, with the higher of the two values between the lobes used in the analyses.
Statistical analysis
Statistical analyses were performed with SPSS version 15.0 (SPSS, Chicago, IL). Continuous data are expressed as median and range throughout the article. The Mann–Whitney test was used to compare continuous variables between subgroups. Categorical variables were compared using the χ 2 test. The Kaplan–Meier method with the log-rank test was used to compare new thyroid uptake rates in univariate analyses. Variables with p<0.2 on univariate analyses were included in multivariate analysis.
A Cox proportional hazard model and the forward stepwise method were used to analyze various prognostic factors for new thyroid FDG uptake in multivariate analyses. The relative importance of prognostic factors was presented as hazard ratio (HR) and 95% confidence intervals (95% CIs), which were calculated using binomial disturbance. Also, linear correlations were assessed between radiation dosage and other parameters. p-values were two-sided throughout, and a p-value of <0.05 was considered statistically significant.
Results
Baseline patient characteristics
Unilateral tumor accounted for 95.9% of all breast malignancies (n=236). Breast cancer was classified according to the tumor, node, metastasis (TNM) classification. There were 18 patients with stage 0 (7.3%), 78 with stage I (31.7%), 98 with stage II (39.8%), 43 with stage III (17.5%), and 9 with stage IV (3.7%). The median follow-up period was 21.1 months (range, 3.1–47.3 months). The median age was 51.0 (range, 24–85 years). Of the 246 patients, 23 (9.3%) showed new diffuse thyroid uptake on PET-CT during the follow-up period.
Table 1 summarizes the baseline (preoperative and postoperative) characteristics of patients with and without new diffuse thyroid FDG uptake on follow-up PET-CT after treatment. Patients with thyroid FDG uptake were younger than those without (p=0.011). There were no differences between the two groups in BMI, preoperative TSH, stage, ER positivity, PR positivity, and C-erb-B2 positivity at baseline. With regard to treatment, there were no differences between the two groups in chemotherapy and hormonal therapy (p=0.917 and p=0.257, respectively). However, patients with thyroid FDG uptake underwent radiotherapy more frequently than those who did not have this treatment (82.6% vs. 49.8%; p=0.003).
Data are expressed as median (range) for continuous variables and as frequency (%) for categorical variables.
TSH, thyroid-stimulating hormone; ER, estrogen receptor; PR, progesterone receptor; T4, thyroxine.
Association of new thyroid FDG uptake with various clinical parameters
Age and bilateral, as opposed to unilateral, breast cancer were significantly associated with thyroid FDG uptake in univariate analysis (p=0.005 and p=0.038, respectively; Table 2 and Fig. 1). Of the 130 patients who received radiotherapy, 19 (14.6%) had thyroid FDG uptake during a follow-up of 21 months, whereas 4 (3.5%) who did not receive radiotherapy had this uptake (log-rank statistics=3.06, p=0.012; Fig. 2). Age (≥55 years; HR=0.15; 95% CI: 0.03–0.65; p=0.012), bilateral nature of breast cancer (HR=3.87; 95% CI: 1.02–14.62; p=0.046), and postsurgery radiotherapy (HR=3.06; 95% CI: 1.03–9.16; p=0.045) showed independent associations with new thyroid FDG uptake in multivariate analysis (Table 2).
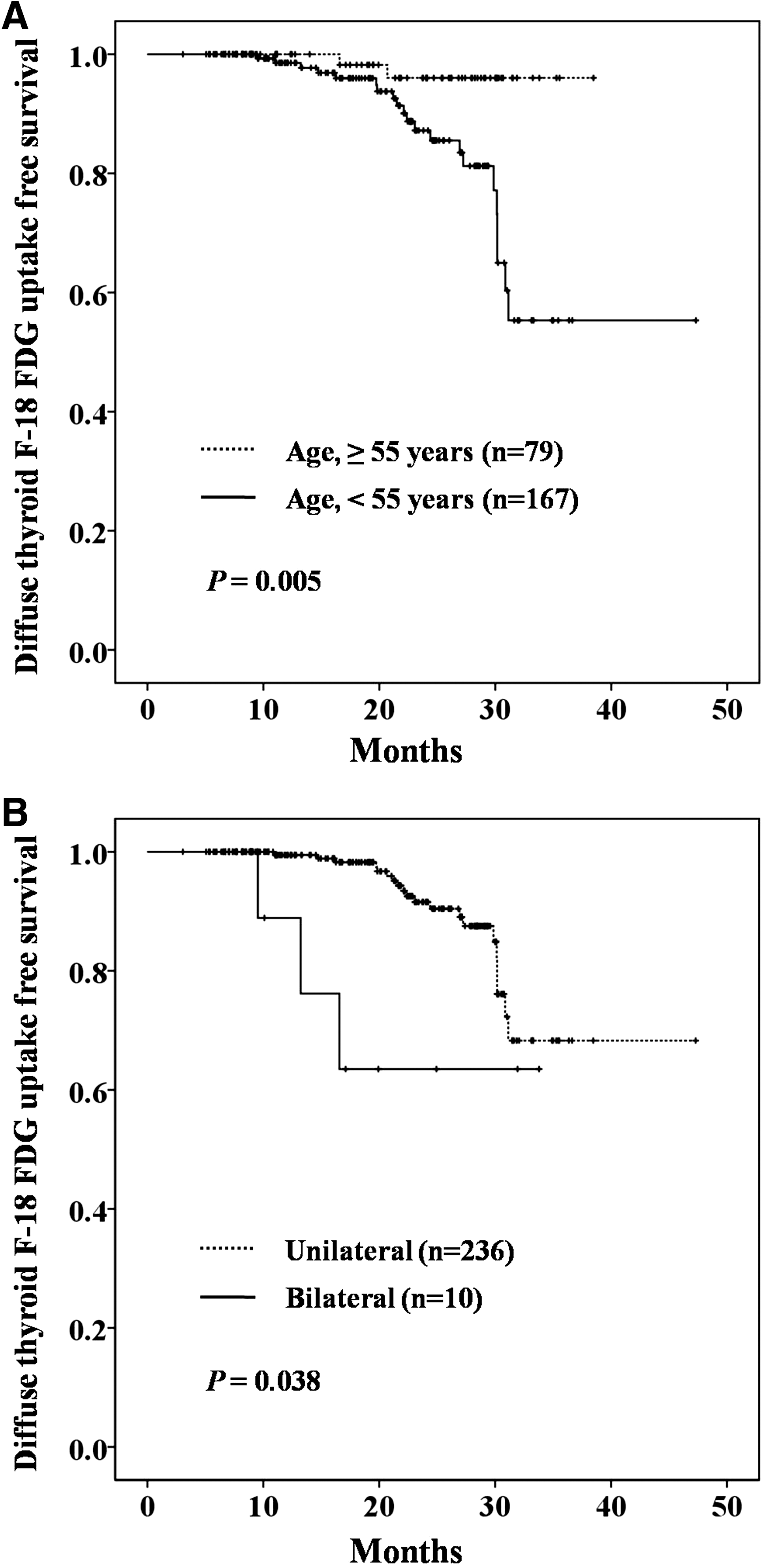
Kaplan–Meier estimate of diffuse thyroid F-18 FDG-free survival according to age group
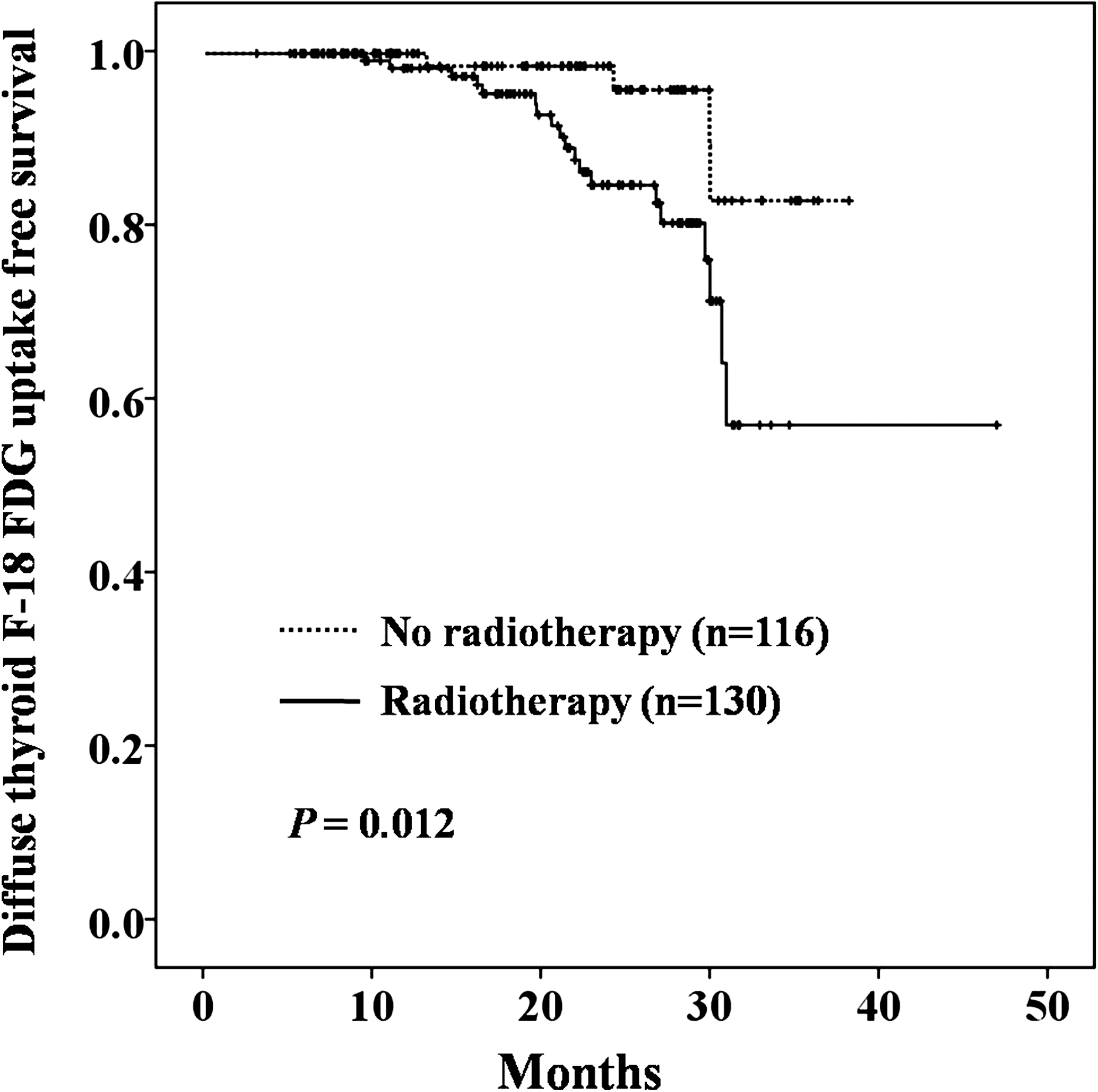
Kaplan–Meier estimate of diffuse thyroid F-18 FDG-free survival according to radiotherapy.
HR, hazard ratio; CI, confidence interval.
Thyroid abnormalities in patients with new thyroid FDG uptake
New diffuse uptake developed in both thyroid lobes in 18 patients, whereas diffuse uptake was observed in one thyroid lobe in 5 patients. The median SUVmax of patients with thyroid FDG uptake was 3.2 (range, 2.0–9.0). All patients with thyroid FDG uptake had more than one of the thyroid abnormalities characteristic of chronic thyroiditis based on tests performed after the second FDG uptake. There were 18 patients who tested positive for TPO or Tg antibodies. There were five patients who had cytology findings of Hashimoto's thyroiditis. There were 19 patients who had US findings of Hashimoto's thyroiditis. In addition, patients with the new thyroid FDG uptake had a higher level of serum TSH than those without thyroid FDG uptake (4.50 vs. 1.91 mIU/L; p<0.001). Of the 23 patients with new thyroid FDG uptake, 12 patients (52.2%) developed hypothyroidism during the follow-up period (vs. 4.5% in patients without uptake; p<0.001). L-T4 was prescribed for hypothyroidism during their follow-up period in six patients in the group that had new thyroid FDG uptake. L-T4 was prescribed in four patients in the group that did not have new thyroid FDG uptake.
Association between the abnormality of thyroid and radiotherapy
During the follow-up period, patients who received radiotherapy had higher serum TSH concentrations than those who did not receive radiotherapy (2.14 vs. 1.54 mIU/L; p=002). Patients with new thyroid FDG uptake received higher radiation doses than those without this (56.3 vs. 32.4 Gy; p=0.003). The Pearson correlation test between radiation dosage and SUVmax showed no significant correlation. There was significant correlation between radiation dosage and TSH level during the follow-up period (r=0.182; p=0.006). However, the radiation dosage did not significantly correlate with the levels of FT4, anti-TPO, and anti-Tg during the follow-up period.
Discussion
This study found that young age, bilateral primary breast cancer, and radiotherapy are each independently associated with the development of diffuse thyroid FDG uptake after treatment of breast cancer patients who had no history of thyroid disorders or evidence for overt or subclinical hypothyroidism. Some of the patients with new thyroid FDG uptake, however, did develop abnormal thyroid function tests after their second FDG study and, notably, following radiation therapy. Importantly, the radiation doses were higher in patients with new thyroid FDG uptake.
In the present study, the prevalence of new thyroid FDG uptake was 12.6% in women <54 years of age (n=167) and 2.5% in women >55 years of age (n=79; p=0.012). It is considered that younger women are more susceptible to the development of thyroid FDG uptake in the present study. The preponderance of young women with autoimmune thyroid disorders may correlate with high estrogen levels, which is implicated as an enhancer of humoral immunity (17).
Various causes of diffuse FDG uptake in the thyroid gland have been reported. F-18 FDG accumulation in normal thyroid tissue is usually low to absent, because free fatty acids are preferred substrates for the thyroid gland (18). Diffuse thyroid uptake is generally regarded as benign, and it results from inflammatory etiologies, such as thyroiditis (19,20). Activated lymphocytes are considered to show enhanced glucose metabolism in chronic thyroiditis (21). Also, fibroblast infiltration results in continuous FDG uptake after treatment in patients with chronic thyroditis (7). Tateishi et al. (9) evaluated the clinical implications of diffuse FDG uptake in the thyroid glands in advanced breast carcinoma by comparing metabolic and morphologic patterns on PET-CT. Twenty percent of patients with advanced breast carcinoma showed diffuse thyroid uptake on the baseline PET-CT scan in that study. Of the patients with diffuse thyroid uptake, 72% patients who received thyroid hormone replacement therapy showed no significant changes in the volume, SUVmax, and total lesion glycolysis (TLG) of the thyroid glands on the follow-up PET-CT scan. In contrast, patients without thyroid hormone replacement therapy showed marked decreases in SUVmax and TLG. They suggested that diffuse thyroid uptake in patients with advanced breast cancer represents active inflammation caused by chronic thyroiditis (9). Patients with prior thyroid FDG uptake before treatment were excluded in our study, unlike evaluating the patients with diffuse thyroid uptake before treatment in the study by Tateishi et al. Despite this fact, all patients with new diffuse thyroid uptake in our study also had evidence for chronic thyroiditis based on autoantibodies, US, and cytological confirmation.
A strong relationship between breast cancer and thyroid autoimmunity has been found in breast cancer patients after mastectomy but before beginning any chemohormonal adjuvant therapy (22). This is particularly important, because the autoimmune system can be influenced by surgery, triggering or worsening autoimmune diseases. However, this relationship was also present before surgery (2). Radiotherapy can lead to thyroid dysfunction either by direct parenchymal damage or by vascular compromise through fibrosis (23). Although the relationship between irradiation and thyroid autoimmunity remains controversial, irradiation can trigger or exacerbate thyroid autoimmunity with clinical or experimental evidence (24,25). Development of thyroid dysfunction after radiotherapy for cancer of the head and neck has been already reported (23,26,27). Also, primary hypothyroidism and autoimmune thyroiditis are more frequently observed after radiotherapy in breast cancer patients (28 –30). In the present study, radiotherapy was also an independent predictive factor for diffuse thyroid FDG uptake associated with thyroid dysfunction. In addition, the radiation doses significantly correlated with the serum TSH level during the follow-up period after radiotherapy, although it did not correlate with autoantibodies.
Several studies have indicated that the autoimmune system can be influenced by surgery or chemotherapy, triggering or worsening autoimmune thyroid disease (2,31). According to other studies, treatment with ER antagonists, such as tamoxifen, is accompanied by an increase in total serum levels of T4 and T3 (32). In the present study, we did not find any significant influence of tamoxifen therapy and chemotherapy on the development of new diffuse thyroid FDG uptake.
Patients with previous thyroid disorders or FDG uptakes before treatment were not excluded in most previous studies dealing with FDG uptake in the thyroid gland in cancer patients (9,15). In contrast, we only included patients with breast cancer without previous thyroid disorders, and thus it was possible to evaluate the risk factors associated with diffuse thyroid FDG uptake and thyroid dysfunction in breast cancer patients after treatment.
This study has several limitations. First, it was retrospective. Second, we could not entirely evaluate the relationship between new thyroid FDG uptake and thyroid autoimmunity, because we did not study a group of subjects who did and did not have breast cancer and who did and did not have treatments for breast cancer and we did not have thyroid antibody tests or other tests for thyroid autoimmunity before the first FDG uptake in all patients. Although all patients had thyroid function test after second FDG study, all the patients who did not have abnormality in thyroid function test or FDG PET-CT imaging did not have thyroid antibody tests during their follow-up.
To the best of our knowledge, there has not been a previous study to evaluate the development of diffuse thyroid FDG uptake in breast cancer patients with no thyroid FDG uptake before treatment, including radiation. In conclusion, the results of the present study confirm the association between radiotherapy for breast cancer and development of diffuse thyroid FDG uptake. Our results call attention to the usefulness of examination for thyroid disorders during follow-up in young breast cancer patients who received radiotherapy.
Footnotes
Disclosure Statement
The authors of the present study declare that no conflicts of interest exist.