
Abstract
Background:
The BRAF V600E mutation has been reported in 50%–80% of papillary thyroid carcinoma (PTC) cases and is highly specific for PTC. Reflex BRAF testing may improve the diagnostic accuracy of thyroid fine-needle aspiration (FNA) tests having equivocal cytologic interpretations and provide prognostic information that helps guide management in patients with PTC.
Patients and Methods:
Cases with equivocal thyroid FNA readings (indeterminate and suspicious for PTC) or a positive diagnosis for PTC and concomitant BRAF mutation analysis were included in this prospective study. BRAF mutation analysis was performed by polymerase chain reaction combined with single-strand conformation polymorphism gel electrophoresis using lavage fluid obtained from needle rinsing. The results of histopathologic follow-up were correlated with the cytologic interpretations and BRAF status.
Results:
One hundred fifty-seven FNAs with equivocal or positive cytologic interpretations were eligible for the study. All but one (99.4%) FNAs were found to have sufficient DNA quality and quantity for the assay. Based on the follow-up diagnosis of nodules after surgical resection, the sensitivity for diagnosing PTC was 63.3% with cytology alone and 80.0% with the combination of cytology and BRAF testing, respectively. No false positives were noted with either cytology or BRAF mutation analysis. All PTCs with extrathyroidal extension and of tall-cell variant were postive for BRAF mutation.
Conclusions:
BRAF V600E mutation analysis can be easily performed on cytologic preparation using lavage fluids obtained from needle rinsing. By combining morphologic evaluation and BRAF testing, there is a substantial improvement in the preoperative identification of PTC when compared with cytology alone. Patients with equivocal cytologic diagnosis and BRAF V600E mutation are candidates for total thyroidectomy ± central lymph node dissection.
Introduction
Although it has been reported in tumors of other organs (11), BRAF mutation involving V600E is highly specific for PTC among other primary thyroid neoplasms and has not been observed in benign thyroid lesions (12 –14). In addition, the presence of BRAF mutation has been associated with aggressive tumor characteristics, such as extrathyroidal extension, lymph node involvement, resistance to radioactive iodide, and tumor recurrence (15 –17). Therefore, the detection of BRAF V600E mutation, using fine-needle aspiration (FNA) biopsy material, would not only assist preoperative diagnosis of PTC but also provide prognostic implications to guide subsequent patient management (18).
In September 2009, our laboratory began to offer reflex BRAF testing on thyroid FNAs that had an equivocal diagnosis, that is, atypia of undetermined significance or suspicious for PTC, as well as thyroid FNAs that were interpreted as positive for PTC. In this prospective study, our objective was to evaluate the utility of reflex BRAF testing for equivocal and positive thyroid FNA readings.
Materials and Methods
Study population
Thyroid FNA cases between September 2009 and November 2010 with a diagnosis of indeterminate, that is, follicular cells of undetermined significance, suspicious for PTC, or positive for PTC and BRAF mutation analysis between September 2009 and November 2010 were included in this prospective study. The study was approved by the institutional review board. All FNAs were performed under ultrasound guidance by either endocrinologists or radiologists. Direct smears were prepared from each pass and were either air dried and stained with Diff Quik stain (Dade Behring) or fixed in alcohol and stained by the Papanicolaou method. The needle was then rinsed in Cytorich Red solution (Thermo-Fisher Scientific) for ThinPrep (Hologic) preparation and subsequent molecular analysis. On average, two to three passes were performed for each nodule. No onsite assessment of adequacy was performed. Histologic diagnoses were used as the gold standard for correlation with the cytologic interpretations and BRAF mutation status.
Cytologic diagnostic terminology and interpretation
At our institution, thyroid FNAs were classified using the six-tier Bethesda classification for thyroid FNA (17). The category “Follicular cells of undetermined significance” was reserved for aspirates with findings that were not convincingly benign but not diagnostic of a neoplastic or malignant process. These cases were often characterized by borderline cellularity. Some of the cases demonstrated a predominant microfollicular pattern and no or minimal colloid, that is, an architectural pattern eliciting concern for a follicular neoplasm. Others demonstrated nuclear atypia such as the presence of occasional nuclear grooves, abnormal chromatin pattern, or nuclear overlapping and crowding, that is, anomalous findings within individual cells eliciting concern for a papillary carcinoma.
The category “Suspicious for malignancy” applied to specimens that demonstrated features of a PTC but were quantitatively or qualitatively insufficient to make a definitive diagnosis of malignancy. These features included, but were not limited to, an occasional intranuclear inclusion, cytoplasmic grooves, or psammoma calcifications (calcospherites). The category “Positive for malignancy” applied to cellular specimens with unequivocal cytologic evidence of a malignant neoplasm.
The cytologic diagnoses were rendered by seven board-certified cytopathologists; their experience ranged from 2 to 10+ years. All cases were reviewed in the daily consensus conference among the cytopathologists to minimize interobserver variability.
BRAF mutational analysis
BRAF testing was performed reflexively when the cytologic diagnosis was indeterminate (equivalent to “Follicular cells of undetermined significance”), suspicious for PTC, or positive for PTC. For patients with two nodules, BRAF testing would be performed for both nodules if their diagnoses fell into one of the aforementioned three categories.
DNA was extracted using the Qiagen tissue kit (Qiagen) following the manufacturer's instructions. The amount of recovered DNA was quantified by reading at 260 nm using a spectrophotometer. A total of 5–20 ng of DNA was amplified using 0.2 μM polymerase chain reaction (PCR) primers flanking the region of V600E mutation of BRAF (5′ flank primer: CTCTTCATAATGCTTGCTCTGATAGG and 3′ flank primer: TAGTAACTCAGCAGCATCTCAGG) in a 50 μL PCR mixture containing 1 × PCR buffer, 0.1 mM dNTP, 1.5 mM MgCl2, and 2.5 units of AmpliTaq Gold DNA polymerase. PCR was started at 95°C for 8 minutes, followed by 35 cycles of 94°C for 1 minute, 55°C for 1 minute, and 72°C for 2 minutes, and finished at 72°C for 10 minutes. The PCR yielded a 250-base pair product. Single-strand conformational polymorphism (SSCP) analysis was carried out using 4 μL of PCR product on mutation detection enhancement nondenaturing gel. Electrophoresis was carried out on ice for 2 hours and 45 minutes at 325 V. The SSCP gel was then stained with SYBR Gold (Molecular Probes) 1:10,000 in TE for 20 minutes. The gel was imaged using Biorad GelDoc UV System (BioRad). The presence or absence of BRAF V600E mutation was identified by comparing the SSCP banding pattern of the case with that of a positive control.
Statistical analysis
The sensitivity and specificity of BRAF as a marker for PTC for patients with an equivocal cytologic diagnosis were estimated. In addition, we also calculated the sensitivity and specificity in diagnosing PTC with cytology alone and combining cytology and BRAF testing. FNAs with a positive cytologic diagnosis, BRAF V600E mutation, or both were considered positive preoperative diagnosis of PTC for calculation. Only cases with histologic follow-up were included in the calculation. Chi-square and Fisher exact tests were used to evaluate frequency differences. Two-tailed t-test was used to evaluate differences in age and tumor size of PTCs between specimens with and without BRAF V600E mutation. A p-value of 0.05 or less was considered to indicate a statistically significant difference. Statistical analyses were performed with SPSS software (SPSS).
Results
Altogether, 157 FNAs with equivocal or positive cytologic interpretations were eligible for the study. They were obtained from 147 patients; 108 (73.5%) female patients and 39 (26.5%) male patients, with a mean age of 52.6 ± 15.6 years (range: 12–87 years). Ten patients had two nodules sampled by FNA. Twenty-four (11.6%) FNAs were from isthmus, 48 (30.6%) from left lobes, and 78 (49.7%) from right lobes. For the remaining nine, one FNA was performed on thyroid bed and nine were performed on cervical lymph nodes in patients with a history of PTC. Eighty (51.0%) FNAs had an indeterminate cytologic interpretation, 20 (12.7%) suspicious for PTC, and 57 (36.3%) positive for PTC.
All but one (99.4%) FNAs were found to have sufficient DNA quality and quantity for the assay. Sixty-four (40.8%) FNAs were found to have BRAF V600E mutation, including 12 of 89 (13.5%) FNAs with an indeterminate diagnosis, 4 of 20 (20.0%) with a suspicious diagnosis, and 48 of 57 (84.2%) with a positive diagnosis. Table 1 summarizes the clinicopathologic features among cases with and without BRAF mutation. The percentage of FNAs with BRAF mutation was significantly higher in cases with a “positive” diagnosis than those with equivocal cases (p < 0.0001). However, there was no statistically significant difference in the proportion of cases with BRAF mutation between cases with “indeterminate” diagnosis and those with “suspicious diagnosis” (p > 0.05).
Ten patients had two nodules biopsied.
According to nodules.
The case with insufficient DNA was excluded. NS, not significant.
Tissue follow-up was available in 76 (52.4%) nodules; 72 nodules (94.7%) from 68 patients were resected, whereas 4 (5.3%) had repeat FNA. Follow-up information was not available for all nodules with positive cytologic diagnosis and/or BRAF mutation because the patients either were lost to follow-up or chose to be treated in another institution. Based on the status of BRAF mutation, 41.3% of nodules without BRAF mutation and 59.4% with BRAF mutation had a tissue follow-up; the difference was statistically significant (p < 0.026). Among the 68 patients with surgery, 60 had total thyroidectomy, including 38 with regional lymph node sampling, 6 lobectomy, and 2 with neck dissection only. Among the patients with total thyroidectomy, seven had initial lobectomy followed by intraoperative consultations and completion thyroidectomy. The indications for surgery for nodules with indeterminate cytologic diagnosis included family history of PTC, symptomatic goiter, hyperthyroidism, positive BRAF mutation, and contralateral cytologic diagnosis of PTC or follicular neoplasm.
For the four nodules with repeat FNA, all had an “indeterminate” cytologic diagnosis initially with absence of BRAF V600E mutation. Repeat FNA of three patients were negative, two were nodular goiter and the other was Hashimoto's thyroiditis. The remaining one was positive for PTC. For the 72 nodules with surgical intervention, 12 (16.7%) were found to be benign and 60 (83.3%) were found to be PTC. Table 2 summarizes the results of histologic follow-up of nodules with equivocal cytologic diagnosis. The sensitivity and specificity of BRAF as a marker for PTC in thyroid nodules with an equivocal cytologic diagnosis were 45.5% and 100%, respectively. All surgically resected nodules with a positive cytologic diagnosis were found to be PTC regardless of their BRAF status (Table 3). Overall, the sensitivity of diagnosing PTC was 63.3% and 80.0% with cytology alone and combined cytology and BRAF testing, respectively. The specificity was 100% in both instances.
Sensitivity: 45.5%; specificity: 100%.
Table 4 summarizes the pathologic features of PTCs. Almost two-thirds of the carcinomas demonstrated the V600E mutation. There were no statistically significant differences in terms of size and nodal status between carcinomas with and without BRAF mutation. The proportion of carcinomas with BRAF mutation was significantly higher in nonfollicular variants than the follicular variant.
Oncocytic variant.
Three tall-cell variants.
Discussion
In the United States, about 1 of 14 adults will present with a thyroid nodule (19,20). However, only 5% of the thyroid nodules are found to be malignant (19,21). As a result, FNA has been widely accepted as the diagnostic procedure of choice in the evaluation of patients presenting with nontoxic thyroid nodules (22,23). About 60%–70% of thyroid nodules are classified cytologically as benign, whereas 4%–10% of nodules are cytologically deemed malignant (24,25). The remaining 20%–30% present equivocal findings, which are not diagnostic of either benignancy or malignancy. Preoperative planning of optimal surgical management in patients with cytologic uncertainty is challenging. According to the new Bethesda System for the classification of thyroid FNA, cases that are classified as “atypia of undetermined significance” or “suspicious” have a risk of malignancy of 10%–15% and 60%–70%, respectively (26,27). The current guidelines recommend repeat FNA for patients with a diagnosis of “atypia of undetermined significance” and lobectomy with or without intraoperative consultation for those with a suspicious diagnosis (23). However, intraoperative analysis of frozen sections does not always provide definitive information (28). As a result, there may be significant management ramifications, ranging from delaying any necessary surgery to avoiding more definitive initial surgical treatment. To avoid delay in definitive surgical intervention or the additional costs and morbidity incurred for additional surgery, new approaches for improving the diagnostic accuracy of thyroid FNA are warranted.
Recent studies have demonstrated that over 80% of follicular cell–derived thyroid cancers have one of the common somatic genetic alterations, such as BRAF and RAS point mutations, RET/PTC rearrangements, etc. (2,3). The most prevalent genetic mutation is a point mutation in BRAF (V600E), which is observed in 50%–80% of PTC cases (4,5). The BRAF V600E point mutation has not been reported in any follicular carcinoma, adenoma, or benign thyroid nodule. Therefore, BRAF V600E point mutation appears to be a highly specific and fairly sensitive marker for the identification of PTC preoperatively.
In the present study, about 40% of all cases were found to have the BRAF V600E point mutation. Eighty-four percent and 17% of positive and equivocal (both indeterminate and suspicious) cases were found to have mutated BRAF, respectively. Other authors have reported the prevalence of BRAF mutation to be between 75% and 89% and between 15% and 39% for positive and equivocal FNAs, respectively (29 –31). Therefore, our results were comparable to those in the literature. We observed that the percentage of FNAs that were BRAF positive was significantly higher in positive cases than equivocal cases (p < 0.001). However, there was no significant difference in the frequencies of BRAF mutation between the two equivocal diagnostic categories. The relative low frequency of BRAF mutation in cases with a suspicious diagnosis may be due to the fact that over 50% of suspicious cases with follow-up were found to be follicular variant of PTC with a high RAS and very low BRAF mutation rates (32). It is not surprising that thyroid nodules with BRAF mutation were more likely to be resected than those without BRAF mutation.
Among the 60 histologically proven PTCs, the cytologic diagnosis was positive in 38 (63.3%) cases, suspicious in 9 (15.0%) cases, and indeterminate in 13 (21.7%) cases. BRAF mutation was detected in 40 of all 60 (66.7%) PTCs, including 30 of 38 (78.9%) positive FNAs, 2 of 9 (22.2%) suspicious FNAs, and 8 of 13 (61.5%) indeterminate FNAs. No false-positive cases were encountered for either FNA or BRAF testing. The combination of cytology and molecular analysis positively identified 48 (80.0%) PTCs, a 26% increase in the number of correctly identified PTC when compared with cytologic diagnosis alone. Other authors have also demonstrated that combining morphologic and molecular analyses improved preoperative identification of PTCs (30,31). For example, Marchetti et al. correctly identified 62% and 82% of PTCs by FNA alone and by combining FNA and BRAF testing, respectively (31). These results demonstrate the benefit of combining FNA and BRAF mutational analysis in improving the diagnostic accuracy of PTCs preoperatively.
Figure 1 illustrates the current management algorithm for patients with equivocal thyroid FNA, that is, indeterminate or suspicious for PTC, in our institution. Patients with nodules that have an equivocal cytologic diagnosis and are positive for BRAF mutation would be strong candidates for total thyroidectomy. This eliminates the need of a second surgery in 40% of patients with equivocal cytology in the present study. Lobectomy with or without intraoperative consultations would be indicated for patients with nodules that have a suspicious cytologic diagnosis but are negative for BRAF V600E mutation. Patients with nodules that have an indeterminate cytologic diagnosis and negative BRAF mutation may be followed up conservatively with repeated FNAs in 6–12 months if there are no other concomitant risk factors.
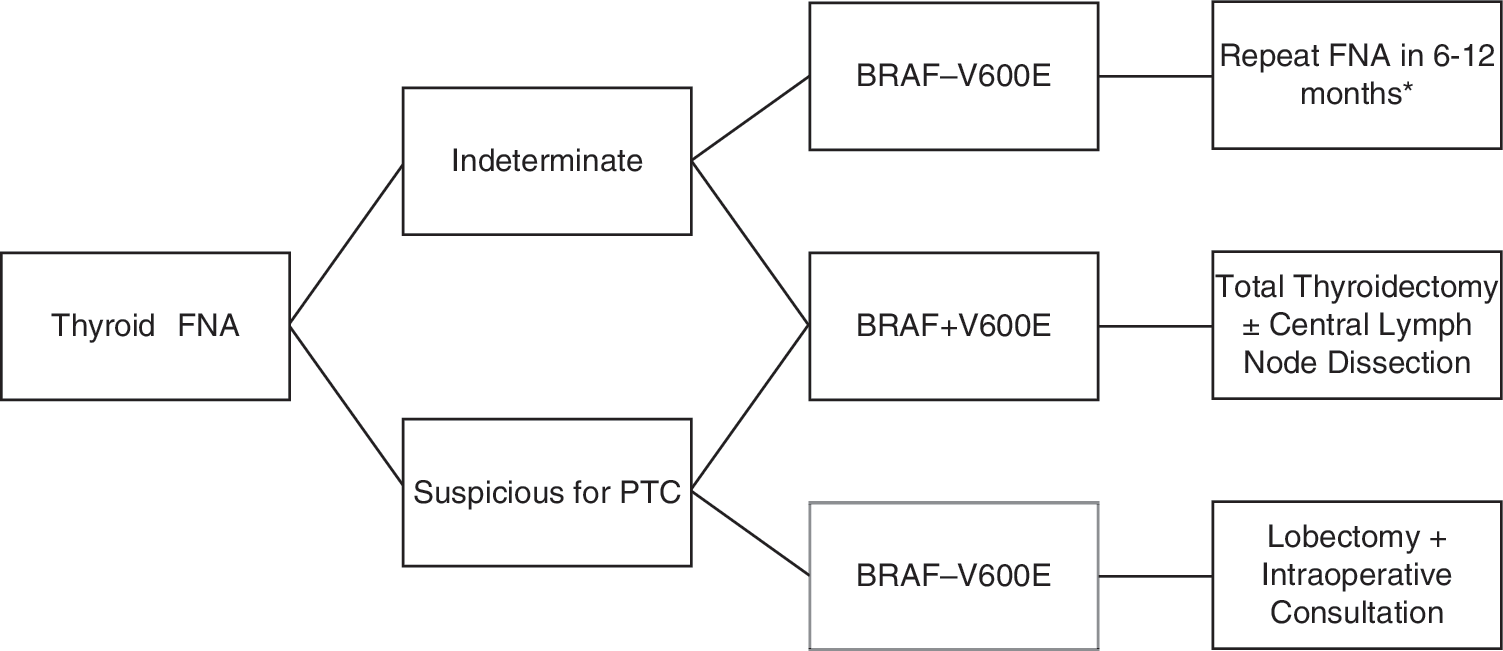
Management algorithm of patients with equivocal thyroid FNA. *Surgery may be indicated if there are other concomitant risk factors. PTC, papillary thyroid carcinoma; FNA, fine-needle aspiration.
Several studies have evaluated the use of cytologic preparations for molecular analysis (29,31,33 –37). Different approaches for obtaining cellular samples for molecular analysis were used in these studies, which included (i) scraping all cellular materials from the archival slides, (ii) microdissecting tumor cells from archival slides, (iii) using lavage fluid obtained from washing the needles after preparation of direct smears, and (iv) obtaining additional pass to be collected in preservative solution. The advantage of the first two approaches is the ability to select the slides containing optimal number of tumor cells for molecular analysis. However, it would require the destruction of diagnostic materials on the original slides, thus preventing future review. Further, it can be labor intensive when microdissection is required. The potential pitfall of using lavage fluid is that the sensitivity of the molecular analysis may be compromised because the quantity and composition of the cellular materials are unknown. In addition, there have been reports of discordance of BRAF mutation status between matched FNA and formalin-fixed, paraffin-embedded samples, that is, mutation was not detected in cytologic samples but was demonstrated in histologic samples (29,38).
In the present study, we employed the third approach. Only 1 of 157 (0.06%) FNAs was found to have inadequate DNA for molecular analysis. We did not evaluate the degree of concordance between matched FNA and formalin-fixed, paraffin-embedded samples. However, in another study using the same methodology, we have demonstrated that BRAF gene mutation can be detected from samples containing only 5% of PTC cells (39). Another additional advantage is that the lavage fluid can be stored in preservative solution in the laboratory for up to 3 weeks after collection, providing ample of time for subsequent molecular testing. Also, the original smears and slides would be preserved.
In addition to being a specific marker for PTC, BRAF mutation status also provides useful prognostic information that may help to refine patient management. It has been shown that the presence of BRAF mutation correlates with the presence of certain aggressive tumor characteristics including aggressive histologic subtypes, extrathyroidal extensions, nodal metastases, resistance to radioactive iodide, local recurrence, and shorter long-term survival (15 –17,40 –42). We observed that all tall-cell variants of PTCs as well as all PTCs with extrathyroidal extension demonstrated BRAF mutation. Tall-cell variants of PTCs are known to be locally more aggressive (43). However, there were no significant differences between PTCs with and without BRAF mutation in term of the tumor size, nodal status, and pathological stages. Plausible explanation is that the number of cases in the present cohort may be too small to demonstrate any statistical difference.
The strengths of the present study are prospective molecular analysis and the use of residual lavage fluid for BRAF mutational analysis. There are several limitations. First, a substantial number of cases, particularly cases with an indeterminate diagnosis, did not have a tissue follow-up. Second, we did not compare the BRAF status of the FNAs with their corresponding histologic specimens. As a result, we were not able to estimate the false-negative and false-positive rates of BRAF testing based on cytologic preparations. Lastly, the follow-up time was not long enough to allow the correlation of BRAF status with recurrent rate, response to radioactive iodide, and survival rate.
In conclusion, BRAF V600E mutation analysis can be easily preformed on cytologic preparation using lavage fluids obtained from needle rinsing. By combining morphologic evaluation and BRAF testing, there is a substantial improvement in the preoperative identification of PTC when compared with cytology alone, thus allowing better planning of surgical treatment.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.