
Abstract
Background:
The incidence of thyroid cancer (TC) has been increasing over the last 30 years in several countries, with some of the worldwide highest TC incidence rates (IRs) reported in Italy. The objectives of this study were to evaluate by histological subtypes the geographical heterogeneity of the incidence of TC in Italy and to analyze recent time trends for papillary thyroid carcinoma (PTC) in different cancer registries (CRs).
Methods:
The study included cases of TC (<85 years of age) reported to 25 Italian CRs between 1991 and 2005. Age-standardized IRs were computed for all histological subtypes of TC according to CRs. Estimated annual percent change and joinpoint regression analysis were used for analysis of PTC.
Results:
In women, IRs of PTC ranged between 3.5/100,000 in Latina and 8.5/100,000 in Sassari for the period 1991–1995 (a 2.4-fold difference) and between 7.3/100,000 in Alto Adige and 37.5/100,000 in Ferrara for 2001–2005 (a 5.1-fold difference). In men, IRs ranged between 0.7/100,000 in Latina and 3.4/100,000 in Sassari for the period 1991–1995 (a 4.9-fold difference) and between 2.0/100,000 (Alto Adige, Trento) and 10.6/100,000 in Ferrara for 2001–2005 (a 5.3-fold difference). In both sexes, IRs significantly higher than the pooled estimates emerged for the most recent period in the majority of CRs located within the Po River plain and in Latina, but they were lower in the Alpine belt. For women, CRs reported higher IRs than pool estimates showed, between 1991 to 2005, a significantly more marked annual percent change (+12%) than other CRs (+7%). For men the corresponding estimates were +11% and +8%.
Conclusions:
The distribution of PTC does not lend support to a role of environmental radiation exposure due to the Chernobyl fallout, iodine deficiency, or (volcanic) soils. Between 1991 and 2005, wide geographic variations in the incidence of PTC and heterogeneous upward trends emerged, suggesting that the heterogeneity was a relatively recent phenomenon; this appeared to be mainly explained by variations, at a local level, in medical surveillance.
Introduction
There has been little study of geographical heterogeneity (16,17) and trends in small areas (8,18 –20). Different explanations have been proposed for the variations in the incidence of TC relating to space and time, in particular, differences in medical surveillance (16,19) and ionizing radiation exposure (18,20). Inconsistent associations between incidence rates and iodine intake have been reported for PTC, by far the most common histological subtype (8,18). A link between some unknown exposure in volcanic areas and the incidence of TC has also been proposed (17).
The aim of the present study was to examine if there was geographical heterogeneity of the incidences of TC in Italy, according to histological subtypes, and to evaluate IR trends for PTC, by taking advantage of the fact that Italy has a large number of active cancer registries (CRs).
Materials and Methods
Cases of TC (International Classification of Diseases [ICD]-10 code C73) diagnosed between 1991 and 2005 in Italian areas where a CR is active were extracted from the anonymous cancer registry database of the Italian Association of Cancer Registries—AIRTUM (
As of June 2009, 25 CRs (18 million people, 32% of the total Italian population) had been active and had collected data on TC up to at least 2001 (Table 1). Sixteen of these registries (i.e., Alto Adige, Biella, Brescia, Ferrara, Friuli Venezia Giulia, Genoa, Milan, Modena, Parma, Reggio Emilia, Romagna, Sondrio, Trento, Turin, Varese, and Veneto) are located in northern Italy, three (i.e., Florence and Prato, Latina, and Umbria) in central Italy, and six (i.e., Naples, Ragusa, Salerno, Sassari, Siracusa, and Trapani) in southern Italy (2,21). CRs vary as far as the size of population they cover (180,000 to 2.1 million) and in number of years of they have been active (3–29 years). Routine indicators of data completeness and quality in Italian CRs are satisfactory (2,21).
Incidence rates are reported as truncated (0–84 years) rates per 100,000, age-standardized on Italian population 1991.
In the period covered by CRs, calculated only for CRs with >10 years of registration.
Impossible to calculate, because there are 0 cases for some years of registration.
Calculated on CRs with IRs available.
CIs, confidence intervals; CRs, cancer registries; EAPC, estimated annual percent change; IR, incidence rate.
All cases of TC occurring in patients aged 85 years or older (n=355) or that were first discovered at autopsy (n=69) were excluded from the analyses. The remaining 18,097 cases were coded using the International Classification of Diseases for Oncology, 3rd edition (ICD-O-3) and stratified into the four major histological subtypes (22): PTC (ICD-O-3 codes 8050, 8052, 8260, 8263, 8340–8344, 8350, 8450), follicular thyroid carcinoma (FTC; ICD-O-3 codes 8290, 8330–8332, 8335), anaplastic thyroid carcinoma (ATC; ICD-O-3 codes 8020–8022, 8030–8033, 8190, 8337), and medullary thyroid carcinoma (MTC; ICD-O-3 codes 8246, 8345–8346, 8510). The remaining ICD-O-3 codes were categorized as “other” (150 cases) or “unknown” (1,782 cases) and excluded from the computations. Notably, all cases included in the present analyses were microscopically confirmed.
IRs were age-standardized by direct method (23) to both the 1991 Italian and the world standard populations, using SEER*Stat 6.5.1. As no appreciable change in trends emerged using the two different standard populations, only the estimates based on the former standard population were used. IRs were reported by sex, place of residence, period of diagnosis (1991–1995, 1996–2000, 2001–2005), and histology (PTC, FTC, MTC, ATC). Ninety-five percent confidence intervals (CIs) of IRs were computed according to the Poisson distribution (23). For CRs with >10 years of registration, the estimated annual percent change (EAPC), by sex, was also calculated for PTC from a log-linear model, using the calendar year as covariate. Female-to-male (F/M) ratios, place of residence and histology, were also analyzed.
Joinpoint regression analysis was used to identify time points (in calendar years) where changes had possibly occurred (24). Using Joinpoint software package 3.4, a logarithmic transformation of the IRs and a maximum number of three joinpoints were specified as options within the program. The final model, selected between models with 0, 1, 2, and 3 joinpoints, was the most parsimonious of these (24), and EAPC between each segment was calculated. To evaluate heterogeneity of observed trends for PTC, joinpoint regression analysis was stratified by CRs reporting IRs for PTC, in 2001–2005, significantly higher or lower (and not significantly different) than pooled estimates in men and women combined.
Results
Between 1991 and 2005, 10,085 female cases and 2,849 male cases of PTC below the age of 85 years were recorded by Italian CRs (Table 1). There was a wide geographical heterogeneity that increased with time (Table 1 and Fig. 1). In the 1991–1995 period, IRs in women ranged from 3.5/100,000 in Latina to 8.5/100,000 in Sassari (a 2.4-fold difference). In the 2001–2005 period, they ranged from 7.3/100,000 in Alto Adige to 37.5/100,000 in Ferrara (a 5.1-fold difference). In the 1991–1995 period, IRs in men varied 4.9-fold in Latina compared to Sassari (0.7/100,000 in Latina, 3.4/100,000 in Sassari). In the 2001–2005 period, IRs varied 5.3-fold in Alto Adige and Trento compared to Ferrara (2.0/100,000 in Alto Adige and Trento, 10.6/100,000 in Ferrara) (Table 1). Figure 1 shows the geographical distribution of CRs and the corresponding IRs of PTC during the most recent 5-year period (i.e., 2001–2005). In both sexes, IRs significantly higher than pooled estimates emerged in the CRs located in the Po River plain (Brescia, Ferrara, Modena, Parma, Reggio Emilia, Romagna) and in Latina CR, whereas lower IRs were noted in the Alpine belt.
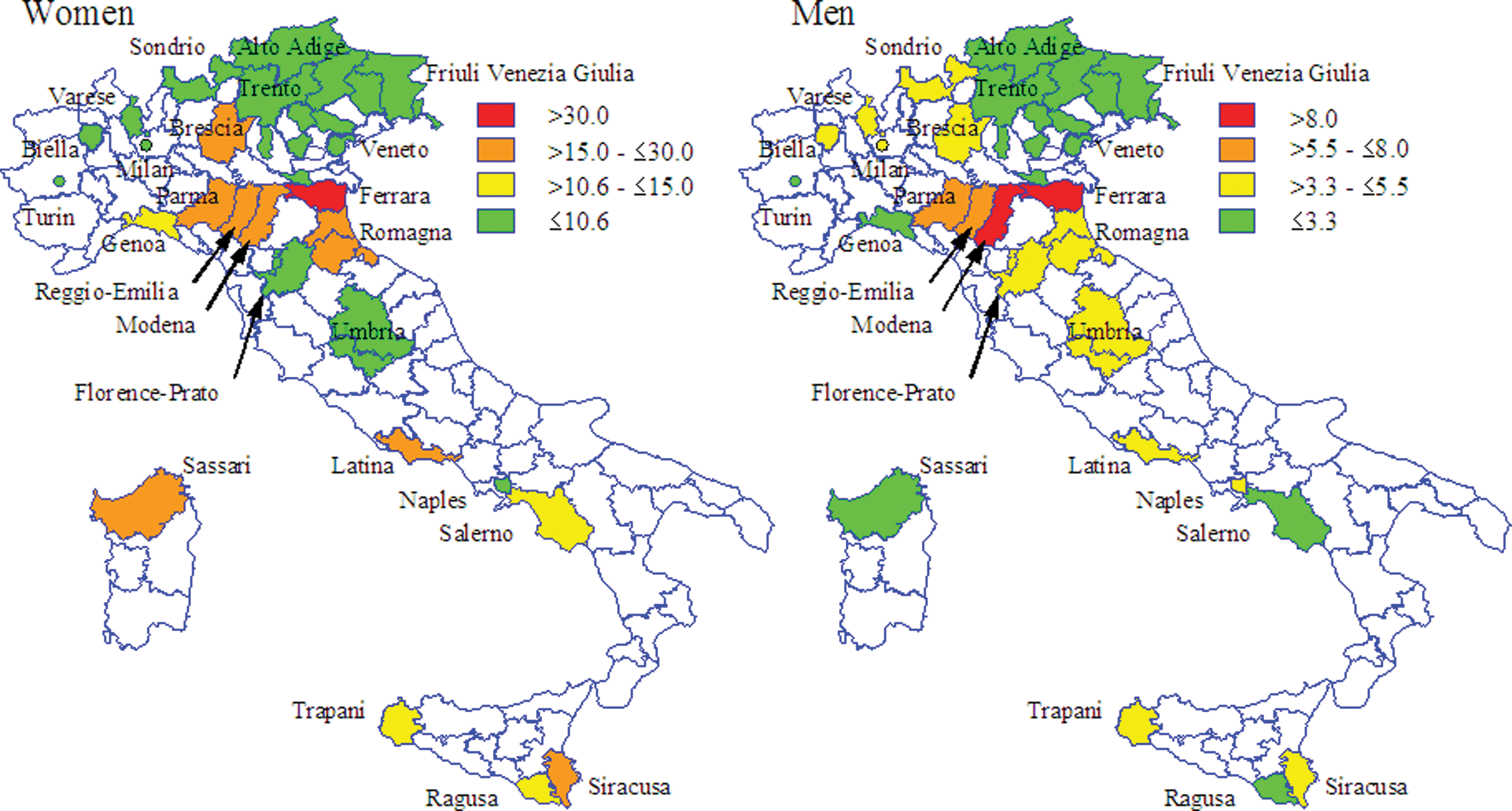
Geographical distribution of incidence rates (IRs) for PTC by sex in 25 Italian cancer registries (2001–2005). The IRs used are truncated (0–84 years) rates per 100,000, age-standardized to the 1991 Italian population; categories were chosen as follows: the first (in green) represents IRs that were significantly below the pooled IR estimates; the second (in yellow), IRs not significantly different from the pooled IR estimates; the third (in orange), IRs significantly higher than the pooled IR but lower than twofold higher; finally, the last categories (in red) represent IRs greater than twofold higher compared with the pooled IR estimates.
IRs for all CRs were more than twofold higher in 2001–2005 than in 1991–1995 in both women (13.6 and 5.6/100,000) and men (4.1 and 1.8/100,000) (Table 1). The annual change between 1991 and 2005 was +9.6% in women (95% CI: +8.8%, +10.4%) and +8.7% in men (95% CI: +7.0%, +10.5%). Restricting the analysis to CRs with >10 years of complete registration (annual change of +9.7% in women and +8.5 in men) or to CRs with complete registration in the period 1996–2003 (annual change of +9.9% in women and +8.5 in men; data not shown) did not modify the results. Joinpoint analysis showed no departure from linear trend either for the pool of all CRs or for each single CR analysis. Substantial heterogeneity in incidence trends was observed, with EAPC values ranging from +0.8% (Friuli Venezia Giulia) to +19.1% (Latina) in women. Significant yearly increases were found in 14 of 15 CRs. CRs showing higher than +9% EAPC were the same ones for both sexes (Ferrara, Genoa, Modena, Parma) (Table 1).
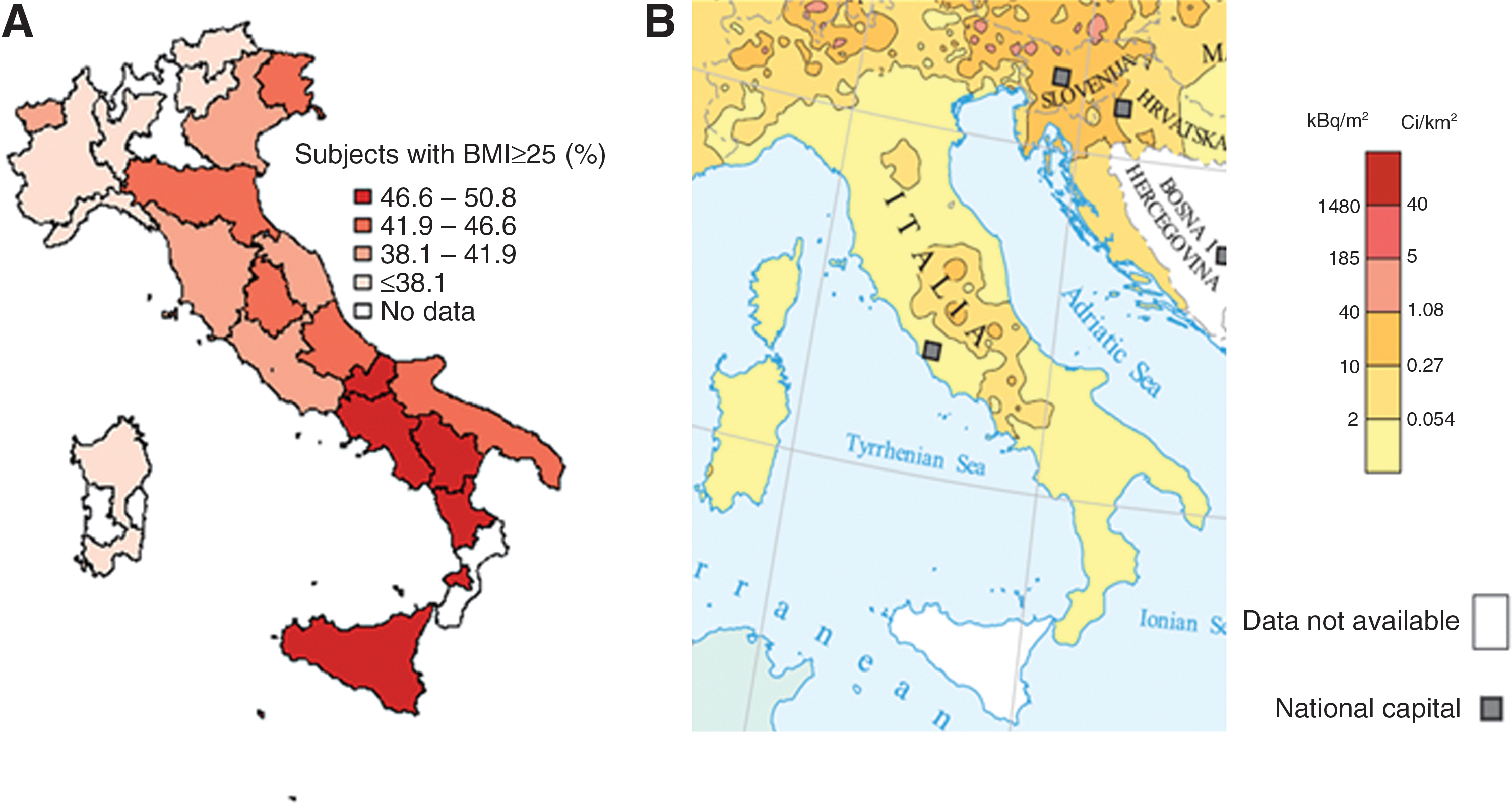
Figure 2 shows the geographical distribution of two factors suggested as possible determinants of TC incidence: the prevalence of overweight subjects (Fig. 2A) in Italy, and the distribution of surface ground deposition of caesium-137 after the Chernobyl accident (Fig. 2B).
Overall, 6,226 PTCs were diagnosed in 2001–2005 (out of 12,934 in 1991–2005), and estimates of IRs in the most recent period by sex and CRs are shown in Fig. 3. PTC (73% of all TC in women and 66% in men) had the highest pooled estimate IRs amongst the histological subtypes (13.6/100,000 and 4.1/100,000 in women and men, respectively). More than fivefold differences in the different IRs for PTC were noted in men and women, though the differences were greater among women. In both men and women, the CRs in the Emilia-Romagna (Ferrara, Modena, Parma, Reggio Emilia, and Romagna) had the highest IRs.
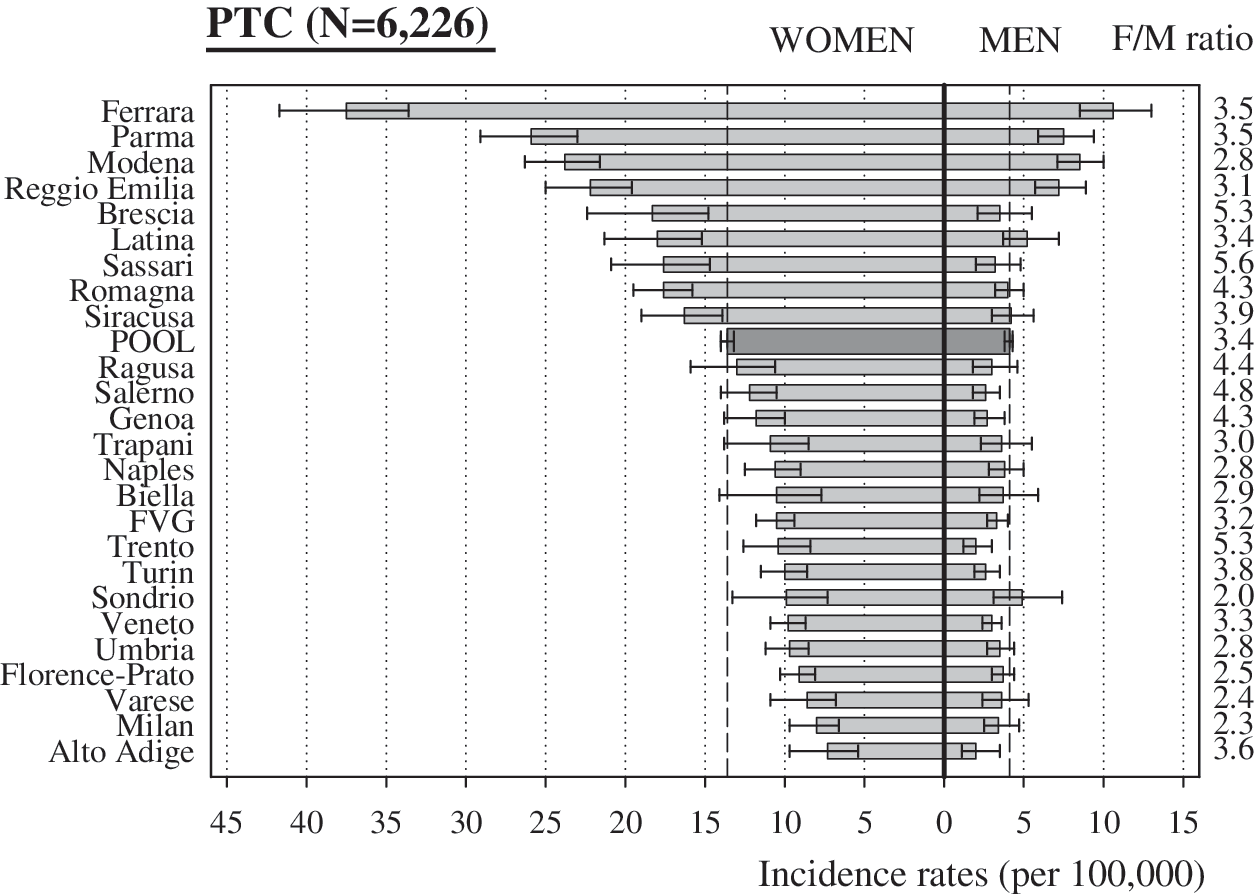
IRs for PTC and F/M ratio in 25 Italian cancer registries (2001–2005). The IRs used are truncated (0–84 years) rates per 100,000, age-standardized to the 1991 Italian population; the bars represent 95% confidence intervals and dashed lines represent pooled IRs. FVG, Friuli Venezia Giulia; F/M, female-to-male.
Figure 4 shows the IRs for other histological subtypes of TC during the 2001–2005 period. The data for CRs with >15% proportion of TC cases in “not otherwise specified” category (Latina, Florence-Prato, Ragusa, Trapani, and Trento) were not included. Pooled IRs for 691 (out of 1,850 in 1991–2005) cases of FTC were 1.6/100,000 and 0.7/100,000 in women and men, respectively. In women, IRs significantly higher than the pooled estimates were only noted in Brescia, Romagna, and Turin. In contrast, significantly lower IRs were noted in Friuli Venezia Giulia, Milan, and Veneto. ATC (118 cases, out of 376 in 1991–2005) had the lowest IRs amongst the histological subtypes (0.2/100,000 pooled estimate for both sexes) with no indication of heterogeneity among the different CRs. Pooled IRs for 257 (out of 612 in 1991–2005) MTC cases were 0.5/100,000 and 0.3/100,000 in women and men, respectively. Significantly higher IRs than pooled estimates were reported for women, in the Parma (1.4/100,000), Modena (1.1/100,000), and Romagna (0.9/100,000) CRs. The F/M ratios were higher for PTC (3.4; 95% CI: 2.8, 3.1) (Fig. 3) and FTC (2.5; 95% CI: 2.1, 3.0) than for MTC (1.7; 95% CI: 1.3, 2.3) and ATC (1.3; 95% CI: 0.9, 1.9) (Fig. 4).
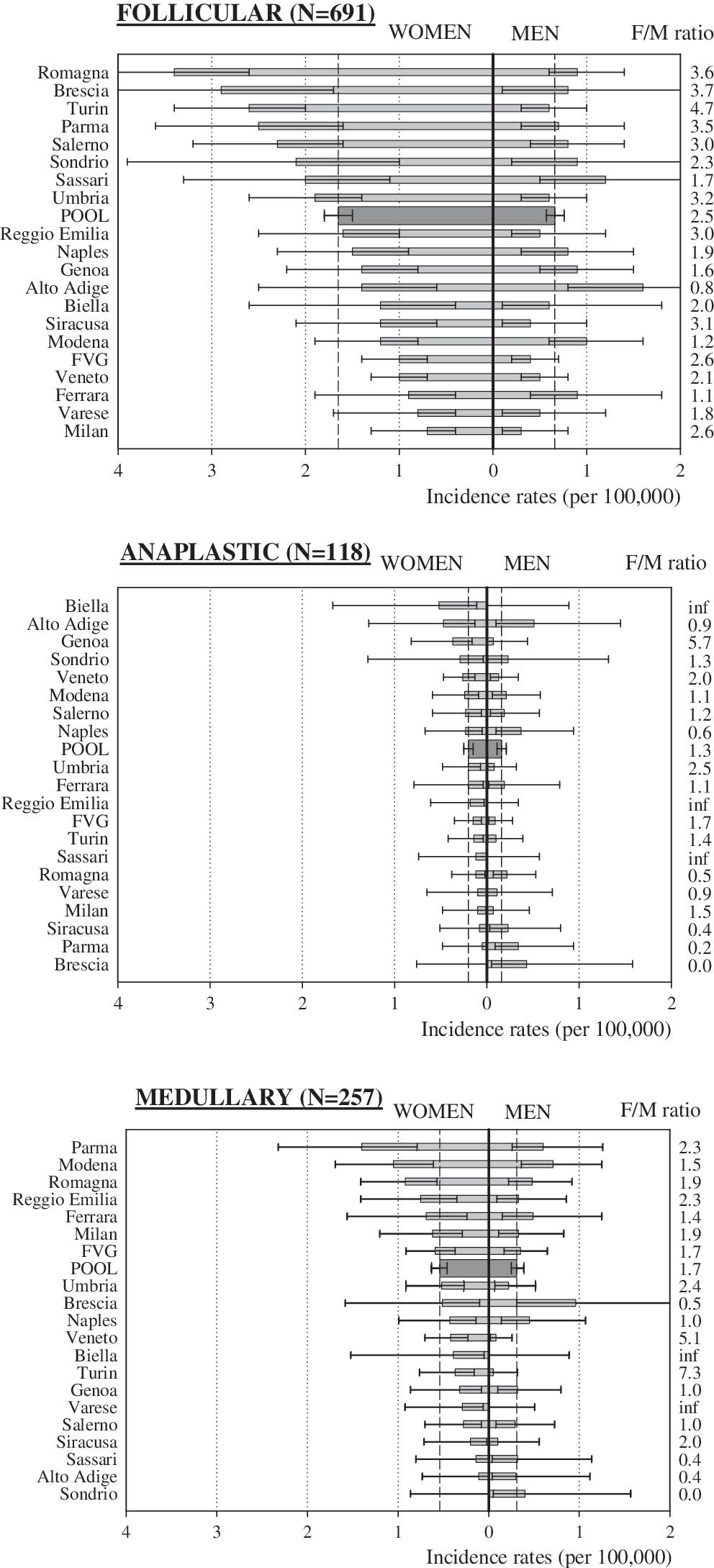
IRs for TC and F/M ratio by histological subtypes in 25 Italian CRs (2001–2005). The IRs used are truncated (0–84 years) rates per 100,000, age-standardized to 1991 Italian population; CRs with % not otherwise specified of >15% (Latina, Florence-Prato, Ragusa, Trapani, Trento) were excluded; bars represent 95% confidence intervals and dashed lines represent pooled IRs.
Figure 5 shows trends by sex and CRs, reporting IRs for PTC in 2001–2005 that were significantly higher versus lower (and not significantly different) than pooled estimates, together with the corresponding linear slopes as estimated from joinpoint analyses. In both men and women, the variations in IRs between the two groups of CRs were small until 1995 and became gradually wider during the 1996–2005 period. The pattern was unchanged for CRs having complete registration in the restricted period, 1996–2003 (data not shown).
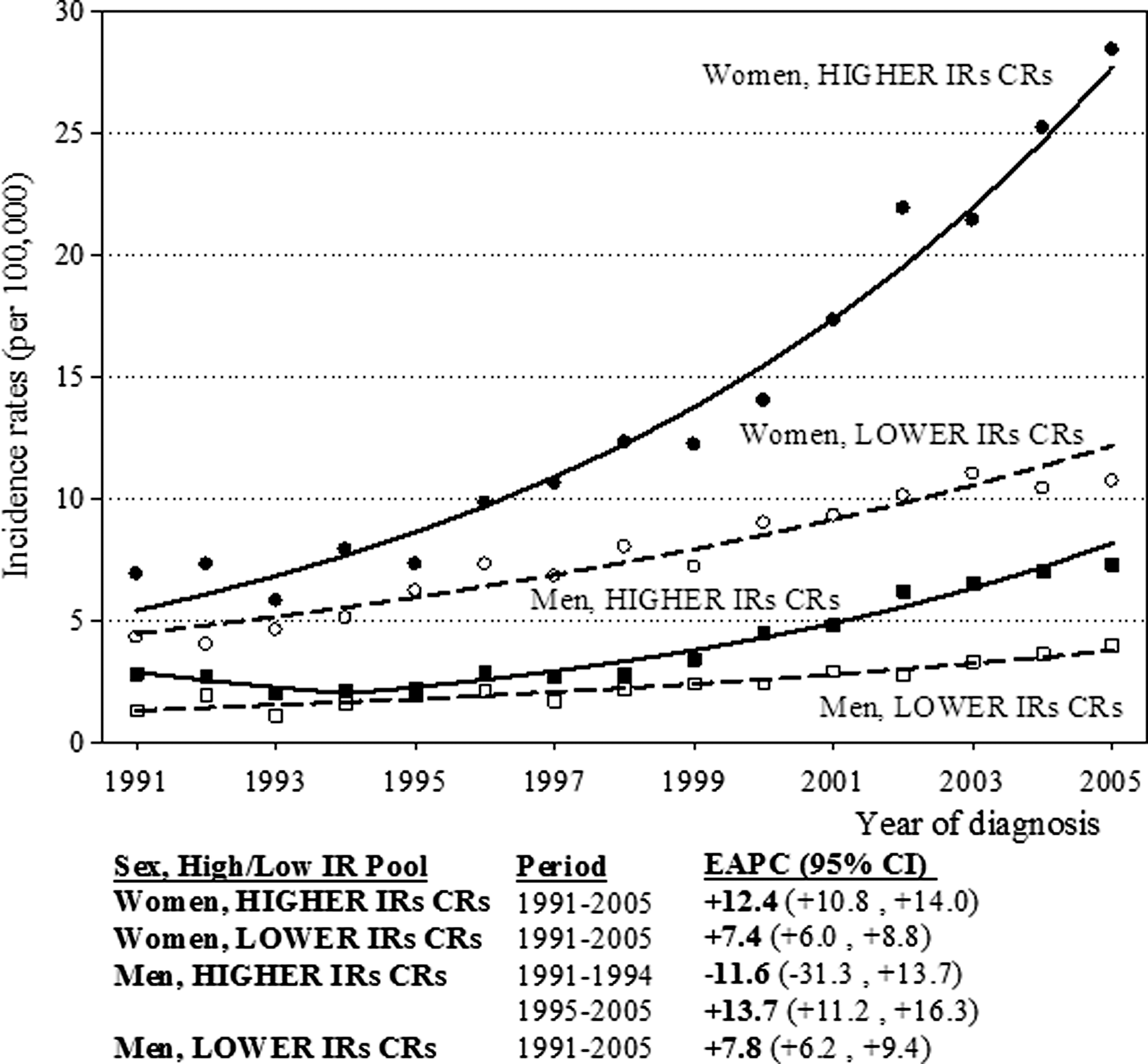
Trends of incidence rates of PTC by sex and cancer registry (CR) with different level of IRs in Italy, 1991–2005. The IRs used are truncated (0–84 years) rates per 100,000, age-standardized to 1991 Italian population. Solid and dashed lines represent fitted trends, based on joinpoint regression using a logarithmic transformation of the rates, by sex, and CRs with different level of IRs. Higher IRs CRs: CR with IRs for PTC significantly higher than the pooled one, in 2001–2005 (Brescia, Ferrara, Latina, Modena, Parma, Reggio Emilia, Romagna, Sassari, Siracusa); Lower IRs CRs: CRs with IRs for PTC lower or not statistically different than the pooled one, in 2001–2005 (Alto Adige, Biella, Florence and Prato, Friuli Venezia Giulia, Genoa, Milan, Naples, Ragusa, Salerno, Sondrio, Trapani, Trento, Turin, Umbria, Varese, and Veneto) (see Fig. 1).
Discussion
Wide geographic heterogeneity in the incidence of TC was observed in Italy; for PTC, this variation appeared to increase between 1991 and 2005.
Patterns of TC incidence were almost exclusively due to PTC, increasingly the most common histological subtype (3). The rise in the identification of small indolent TCs mainly concerns PTC incidence rates (25). Our study was limited by the lack of information on tumor size and diagnostic modalities as they were not systematically recorded by the Italian CRs. However, stable or decreasing TC mortality rates in Italy, as well as in other countries (5,15), indirectly supports the predominance of early detected PTC with a good prognosis as accounting for the upward trend in TC. In our study, the incidence of FTC was also geographically heterogeneous but this was not the case for ATC or MTC, possibly also because of their rarity. The IRs for MTC increased slightly in Italy between 1991 and 2005, whereas those for FTC and ATC did not change (3).
The mean incidence of PTC has nearly doubled in Italian CRs between the 1991–1995 and 2001–2005 periods, with almost all CRs reporting an increase. The differences between CRs in the most recent period were merely the consequences of differences in trends, suggesting that heterogeneity was a relatively recent phenomenon.
As elsewhere, upward trends for both sexes in different parts of Italy in our study were most likely attributable to increased medical surveillance of thyroid nodules and symptoms potentially related to thyroid gland dysfunction (12,25 –27). We recently obtained evidence that the greater use of healthcare services by young and middle-aged women (because of events related to reproduction and peri- and postmenopausal symptoms) than by men of the same age made the impact of diagnostic changes emerge more rapidly and at an earlier age in women (3). The greater increase of PTC in women, also because of their higher prevalence of benign thyroid conditions, is consistent with this (28).
Wide geographic variations in the incidence of PTC and the lack of a clear north–south or urban–rural pattern suggests that the variations correlate with patchy differences in local medical practices. Specialized centers of research, detection, and treatment of benign thyroid diseases and TC are unequally distributed across Italian regions, but diagnostic ultrasound technologies and thyroid hormone assays have been widely available in Italy since the early 1980s (29). Geographic variations in the IRs for PTC could be related to socioeconomic-based differences in healthcare access (16). In Italy, income level has a north–south gradient, with regions at highest income located in the north of the country. This does not seem consistent with the pattern of the incidence of PTC noted in the present study. However, Italy has a universal health care system that guarantees equal access to diagnostics throughout the country, independently of income level.
Along with medical surveillance, other factors varying locally and potentially affecting the observed incidence of PTC could not be fully excluded by this study. The best-established cause of PTC is exposure to ionizing radiation, particularly during childhood (30). In our study, the distribution of PTC does not lend support to a role of environmental radiation exposure due to the Chernobyl fallout in 1986. The areas that experienced the highest deposition of caesium-137 after the Chernobyl accident (North Italy and Umbria) (Fig. 1) (31) showed among the lowest incidences of TC in Italy (Fig. 2B). However, it can be speculated that an increase in diagnostic radiological examinations, which have doubled in the past 10–15 years in the United States and other countries (32), might be partly responsible for to the upward trends of PTC in some areas. The use of radiation treatment for benign childhood conditions in the 1950s and 1960s (e.g., thymic enlargement) might have contributed to the increasing trends of PTC in Italy (33). As there has not been a nationwide survey of medical radiation exposures it is not known if variations in medical radiation exposure are correlated with the incidence of PTC.
Despite the fact that iodine deficiency is an established risk factor for FTC and ATC (34), the relationship between the incidence of PTC and varying degrees of iodine intake has been inconsistent (8,35). Although subclinical iodine deficiency has been frequently reported in many Italian areas (36), no systematic campaign of iodine supplementation was undertaken in Italy prior or during the study period. CRs located near the Alps and the Apennine Mountain Ranges, where iodine in soil and water is at the lowest levels, had, in fact, some of the lowest IRs for PTC in Italy.
A possible association between the incidence of PTC and the presence of volcanic soil has also been suggested (17). In our study, the highest IRs of PTC were found in CRs located in the Po River plain. The only CR located in a volcanic area (Mount Vesuvius) is the Naples CR, where low IRs for PTC were obtained for both men and women. Therefore it seems unlikely that exposures related to volcanic soils may account for the rapidly increasing incidence of PTC (37).
Some evidence for an association between obesity and TC has been reported (35,38). In Italy, the prevalence of obesity has a north-south gradient (Fig. 2A) (39); this contrasts with the incidence pattern of PTC found in our study (Fig. 1). Despite the increasing number of overweight subjects in most developed countries, a moderate body mass index (BMI) increase for men and a modest BMI decrease for women were reported in Italy between 1980 and 2008 (40).
Lack of nationwide information on the incidence of cancer and the low number of CRs in Southern Italy are the main limitations of the present study. However, the completeness and quality of Italian CRs have been considered to be satisfactory (2,21). Conducting homogenous quality checks (41) guarantees comparability of IRs between areas in Italy. Moreover, the limited population mobility and the strict policy for keeping updated a subject's residence in Italy provided reassurance on the negligible effect of misclassification between areas.
To better understand the causes for the differences in the incidences of TC in various parts of Italy, CRs should collect information on the diagnostic modalities used in their region and on lifestyle and environmental factors that are thought to affect the risk of TC. The consequences of the current policy of intensely searching for PTC, with the resulting possibility of overtreating indolent tumors (42), evoking more expenditures, and increased morbidity associated with thyroidectomy and thyroid hormone replacement (especially in young women), need careful consideration.
Footnotes
Acknowledgments
M.L. was supported by a fellowship from the Italian Association for Cancer Research (AIRC) carried out at the International Agency for Research on Cancer. The authors thank Mrs. Luigina Mei for editorial assistance.
Disclosure Statement
The authors have no conflict of interests to declare.