
Abstract
Background:
Patients with severe Graves' orbitopathy often have hyperthyroidism that is difficult to treat and a high proportion of patients experience relapse of hyperthyroidism after a course of antithyroid drug (ATD) therapy of fixed duration. The aim of the study was to evaluate the feasibility of prolonged low-dose ATD therapy for attaining stable euthyroidism in patients with severe Graves' orbitopathy and hyperthyroidism.
Methods:
We performed retrospective analyses of data collected during observation of a cohort of patients (n = 108) treated for severe Graves' orbitopathy and for hyperthyroidism using partial block with low-dose thionamide + replacement with levothyroxine (L-T4) for >2 years. The study was performed at a university hospital referral center for patients with severe Graves' orbitopathy.
Results:
The median duration of thionamide therapy was 80 months (25–75 percentiles: 55–115 months); 101 patients received methimazole (median: 5 mg/day) without side effects during prolonged therapy, and 7 propylthiouracil (median: 200 mg/day); median L-T4 dose was 0.1 mg/day. Ninety percent of patients remained euthyroid throughout the period of therapy, and 65% of them had thyroid stimulating hormone (TSH) receptor antibodies in serum within the assay reference interval at the last observation. Only four (3.7%) developed episodes of hyperthyroidism during stable therapy, and 94% had serum TSH within 0.1–4.0 mU/L at the last observation. One patient developed reversible cutaneous vasculitis after 6 years of propylthiouracil therapy.
Conclusions:
Prolonged partial block plus replacement therapy with low-dose ATD + L-T4 keeps the majority of patients with severe Graves' orbitopathy and hyperthyroidism stable and euthyroid.
Introduction
TSH receptor autoimmunity gradually disappears in many patients with Graves' disease when they are made euthyroid by administration of antithyroid drugs (ATDs) (11), but such therapy is normally given for a fixed period of 1–2 years only (12). Relapse of hyperthyroidism after withdrawal of ATD therapy is very common in patients with severe Graves' orbitopathy (4).
Some evidence supports that keeping patients with Graves' disease euthyroid is important for achieving and sustaining remission of the autoimmune disorder (13). We report on our experience with the prolonged use of partial block plus replacement therapy of hyperthyroidism in a group of patients who suffered from severe Graves' orbitopathy. In the majority of patients, this therapy was successful in keeping patients stable and euthyroid and with few side effects only from therapy. These findings are in accordance with publications on the prolonged use of ATD therapy in other groups of patients with Graves' disease (14 –18).
Methods
We retrospectively evaluated the course of hyperthyroidism in a group of 108 patients suffering from Graves' disease with hyperthyroidism. At enrolment, all patients had active Graves' orbitopathy that ranged from moderate–severe to sight threatening, as described in the European Consensus Statement (9). After enrolment they had been followed for at least 2 years in our Graves' orbitopathy clinic and had received ATDs for >2 years. Figure 1 illustrates criteria for selection of patients for the present study.
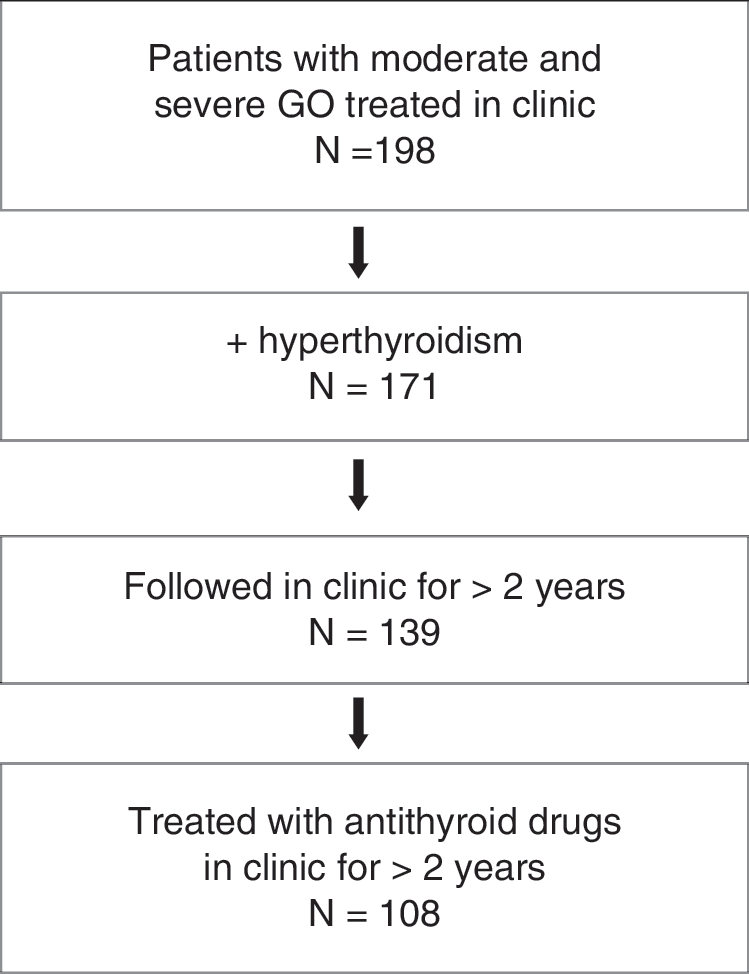
Criteria for selection of patients for the present study. GO, Graves' orbitopathy.
Of our cohort of patients with this type of Graves' orbitopathy and hyperthyroidism, all of whom had been followed for >2 years (n = 139) (Fig. 1), 31 had undergone surgical thyroidectomy after being treated with ATDs for <2 years. These were patients who had large goiters or did not respond properly to ATDs (19) or, for some other reason, preferred surgery to ATD therapy.
TSH receptor antibodies (TRAb) in serum was measured using TRAK-human (BRAHMS, Berlin, Germany; analytical sensitivity of 0.3 IU/L, reference: <1.0 IU/L), as previously described (20). TSH, thyroxine (T4), and triiodothyronine (T3) in serum were measured using standard automated assays. TSH values given were analyzed with Roche Modular E® system by electrochemical luminescence using ELECSYS® TSH reagents. We used SPSS (version 15.0; Chicago, IL) for analyses of data.
Results
Patients studied
Characteristics of the 108 patients studied at the time of enrolment including some manifestations of the orbitopathy are given in Table 1. All patients had a Caucasian ancestry except for one male of Asian ancestry. Eight had received radioiodine therapy for the current hyperthyroidism before referral, but still needed ATDs. Three had previously undergone partial thyroidectomy. A total of 15 of the 108 patients had been previously treated for hyperthyroidism, before the current disease.
Depending on the manifestations, severity, and course of the orbitopathy, all the patients had initially received some combination of medical immune suppression, orbital irradiation, and eye surgery (9).
Therapy of hyperthyroidism
All patients had been started on methimazole before admission or were started at admission on a drug dose depending on the severity of the hyperthyroidism (this is standard therapy in Denmark). When serum T4 and T3 had become normal or near normal on ATD therapy, the principle used was to reduce the dose, for example, methimazole 10 mg once daily and gradually to add levothyroxine (L-T4) (partial block + replacement). Subsequently, during prolonged therapy, the dose of methimazole was further reduced to 5 mg once daily in many patients, and by adjustment of doses of ATD and L-T4, we aimed at keeping serum TSH within the range of 0.3–3.0 mU/L. The range 0.1–4.0 mU/L was considered acceptable. At the end of follow-up, the duration of ATD therapy was 80 months (55–115), the dose of methimazole was 5 mg/day (5 –10), the dose of propylthiouracil (PTU) was 200 mg/day (100–200), and the dose of L-T4 was 100 μg/day (100–127), with all values in parentheses being the 25th to 75th percentiles.
Stability and relapse of hyperthyroidism during prolonged low-dose ATD + L-T4 therapy
The majority of patients remained euthyroid on the prolonged ATD therapy, and only a minor fraction had episodes of hyperthyroidism as shown in Figure 2. In seven patients, this occurred a few months after the dose of methimazole had been reduced from 10 to 5 mg/day. They all developed mild biochemical and clinical abnormalities, and they responded well to a return in the methimazole dose to 10 mg/day. Four patients had regular relapse of hyperthyroidism during stable prolonged partial block plus replacement therapy.
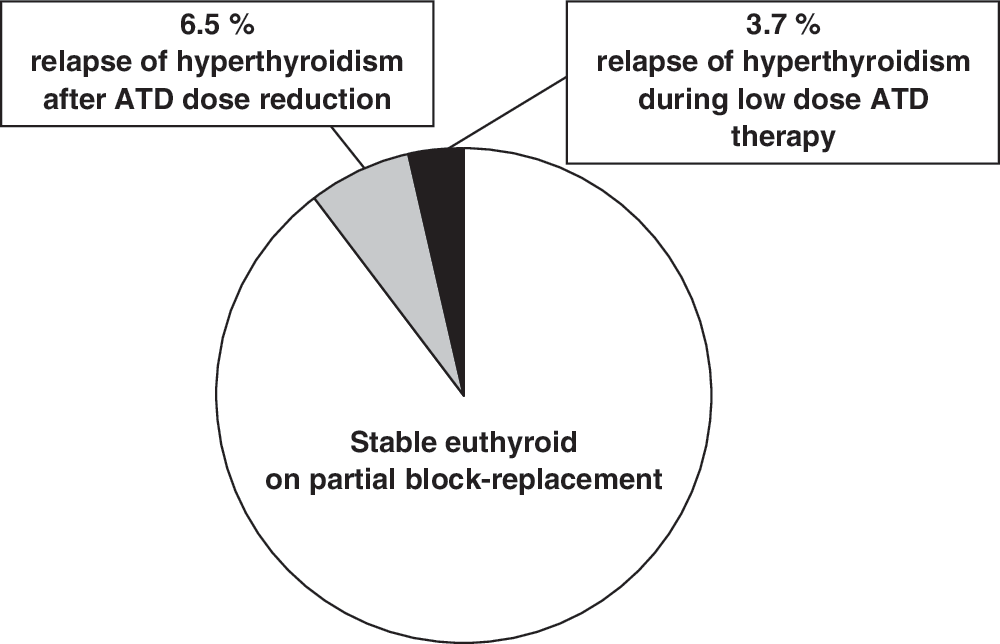
Outcome of prolonged (median: 80 months) low-dose medical therapy for hyperthyroidism in 108 patients with severe Graves' orbitopathy and hyperthyroidism: Proportion of patients remaining stable and euthyroid during partial block + replacement therapy with low-dose ATD + L-T4, patients who became hyperthyroid after reduction of the dose of ATD, and patients who had relapse of hyperthyroidism during prolonged partial block + replacement. ATD, antithyroid drug; L-T4, levothyroxine.
After some years of clinical and biochemical stability, the patients were typically seen for management once yearly. At the most recent visit, while on ATD + L-T4 therapy, 6 of the 108 patients had TSH outside the range 0.1–4.0 mU/L (TSH values were 0.010, 0.010, 0.031, 0.074, 4.1, and 5.9 mU/L). All patients had serum T4 and T3 within the laboratory reference range. Median serum TSH was 1.10 mU/L (25–75 percentiles: 0.63–1.80 mU/L). At testing 1 year previously, four patients had TSH outside the range 0.1–4.0 mU/L.
The possibility of ATD withdrawal was discussed with the patients after some years. The majority preferred continuing drug therapy, and therapy had been stopped in 22 patients only (after a median duration of ATD therapy of 70 months). All these patients had no TRAb measurable (<1.0 IU/L) at the time of ATD withdrawal. Two experienced relapse of hyperthyroidism during a median follow-up of this group of patients of 24 months. None of the two had reactivation of orbitopathy in relation to this.
In many patients, TRAb gradually disappeared from serum during therapy. At the most recent control on medication, TRAb was <1.0 IU/L in 53 of the 81 (65%) patients who had stayed euthyroid and in whom TRAb had been measured using the current improved assay. At the time of inclusion, TRAb had been measured using this assay in 52 of the patients and was <1.0 IU/L in 3 only (6%).
Side effects to prolonged ATD therapy
Seven of the 108 patients had an early shift of ATD from methimazole to PTU either before or after admission to our clinic. This was mostly due to suspicion of cutaneous reactions occurring within the first months of therapy (n = 5, none severe). One patient had slightly elevated circulating liver enzymes and one had moderate arthralgia, both with no clear relation to methimazole therapy.
The only serious side effect to ATD therapy observed in the present study occurred in a 48-year-old woman. She had a cutaneous rash after 3 weeks of methimazole therapy and this was changed to PTU. After 6 years of uncomplicated PTU therapy, she developed vasculitis with small cutaneous ulcerations confined to the nose and the ear lobes (Fig. 3).

Cutaneous necrosis on ear lobe in a patient treated with PTU for 6 years. The patient had positive reaction for MPO (myeloperoxidase)–ANCA (antineutrophil cytoplasmic antibodies) (18 U, ref. <10). The vasculitis disappeared and MPO-ANCA became negative after a short course of prednisolone therapy and withdrawal of PTU. The patient was subsequently followed for 4 years without medication and remained euthyroid. PTU, propylthiouracil.
Discussion
Principal findings
This observational study of prolonged low-dose ATD + L-T4 therapy of hyperthyroidism in 108 patients with severe Graves' orbitopathy and hyperthyroidism illustrates that this mode of therapy is feasible, although not a perfect way of controlling thyroid function in such patients.
Comparison with previous studies
Standard ATD therapy of the hyperthyroidism of Graves' disease aims at making and subsequently keeping the patients euthyroid on the drug for a fixed period of time, which may be 12–24 months (12). After ATD withdrawal, patients with a more severe autoimmune abnormality, such as those developing Graves' disease during childhood (21), and those with persistently measurable TRAb in serum (11), a large goiter (22,23), or severe orbitopathy (4) have a high risk of relapse of hyperthyroidism. The risk is also high in smokers (24,25) and after excessive iodine intake (26).
Previously, the outcome of ATD therapy in patients with severe Graves' orbitopathy was little studied except for the publication by Eckstein et al. (4). They treated hyperthyroidism in patients with Graves' hyperthyroidism and orbitopathy with ATDs for 12 months, followed by withdrawal of medication. In the patients with severe Graves' orbitopathy, 92% had relapse of hyperthyroidism within 12 months after withdrawal of ATDs. This outcome markedly differs from the prolonged euthyroid state observed in the majority of patients in the present study. Ninety percent of our patients who initially suffered from hyperthyroidism and severe orbitopathy remained stable and euthyroid on low-dose block + replacement therapy during a median observation period of nearly 7 years.
As previously discussed (13), hyperthyroidism per se may aggravate the autoimmune activity of Graves' disease, and thyroid stimulation by elevated serum TSH may also be associated with worsening (7). Thus, a primary goal of therapy for hyperthyroidism in patients with Graves' orbitopathy is to make and keep the patients euthyroid.
Recently, Elbers et al. (27) published results of a questionnaire based retrospective follow-up study of patients with concomitant Graves' orbitopathy and hyperthyroidism. Compared with our study, the duration of therapy was shorter (median: 41 months), and therapy was discontinued in all the 73 patients studied. Observation after the discontinuation was for a median period of 57 months and the recurrence rate of hyperthyroidism was 37%. TSH receptor antibodies were not measured. In this Dutch study (27), the dose of MMI was kept at (nearly) full blocking dose, and no side effects were reported. The relapse rate of 37% was much lower than that reported by Eckstein et al. (4) after withdrawal of ATDs after 12 months of therapy, which may support the use of more prolonged therapy. Still, the relapse rate was not negligible in the Dutch study, but detailed comparisons of the different observational studies might be biased.
Side effects from therapy
One problem with the thionamide drugs is the relatively high rate of side effects seen in around 5% of patients (28). This leads to great alertness among physicians and patients, especially during the initial period of therapy when most side effects occur. We used primarily methimazole therapy, which has advantages compared with PTU (12,28). Side effects to methimazole are dose dependent (29,30) and we attempted to use small doses for the prolonged therapy. We observed no side effects to methimazole during the late phase of therapy.
One of the few PTU-treated patients developed antineutrophil cytoplasmic antibody–positive vasculitis after 6 years of therapy. This is a well-known side effect of prolonged PTU therapy that may lead to serious morbidity (31). As recommended by Gunton et al. (32), PTU may be less well suited for long-term therapy of hyperthyroidism, and if used, any unexplained clinical symptom and sign should be further evaluated on suspicion of a PTU side effect. Antineutrophil cytoplasmic antibody–positive vasculitis has been also reported during carbimazole and methimazole therapy, but this is much less common (31,32). The rare complication of liver failure during PTU therapy has also attained focus recently (33,34). Thionamide ATDs are very useful for treating hyperthyroidism in the majority of patients; however, development of ATDs with fewer side effects is needed (19).
Study limitations
The present study is an observational study, with the principal limitation of having no direct controls. The early phase of therapy of hyperthyroidism had been often performed before patients were referred for the orbitopathy and standardized evaluation, before ATD therapy had been not given. A minor part of the original cohort of patients with severe Graves' orbitopathy and hyperthyroidism underwent early surgical thyroidectomy. As this included patients with large goiter and insufficient response to ATD therapy, some of the patients with the most severe autoimmune abnormality of Graves' disease may not have been included in the selected cohort studied.
Nearly all patients received immunosuppressive medical therapy in the early phase of therapy for orbitopathy. It cannot be formally excluded that the low rate of relapse of hyperthyroidism observed was caused by this initial immunosuppressive therapy, although we consider this unlikely and it is not supported by other studies (4). A more likely explanation is the prolonged low-dose ATD therapy given. Several investigators have previously published on the feasibility of prolonged, mostly low-dose ATD therapy in patients with Graves' disease to avoid relapse (14 –18).
We used a low dose of ATDs to reduce the risk of side effects and combined this with L-T4 (partial block + replacement). L-T4 was added to optimize stability of thyroid function during the initial phase of active orbitopathy and to reduce the need for frequent thyroid function testing during prolonged therapy. The design of the present study does not allow any conclusion on the benefits of such a strategy of therapy versus low-dose ATD therapy without addition of L-T4 replacement.
Conclusion
In this observational study, prolonged low-dose block + replacement therapy of hyperthyroidism kept 90% of patients with Graves' hyperthyroidism and severe orbitopathy euthyroid for prolonged periods. Prospective randomized studies are needed to expand our understanding of the usefulness of prolonged ATD therapy in patients with Graves' disease.
Footnotes
Disclosure Statement
The authors have nothing to disclose.