
Abstract
Background:
Graves' disease (GD) is caused by the continuous stimulation of the thyroid gland by autoantibodies directed against the thyroid-stimulating hormone receptor (TSHR). Two frequent assays for the measurement of TSHR autoantibodies (TSHRAb) were compared, one measuring stimulation of cyclic adenosine monophosphate (cAMP) production and one measuring inhibition of TSH binding, with regard to diagnostic accuracy for GD as well as whether there was an existence of their discordant results in patients with GD and painless thyroiditis (PT).
Methods:
Using 106 sera from untreated GD and 80 sera from autoimmune PT, we compared the diagnostic performance of two TSHRAb assays that have been recently developed. The first one is a bioreporter assay using chimera TSHR (Mc-4), which detects a stimulation signal of cAMP level in cultured CHO cells (Mc4-TSAb assay). The second is a binding inhibition assay using the extracelluar domain of porcine TSHR and a monoclonal antibody (M22) closely mimicking the binding to TSH (M22-TRAb assay). In addition, we compared both assays by using eight sera from eight GD subjects becoming spontaneously hypothyroid due to appearance of thyroid blocking autoantibodies (TBAb) that were measured with inhibition rates of TSH-stimulated cAMP in porcine cells.
Results:
The Mc4-TSAb assay and the M22-TRAb assay were positive in 94.3% and 92.5% of the GD patients, respectively, whereas they were negative in 95.0% and 98.8% of the PT subjects. However, 10 of 106 GD sera (9.4%) showed discordant results. Six of 106 cases with untreated GD (5.7%) were Mc4-TSAb positive and M22-TRAb negative. In contrast, 4 of 106 sera (3.8%) were Mc4-TSAb negative but M22-TRAb positive. Two cases of untreated GD were negative for both Mc4-TSAb and M22-TRAb. In eight GD subjects with TBAb and hypothyroidism, the binding assay was highly positive, although Mc4-TSAb was negative.
Conclusion:
Similar and excellent performance was noted for the Mc4-TSAb and M22-TRAb assays in a large group of patients with GD. However, there was 9.4% discordance with regard to false negatives for GD and 3.8% discordance between the two tests with regard to false positives for PT. With regard to the relatively high rate of discordancy, a combination of both assays could reduce the presence of TSHRAb-seronegative GD.
Introduction
Materials and Methods
Patients
Overall, 106 patients with untreated GD were included in this study (39±13 years, mean±standard deviation [SD]; 10 men and 96 women) as well as 80 patients with autoimmune PT (41±14 years; 4 men and 76 women). Eight patients (54±14 years; 2 men and 6 women) who had developed hypothyroidism due to appearance of blocking type of TSHRAb (TSBAb) during methimazole (MMI) treatment for GD (n=6) or were in remission after MMI withdrawal (n=2) were also investigated. The median duration of MMI treatment (15 mg (n=3) or 30 mg (n=5)/day at initiation) was 14.5 months ranging from 2 months to 468 months. Thyroid weights at the time of diagnosis of hypothyroidism were normal (n=2), mildly enlarged (n=5), and enlarged (n=1). The diagnosis of GD was made on the basis of clinical and laboratory evidence of hyperthyroidism, the presence of a diffusely enlarged thyroid gland, and increased diffuse thyroid uptake 20 minutes after Tc-99m injection (>2.0%) and/or increased vascularity index (>80%) in power color Doppler sonography with positive M22-TRAb, as previously reported (8). The diagnosis of PT was based on laboratory evidence of thyrotoxicosis and decreased diffuse thyroid uptake of 20 minutes after Tc-99m injection (<0.5%) and/or decreased vascularity (<50%) by power Doppler sonography with negative M22-TRAb, as previously reported (8). All serum samples were stored at −20°C. The study was approved by the Committee for Medical Research Ethics of the Kamijo Thyroid Research Institute and the Kamijo Thyroid Clinic. All patients were informed of the purpose of this study and gave their written consent.
Mc4-TSAb assay
The Mc4-TSAb levels in the patients' sera were measured by a novel, FDA cleared bioreporter assay kit-Thyretain® (Diagnostics Hybrids, Inc., Athens, OH) as previously reported (5). This assay detects TSHRAbs by using an Mc-4 chimeric receptor, where the region of the C-terminus TSHR is substituted with amino acid residues of the rat luteotropin-choriogonadotropin receptor (9). Sera samples were diluted 11-fold with reaction buffer, and 100 μL aliquots were added to a well of a 96-well microplate, which was confluent with CHO cells expressing chimeric receptors, together with 100 μL of reaction buffer. The plate was incubated at 37°C, 5% CO2for 3 hours. After discarding the solution, 75 μL of cell lysis solution containing luciferin substrate was added to each plate. Chemiluminescense intensity was measured 10 minutes after the addition of substrate solution. The Mc-4 TSAb level of each serum sample was expressed as a percentage of luciferase production compared with that of the reference control. Based on previous experiments, 128% of Mc4-TSAb level was the optimal cut-off value (5).The intra-assay variation for Mc4-TSAb assay ranged from 2.9% to 7.9% (n=5), and the inter-assay variation stretched across two different reagent lots ranging from 7.5% to 13.0% (n=4).
M22-TRAb assay
The M22-TRAb levels in the patients' sera were measured by an inhibition assay kit- Elecsys anti-TSH receptor assay (Roche Diagnostics GmbH, Penzberg, Germany) according to its instruction manual (6,8). This assay detects TSHRAb by using inhibition of a monoclonal antibody (M22) binding the extracelluar domain of porcine TSHR. The estimated optimal M22-TRAb cut-off value was 2.0 IU/L (10). The intra-assay variation and inter-assay variation for M22-TRAb were 7.8% and 5.3%, respectively (8).
Sera from 110 normal healthy controls (5,8), who were euthyroid, both thyroglobulin antibody (TgAb) and thyroid peroxidase antibody (TPOAb) negative, and had normal thyroid volumes measured by thyroid sonography were all negative for Mc4-TSAb and M22-TRAb.
Free thyroxine, free triiodothyronine, anti-TPOAb, anti-TgAb, and TSH assay
Free thyroxine (FT4), free triiodothyronine (FT3), anti-TPOAb, anti-TgAb, and TSH levels were determined with Elecsys Free T4 assay, Elecsys Free T3 assay, Elecsys anti-TPOAb, Elecsys anti-TgAb, and Elecsys TSH assay (Roche Diagnostics GmbH), respectively.
Measurement of TSBAb activity
Using porcine thyroid cell cAMP system (5), TSBAb activity was assayed by measuring the ability of patients' immunoglobulin G (IgG) to inhibit TSH-stimulating cAMP production in comparison to control IgG response and was calculated as follows (11,12):
TSBAb activity of 50 normal subjects was 1.2%±22.2% (mean±SD); and, therefore, the cut-off value of TSBAb was set as 45.6% (mean+2SD).
The presence of TSBAb was established by the assay previously described in detail by using a porcine thyroid cell cAMP system (5). All sera from eight cases showed marked blocking activities against TSH-induced cAMP increase, ranging from 92.9% to 98.9% (normal range, <45%). Individual data are shown in Table 3.
Statistical analysis was performed by the delta test. Correlations were assessed by the Pearson's method.
Results
Comparison of the diagnostic performance of Mc4-TSAb and M22-TRAb in GD and PT
The Mc4-TSAb over the cut-off value of 128% were detected in 100 of 106 patients with untreated GD (94.3%) and were below the cut-off value in 76 of 80 patients with PT (95.0%). The M22-TRAb greater than the cut-off value (2.0 IU/L) were shown in 98 of 106 patients with untreated GD (92.5%) and in 1 of 80 patients with PT (1.3%) (Table 1). The sensitivities of the Mc4-TSAb and M22-TRAb assays in GD were 94.3% and 92.5%, respectively; whereas the specificities in the patients with PT were 95.0% and 98.8%, respectively. No significant differences between the specificity and sensitivity of the Mc4-TSAb assay and M22-TRAb assays were noted in both patient collectives (n.s.). Using comparative receiver operating characteristic (ROC) analysis, we also compared the diagnostic performance of Mc4-TSAb and M22-TRAb in GD and PT. The area under the ROC curve for the Mc4-TSAb showed no significant difference from the area of M22-TRAb (0.9742±0.0088 [area under the curve (AUC)±standard error (SE)] vs. 0.9874±0.0026 [AUC±SE]), The result also indicated there was no significant difference in assay performance between Mc4-TSAb and M22-TRAb (Fig. 1).
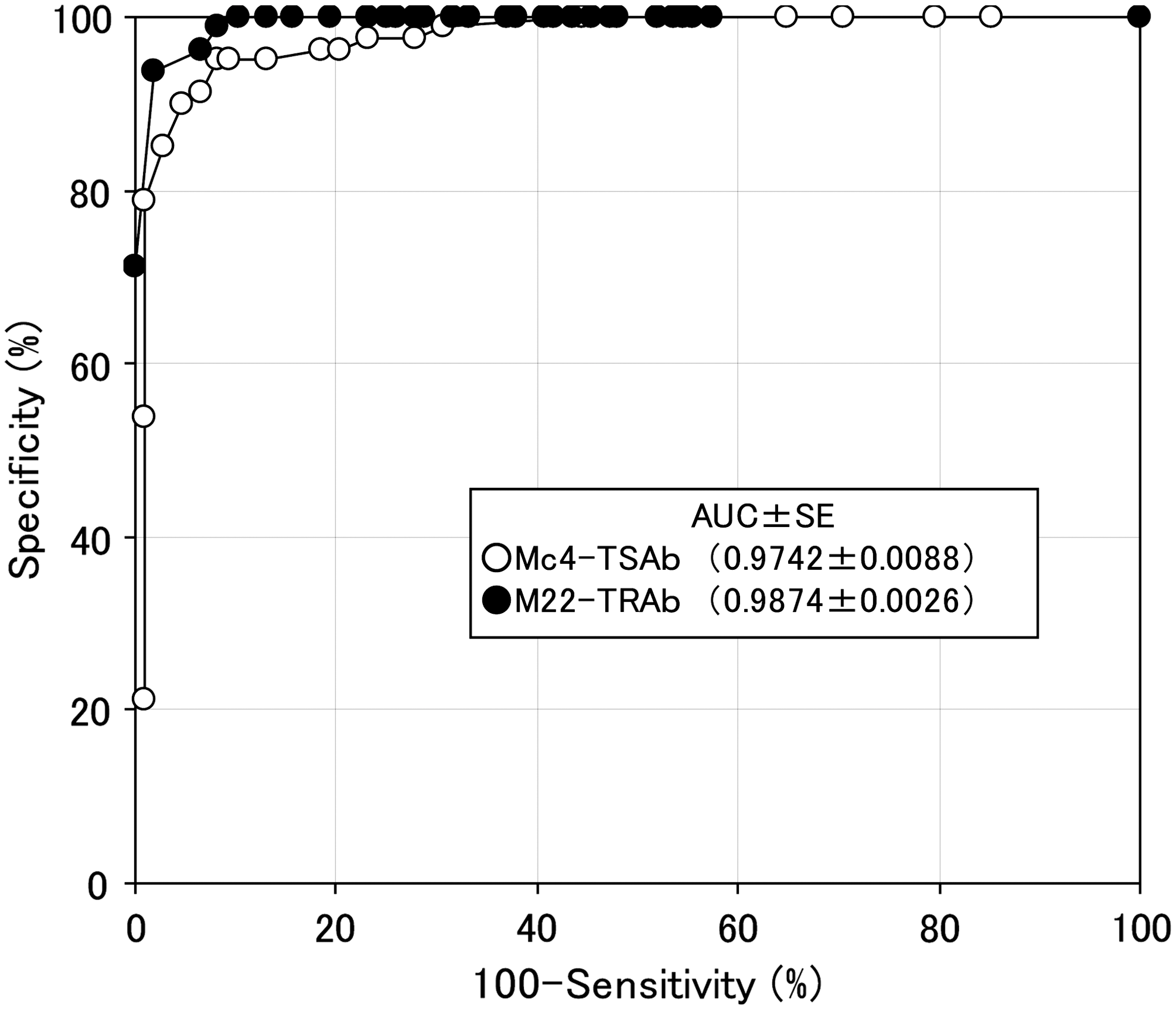
Comparison of the ROC analysis with Mc4-TSAb and M22-TRAb. The area under the ROC curve for the Mc4-TSAb using untreated Graves' disease (n=108) and painless thyroiditis (n=80) was 0.9742±0.0088 (AUC±SE), and the area of M22-TRAb was 0.9874±0.0026 (AUC±SE). There was no significant difference from those areas, thus indicating that there was no significant difference in assay performance between Mc4-TSAb and M22-TRAb. ROC, receiver operating characteristic; AUC, area under the curve; SE, standard error.
There was no significant difference in the positive rates in patients with untreated GD between Mc4-TSAb and M22-TRAb assays. In addition, for PT, the negative rate of Mc4-TSAb was not significant compared with the M22-TRAb. Overall, there was no clinical significant difference in the accuracy of GD and PT diagnosis between Mc4-TSAb and M22-TRAb.
GD, Graves' disease; PT, painless thyroiditis.
Discordant findings between both assays in untreated GD
Although neither the sensitivity nor specificity of Mc4-TSAb was significantly different from that of M22-TRAb, we observed that 6 Mc4-TSAb positive patients of 106 untreated GD patients (5.75%) were also M22-TRAb negative. In contrast, four of 106 patients (3.8%) who were M22-TRAb positive for untreated GD were also Mc4-TSAb negative. Only two of 106 patients (1.9%) with untreated GD were negative for both Mc4-TSAb and M22-TRAb (Table 2).
Two of 106 patients (1.9%) were negative for both Mc4-TSAb and M22-TRAb. Six cases of 106 (5.7%) were Mc4-TSAb positive and M22-TRAb negative. In contrast, four cases of (3.8%) were M22-TRAb positive and Mc4-TSAb negative.
TPOAb, thyroid peroxidase antibody; TgAb, thyroglobulin antibody.
Comparison of Mc4-TSAb and M22-TRAb in sera including TSBAb
In eight hypothyroid patients with a previous history of MMI treatment for GD, M22-TRAb levels in the binding assay were markedly elevated ranging from 22.9 to 193.5 IU/L. In contrast, the Mc4-TSAb levels in those patients were all less than the cut-off values (Table 3).
Mc4-TSAb and M22-TRAb levels in sera from eight patients with GD who spontaneously developed hypothyroidism after treatment with antithyroid drugs that was caused by the presence of TSHR blocking activity. Mc4-TSAb levels in all cases were lower than the cut-off values, although M22-TRAb showed high values.
L-T4, levo-thyroxine; MMI, methimazole; TBAb, thyroid blocking autoantibodies; FT4, free thyroxine; FT3, free triiodothyronine; TSH, thyroid-stimulating hormone; TSHR, TSH receptor.
Discussion
This study demonstrated a similar clinical performance of an FDA cleared, novel chimeric TSHR bioassay with an automated anti-TSHR binding inhibiting assay by using the recently isolated monoclonal autoantibody M22. We compared two distinct detection methods for TSHRAb by using sera from patients with untreated GD or PT. One was the Mc4-TSAb assay, which detects the signal of cAMP production through Mc4 chimeric TSHR binding with TSHRAbs in a patient's serum. The other was the M22-TRAb assay, which detects the inhibition rate of the M22 monoclonal antibody bound to the wild-type TSHR by TSHRAb in a patient's serum. Sensitivity and specificity were comparable in two large groups of patients with autoimmune thyroid disease, thus showing the usefulness of both tests in the diagnosis of GD. All in all, no significant or major differences in the sensitivity and specificity were noted for differentiating untreated GD from PT between Mc4-TSAb and M22-TRAb. Using comparative ROC analysis, we also confirmed that there was no significant difference in assay performance between Mc4-TSAb and M22-TRAb.
Discordant findings were registered in 10 of 106 sera of patients with untreated GD; and in six cases, the patients were positive for the bioassay but negative for the binding assay. This is in line with a recent observation (13) that all 11 subjects with positive bioassay results but negative binding findings had Graves' extrathyroidal disease, for example, orbitopathy, dermopathy, and acropachy; whereas those seven patients whose bioassay was negative but binding assay was positive had Graves' thyroidal disease only, were euthyroid, and were not smokers. These recent observations point to the fact that thyroid-stimulating immunoglobulins (TSI) detected and measured by the chimeric TSHR bioassay are functional biomarkers for the extrathyroidal and/or systemic involvement of GD. In line with this is a recent publication clearly demonstrating the clinical relevance of thyroid stimulating autoantibodies in Graves' eye disease (14). In this article evaluating 108 untreated cases of Graves' orbitopathy with various stages of clinical activity and clinical severity, TSI showed more significant association with clinical features of thyroid associated eye disease than the thyroid binding inhibiting immunoglobulins. Thus, with the help of the novel chimeric TSHR bioassay and in contrast to the anti TSHR binding assay, a clear differentiation of the character and functionality of the measured TSHR antibodies is possible.
Another explanation for the discordant findings is the binding of different autoantibodies to various TSHR epitopes. In addition, these data suggest that the combination of Mc4-TSAb assay and M22-TRAb assay could be effective in reducing the number of patients with GD who are TSHRAb seronegative, compared with the result obtained from only one method, Mc4-TSAb or M22-TRAb, because both Mc4-TSAb and M22-TRAb seronegative GD were found in only 2 (1.9%) of 106 patients with GD, whereas Mc4-TSAb seronegative GD was 5.7% in GD and 7.5%in the M22-TRAb method.
Since a previous study revealed that 75% of GD sera had TSBAb together with stimulating TSHRAb (15), we examined the influence of the TSBAb on Mc4-TSAb and M22-TRAb assays. Using TSBAb positive sera from eight patients who had been receiving ATD treatment for GD and subsequently developed hypothyroidism, it was confirmed that TSBAb had no influence on Mc4-TSAb but did explain the high positivity of the M22-TRAb assay. Thus, the Mc4-TSAb bioassay detects the stimulating type of TSHRAb without interacting with TSBAb, whereas the binding M22-TRAb assay cannot differentiate between TSBAb and stimulating TSHRAb. This may not be critical when using these assays as a diagnostic tool in untreated GD. However, this difference between the Mc4-TSAb and M22-TRAb assays may be important during monitoring ATD treatment, especially in circumstances in which a differential rate of decrease of TSBAb versus stimulating TSHRAb occurs during treatment.
Footnotes
Disclosure Statement
Hiroshi Murayama, Takahiro Uzu, and Kazuyoshi Togashi are employees of the Yamasa Corporation; Paul D. Olivo is an employee of DHI, and George J. Kahaly consults for DHI. The authors declare that no competing financial interests exist.