
Abstract
Background:
In a number of human malignancies, the presence of lymphocytic infiltration in or around tumor tissue is commonly considered to be part of the host tumor immune response. An association between thyroid carcinoma and chronic inflammation has been described. This relationship is not fully understood, so we performed a systematic study on a follicular variant of papillary thyroid carcinoma (FVPTC), to evaluate the type and distribution of certain immunological cells and their relationship with prognostic factors.
Methods:
We selected 91 consecutive cases of FVPTC, in which we evaluated the presence of three different immunological cells: dendritic cells (DC), immature CD1a+ and mature DC-Lamp+; mast cells (MC), tryptase+; and macrophages (M), CD68+, in the intratumoral, peritumoral, and extratumoral areas. As a control we analyzed 44 cases of thyroid adenomas (A).
Results:
In the intratumoral and peritumoral areas, the expression of CD1a, tryptase, and CD68 was significantly higher in FVPTC than in adenomas. Expression of CD1a and tryptase was comparable in the extratumoral compartment, whereas CD68 expression in the extratumoral area was significantly higher in FVPTC than in adenoma (p=0.0015). DC-Lamp expression was not significantly different among the intra-tumor, peri-tumor, and extra-tumor areas of FVPTC or adenoma. It was also very interesting that nonencapsulated FVPTC were more positive to tryptase.
Conclusion:
We highlight a higher presence of immunological cells in carcinomas than in adenomas. On this basis, it is possible to speculate that these inflammatory elements could be involved in tumor progression and invasion, as appears to be the case for MC and M.
Introduction
This diagnostic dilemma has very important therapeutic implications. Usually in PTCs, total thyroidectomy followed by radioactive iodine therapy is recommended. Some studies have suggested that patients with encapsulated FVPTCs have a better prognosis than those with un-encapsulated FVPTCs. However, there are few outcome data with long median follow-up from a large number of patients with FVPTC. Moreover, there have been very few studies in which tumor behavior was analyzed according to clinical and pathological features (4). Interestingly, among the several clinical and pathological parameters analyzed, few studies have considered inflammation and intratumoral fibrosis, which are significantly reduced in encapsulated tumors and play an important role in tumor development and progression. Alterations in the tumor stroma can be induced by chronic inflammation, and these changes can lead to enhanced tumor cell proliferation and metastasis and further genetic instability (5,6).
Epidemiological studies have demonstrated that chronic inflammation leads to a predisposition to certain cancers. The causes of chronic inflammation that increased cancer risk include microbial infections (e.g., Helicobacter pylori for gastric cancer and mucosal lymphoma, Hepatitis B or C, human papillomavirus, and EBV), autoimmune diseases (e.g., inflammatory bowel disease for colon cancer), cryptogenic inflammatory conditions (e.g., prostatitis for prostate cancer), and physical or irritants agents (e.g., solar exposure, tobacco smoke, and asbestos fibers).
The relationship between thyroid cancer and chronic inflammation is the subject of debate—in particular, inflammation associated with autoimmune diseases (e.g., Hashimoto's thyroiditis). Some authors agree that lymphocytic infiltration represents a form of immune reaction to control tumor growth and proliferation (7,8), whereas others have suggested that thyroiditis may be a precursor of thyroid carcinoma (9,10).
In this study we evaluated the presence of three different immunological cells: dendritic cells (DC), mast cells (MCs), and macrophage (M).
DCs, immature (CD1a+) and mature (DC-Lamp+), represent a complex system of antigen-presenting cells that play key roles in antitumor immunity and actively participate in the generation of tumor-specific effector T cells (11,12). Immature CD1a+ DC and mature DC-Lamp+ DC are widespread in most tumoral tissues and they are reported to be associated with improved prognosis (13,14).
MCs (Tryptase+) are residents of normal connective tissue and have been widely discussed for their role as tumor promoters during in tumor pathogenesis (15,16).
Finally, we analyzed the expression of macrophages (CD68+), which have been extensively described as inflammatory components of the microenvironment. However, under certain conditions, CD68+ macrophages can kill tumor cells; on the other hand, several investigations have highlighted their potential role as tumor promoters (17,18).
Materials and Methods
Patients
We analyzed 91 consecutive cases of FVPTC, treated by total thyroidectomy from January 2006 to January 2007 at the Department of Surgery, University of Pisa, Italy. As a control we selected 44 cases of thyroid adenomas, defined as consecutive cases with a solitary nodule, that underwent surgery during the same period of time. All the histological diagnosis were independently reviewed by two pathologists (A.P. and C.U.). Clinical and pathological parameters were available for all patients (Table 1).
FVPTC, follicular variant of papillary thyroid carcinoma.
Tumor samples from patients treated with total thyroidectomy were formalin-fixed, paraffin-embedded, and stained using hematoxylin and eosin. Normal thyroid tissue far (>1 cm) from the neoplastic nodule of the same lobe or, when possible, the normal thyroid tissue of the controlateral lobe was used as a control. We excluded cases of chronic lymphocytic thyroiditis from our study groups, since the coincidental presence of even a minor inflammatory component can greatly alter the results.
Immunohistochemistry
For each sample of tumor and nontumor tissue 2–4-μm-thick sections that were immediately adjacent to those used for histological diagnosis were studied by immunohistochemistry, with the streptavidin–peroxidase technique, using the automated Benchmark IHC staining system (Ventana Medical Systems, Tucson, AZ).
The following primary antibodies were used: anti-tryptase (1/1500 dilution; Chemicon International, Temecula, CA), anti-CD68 (1/100 dilution; Dako, Carpenteria, CA), anti-CD1a (prediluted; Ventana Medical Systems), and anti-DC-Lamp (DCs-human lysosome-associated membrane protein-3) (1/50 dilution; Immunotech, Marseille, France).
Evaluation of the immunohistochemical results
We assessed the immunohistochemical expression of tryptase, CD68, CD1a, and DC-Lamp using a semiquantitative method (Negative: 0–10 positive cells; Weak: 10–25 positive cells; Strong: ≥26 positive cells). The number of positive cells for each of the three sites (intratumoral, peritumoral, and extratumoral) was determined using two fields at 40× magnification and the mean value of the two areas was calculated. We evaluated the presence and the number of positive cells in the intratumoral and peritumoral site (immediately adjacent to the tumor front of invasion or to the tumor capsule, if present) and as a control in the extratumoral sites (in the controlateral lobe where possible).
Evaluation of the immunohistochemical staining was performed independently by two of the authors (A.P. and C.U.), and contrasting results were discussed until an agreement was reached. In both the intratumoral and peritumoral sites, cells with strong or weak staining were considered together to be positive, whereas cells without any staining were considered to be negative.
Positive strong or weak expression in extratumoral site was used as a control and was not considered in our statistical analysis.
Statistical analysis
Data were analyzed using both univariate and multivariate tests (STATISTICA Software, Stat Soft, Tulsa, OK). A p-value of <0.05 denoted the presence of a significant difference.
Results
Clinical and pathological parameters of FVPTCs and adenomas
Clinical and pathological parameters of FVPTCs and the control group (adenomas) are summarized in Table 1. No differences in age, tumor size, or gender were observed between the two groups. Among the FVPTCs, 49 out of 91 (54%) were encapsulated FVPTCs. Among the nonencapsulated tumors, 26 out of 42 (62%) were confined to the thyroid, whereas 16 (38%) extended outside the gland. Lymph node metastases were present in eight cases (9%).
CD1a, tryptase DC-Lamp and CD68 expression in FVPTCs and adenomas
In Table 2, we report the expression and distribution of each of the study markers in FVPTCs and adenomas. In the intratumoral area expression of immature DCs was positive in 46% of FVPTC and only in 3% of adenomas, which was highly significant (p=0.00001). MCs tryptase+ carcinomas in the intratumoral area were 41% versus 14% of positive adenomas (p=0.0011). Moreover, macrophages were significantly higher in FVPTCs (68%) than in adenomas (14%) with a strong significance (p=0.00001). No difference in mature DCs expression was observed between carcinomas and adenomas. Similar results were obtained by evaluating the peritumoral zone. Immature DCs, CD1a+, were positively observed in 21% of FVPTC and in 3% of adenomas (p=0.0023). MCs, Tryptase+, expression was higher in carcinomas than in adenomas, 13% versus 11% (p=0.046); and CD68 expression was significantly stronger in FVPTCs than in the control group (41% vs. 11%, p=0.015 respectively). When tissue outside the tumor (extratumoral site) was investigated, no differences were observed between carcinomas and adenomas for immature DCs (CD1a+) and MCs (Tryptase+), whereas expression of M (CD68+) was significantly higher in FVPTC (22% vs. 3%, p=0.0015).
Neg (Negative): 0–10 positive cells.
Negative (for tryptase only): 0–20 positive cells.
Positive: Weak: 1–25 positive cells and Strong: ≥26 positive cells; 21–50 positive cells (for tryptase only).
The number of positive cells for each of the three sites (intratumoral, peritumoral, and extratumoral) was determined using two fields at 40× magnification, and the mean value of the two areas was calculated.
p-value <0.05 denoted the presence of a significant difference.
CD1a: immature DCs marker.
Tryptase: mast cells marker.
DC-Lamp: mature DCs marker.
CD68: macrophages marker.
IT, intratumoral area; PT, peritumoral area; ET, extratumoral area; DC, dendritic cell; n.s., not significant.
Mature DCs (DC-Lamp+) expression was not significantly different in the intratumoral, peritumoral, and extratumoral areas.
Correlation between immunological markers and clinical and pathological features
In Table 3, we report statistical correlations between expression of the immunological markers and the clinical and pathological features in FVPTCs. Some of these parameters, such as tumor size, extrathyroidal invasion multifocality, and presence of node metastases, did not correlate with any of the evaluated markers. However, DC-Lamp expression was positively associated with female sex (p=0.0562), whereas CD1a and DC-Lamp were strongly associated with age (p=0.03, p=0.025, respectively). In both cases, older patients tended to exhibit stronger expression patterns. Tryptase expression was statistically correlated to the absence of a tumor capsule (p=0.0278). In fact, the majority (58%) of nonencapsulated FVPTCs expressed Tryptase-positive MCs.
Discussion
Numerous studies have reported the presence of lymphocytic infiltrate in thyroid carcinomas. Nevertheless, the role of such infiltrate is not completely clear.
The presence of lymphocytic infiltrate is more frequent in patients with PTC than in those with nodular goiter, suggesting that the inflammatory component supports tumor development (19). However, there are different opinions about the role of inflammation in thyroid cancer. Some authors have shown an increased incidence of thyroiditis in papillary carcinomas, whereas others have shown that tumors with intense infiltrate exhibit a lower frequency of recurrence and distant metastasis (20). In addition, poorly differentiated and anaplastic carcinomas are characterized by a significant decrease in inflammatory infiltrate compared to PTCs, confirming the protective role of the lymphocytic infiltrate (21). Macrophages, DCs, and MCs are frequently observed in PTCs (22).
DCs are a group of large nonlymphoid, class II MHC-positive mononuclear cells that appear to act as accessory cells in the immune response. Mature DCs are, in fact, the most effective at priming tumor-specific T-cells (23). Recent investigations, carried out using immunohistochemical methods, revealed that dense infiltration by DC immature cells, recognized by CD1a antigen, correlated with favorable prognosis in several types of cancer, including thyroid papillary carcinoma (24), suggesting that these cells play a critical role as antigen-presenting cells in the T cell-mediated antitumor response.
In the present study, we found a significant difference between FVPTCs and follicular adenomas regarding CD1a-positive immature DC expression in both the intratumoral and peritumoral areas (Figs. 1A and 2A).
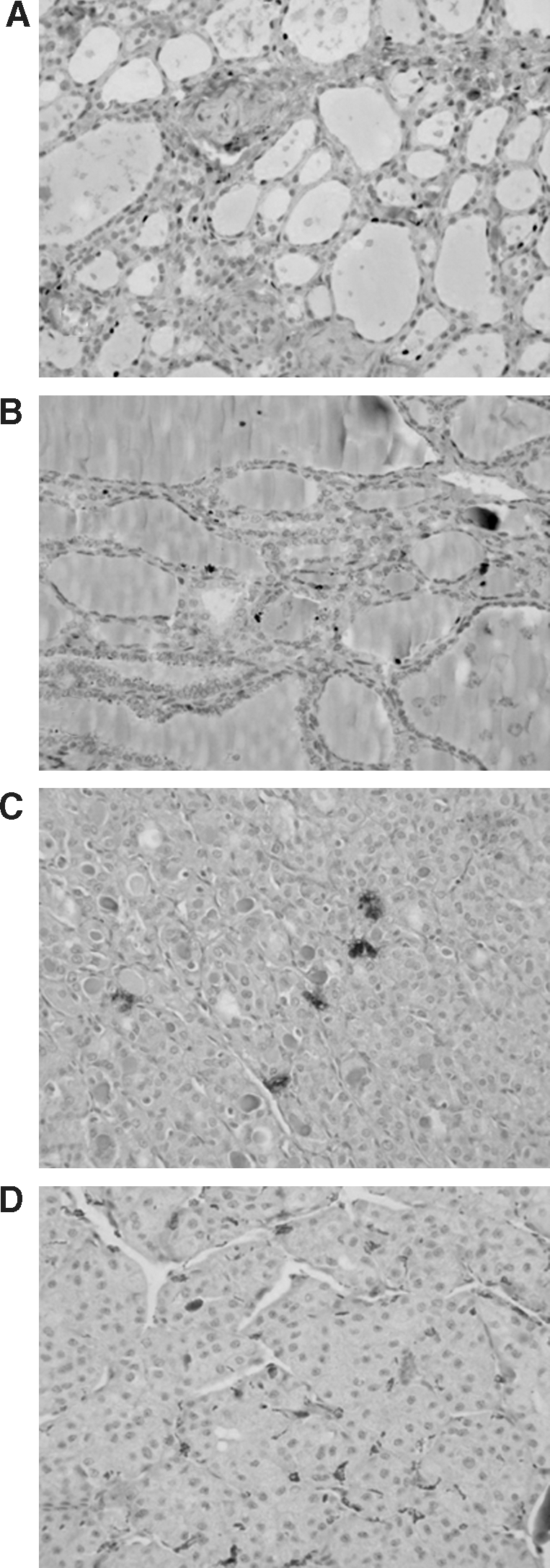
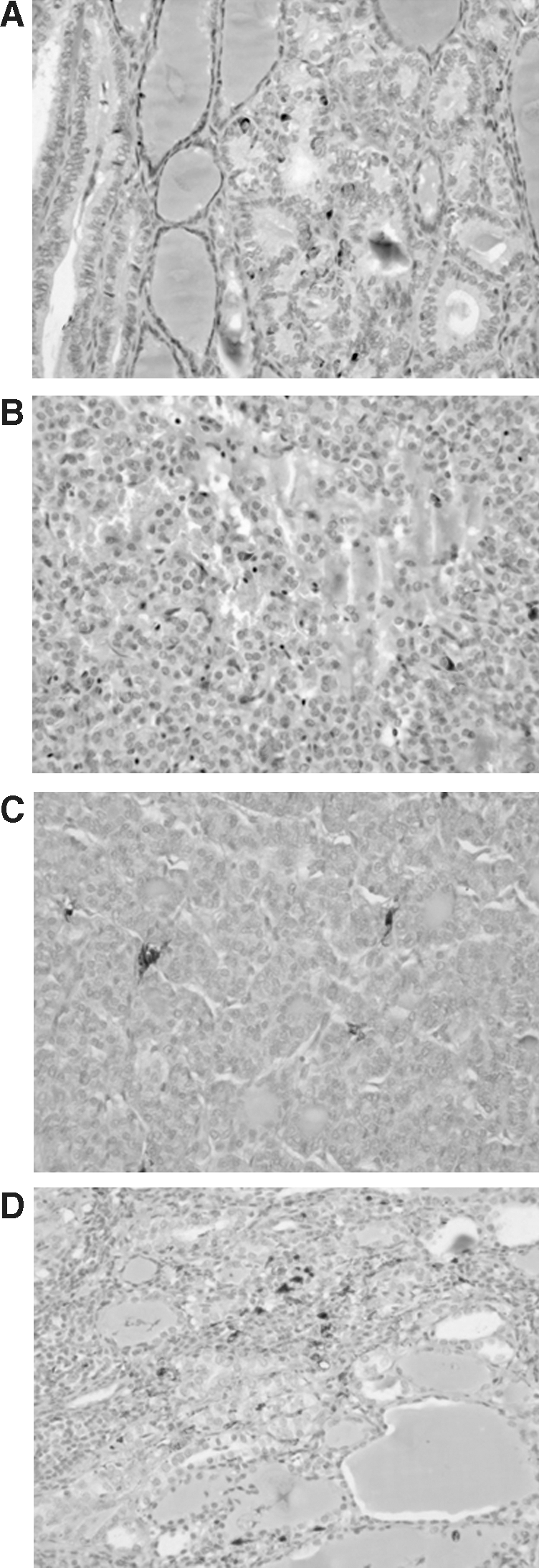
Specifically, the density of CD1a+ DCs was higher in FVPTCs than in adenomas. On the other hand, no difference was observed for DC-Lamp+ mature DCs in all compartments (Figs. 1B and 2B). These data partially support the observation by Bell et al. (25) that CD1a+ DCs in the tumor microenvironment appear higher than in normal breast epithelia, suggesting increased homing and infiltration. DC-Lamp+ DC were mainly located in the peritumoral area. They speculated that stromal factors may determine DC adherence and maturation. We cannot completely support these observations, but we could propose the important role for DCs in the development of tumor immunity.
We also evaluated the presence and distribution of MCs (Tryptase+) in FVPTCs and follicular adenomas (Figs. 1C and 2C). Interestingly, they were significantly highly expressed in the peritumoral compartment of FVPTCs.
Considering only the FVPTC group there was also a significant correlation between the abundance of MCs and the infiltrative pattern of the tumor. These data are in agreement with Acikalin et al., who suggested a pro-tumoral role for MCs based on the tight association between these cells and the promotion of microangiogenesis in tumor tissues (12,26). Even so, other authors have proposed a protective role of these immunological elements. Sinnamon et al. (27) examined the role of MCs in intestinal tumorigenesis and noticed an induction of apoptosis in MC-rich tumors, suggesting an anti-tumoral role of MCs.
Some studies have been conducted on MCs in thyroid carcinomas. MC infiltration positively correlated with growth, multifocality, and invasive ability of PTCs (28). Although in several cancer types, MC infiltration correlates with increased angiogenesis (29,30), our data could support a role for MC in thyroid cancer invasive capacity. How MCs are activated in our model system is currently unknown and will be the object of further investigation. Melillo et al. suggested that MCs are recruited into thyroid carcinoma where they induce tumor growth and invasiveness through MC-derived mediators, including histamine and chemokines, such as CXCL1/GROα and CXCL10/IP10 (28). Whatever the case, our results could support the finding that MC infiltration promotes proliferation and PTC invasiveness. These results are consistent with those reported by Gounaris and colleagues. In their mouse model of adenomatous polyposis coli MC ablation reduced the frequency and size of polyps through decreases in blood vessel density and mitotic activity and an increase in apoptosis. Taken together, these data suggest that MCs are necessary for most of the hallmarks of polyp formation (31). In our study, the higher presence of these immunomodulating cells in the peritumoral compartment of nonencapsulated FVPTCs could suggests a role for these cells in promoting tumor invasiveness. However, FVPTCs are not highly aggressive neoplasms, so it could be very interesting to study the relationship between MC abundance and prognosis in more aggressive thyroid tumors, such as classic and tall cell variants of PTC or poorly differentiated carcinomas.
These data seem to confirm that tryptase-positive MCs are involved in tumor progression, as largely discussed in the literature (28,32,33).
Finally, in the same two groups of FVPTCs and thyroid adenomas, we evaluated the presence and distribution of CD68+ macrophages (Figs. 1D and 2D). An association between these cells and solid tumors, including breast, colorectal, prostate, and lung cancer, as well as gliomas and bladder neoplasms, has been reported. Although macrophages can kill tumor cells under certain conditions, several investigation have highlighted their potential role as tumor promoters that act by secreting factors that can directly stimulate the growth and migration of tumor cells, angiogenesis and lymphoangiogenesis-promoting factors, and proteases that facilitate tumor invasion and metastases (20,30). In thyroid cancer, the role of tumor associated-macrophages (TAMs) was studied by Fagin and colleagues (34) in a series of well-differentiated, poorly differentiated and anaplastic carcinomas. The presence and density of TAMs correlated with clinical and pathological parameters. It appeared that the density of TAMs was higher in advanced thyroid cancers and was related to invasion and decreased survival. These data support the role of Ms as tumor-promoting cells (34). A prevalent distribution of CD68+ cells in the stroma and, in particular, along the tumor front has also been reported (20). These association has partially been confirmed by our data. We found a significant difference in the abundance and distribution of the inflammatory cell infiltration in intratumoral and peritumoral areas of papillary tumors although there was no association with prognostic factors. These data support a pro-tumoral role of Ms, and we can speculate the importance of a wide analysis of M presence in more aggressive thyroid neoplasm.
In conclusion, we can assert that there are major differences between FVPTCs and adenomas regarding the distribution of inflammatory infiltrate. We highlighted a higher presence of immunological cells in carcinomas than in adenomas. Further, these cells were mostly distributed in intratumoral and peritumoral areas. On this basis, we can speculate that these inflammatory elements could be involved in tumor progression and invasion, as in case of MCs and Ms. The extratumoral inflammatory infiltrate was equally distributed in FVPTCs and adenomas; in these groups it was significantly associated with clinical and pathological parameters.
These findings could be the first step toward a thorough analysis of the role of immunological cells in more aggressive thyroid neoplasms, such as poorly differentiated carcinomas and tall cell or classical variants of papillary carcinoma.
Footnotes
Acknowledgments
This study has been supported in parts by grants from Ministero dell'Istruzione, dell'Università e della Ricerca, Associazione Italiana per la Ricerca sul Cancro, Istituto Toscano Tumori, and Ministero della Salute.
Disclosure Statement
The authors declare that no competing financial interests exist.