
Abstract
Background:
Papillary carcinomas with diameters that are less than or equal to 1 cm (thyroid papillary microcarcinoma [mPTC]) are quite common but can carry more risk than previously thought. The proper treatment and management of these lesions is still being debated. Even though fine needle aspiration cytology (FNAC) is considered the best method for the diagnosis of thyroid nodules, its efficacy is still questioned for mPTC. We investigated the role of BRAF gene status in preoperative cytological samples, using manual macrodissection as an additional tool to improve the diagnostic accuracy of mPTC.
Methods
Results:
In this study, we showed that the BRAF V600E mutation was present with a high frequency in patients with mPTC (74%). The presence of the mutation was independent of the size of the tumor. In our study, the combination of the cytological diagnosis and the molecular analysis was able to identify 82% of all cases of mPTC, with an increase of 37% compared with a morphological diagnosis alone. The morpho-molecular analysis was able to reduce the number of suspicious cases by >70%. All of the goiters had a wild-type BRAF status.
Conclusions:
The analysis of BRAF mutational status in FNAC obtained from papillary microcarcinomas demonstrates that molecular pathology, combined with morphology and molecular biology is a powerful tool for cytological diagnosis of mPTC. Our results also confirm the data supporting the biological relevance of PTCs with diameters that are ≤1 cm and the importance of “manual macrodissection” in the molecular analysis of cytological material.
Introduction
Similar data from a 2004 report of the French Thyroid Cancer Committee (3) described a doubling of cases of mPTC from 1983 to 1987 (∼18%) to 1998–2001 (∼43%). A study from the United States comparing rates of PTC from 1973 to 2002 reported an approximately threefold increase in PTC, with almost 50% of this increase consisting of tumors with diameters that were ≤1 cm (4).
The nature and clinical relevance of mPTC is still questioned (5,6). Several lines of evidence strongly support the hypothesis that mPTC not only represents an early phase of PTC, but also progresses quickly toward the acquisition of a metastatic genotype/phenotype. As a matter of fact, mPTC is often multifocal and, in a significant number of cases, is associated with extracapsular invasion and either nodal or distant metastasis (7,8). Moreover, the BRAF V600E mutation is detected in about 18% of incidental cases of mPTC and in 40% of preoperatively identified cases of mPTC (9). The BRAF gene is one of the three isoforms of the RAF family. It is a serine/threonine kinase, located downstream of rat sarcoma (RAS) and upstream of the mitogen-activated protein kinase (MAPK) cascade (10). In PTC, including all of its variants, the BRAF gene is mutated at a rate of up to 70% (11 –13). V600E is the most commonly detected mutation, leading to a thymine-adenine transversion at nucleotide 1799 (T1799A) in exon 15. At the protein level, the valine at position 600 is substituted with glutamic acid (10). In cases of PTC, the BRAF V600E mutation results in an increase in invasiveness and both local and distant metastasis, in addition to a decrease in survival (14). Notably, mutated cases can be refractory to radioiodine therapy (13,15). The evaluation of BRAF status is currently considered important to the assessment of the prognosis and management of PTCs (16,17).
Recently, the strong prognostic value of mutations in the BRAF gene was also demonstrated for cases of mPTC (18). The need for better preoperative characterization of mPTCs and the absence of studies focused on BRAF analysis by manual macrodissection in FNAC obtained from mPTCs encouraged us to verify the feasibility of a molecular approach to this variant of lesion in preoperative cytological material. Our laboratory recently proposed a simple and robust method to perform BRAF molecular analysis on cells obtained by FNAC of thyroid nodules (19). To our knowledge, this article is the first on the evaluation of the BRAF V600E mutation using manual macrodissection in samples obtained from FNAC of mPTCs.
Materials and Methods
Patients
The study group consisted of 95 patients (80 females and 15 males) each of whom underwent a total thyroidectomy. The mean age was 41 yrs (range, 19–67 years) for men and 35 years (range, 15–47 years) for women. According to guidelines for the management of thyroid cancer in adults, all patients falling within the cytological Thy3, Thy4, and Thy5 diagnostic categories underwent surgery (i.e., Thy3: all follicular indeterminate lesions; Thy4: abnormal, suspicious for malignancy; Thy5: diagnostic for malignancy; according to the Guidelines for the Management of Thyroid Cancer in Adults, March 2002) (20).
Thyroid nodules
Eighty-five cases were mPTC, that is, PTC with diameters that were ≤1 cm, and 10 cases were goiters. All mPTCs were the classical type. The nodules were preoperatively evaluated using ultrasonography according to the Medical Guidelines for Clinical Practice for the Diagnosis and Management of Thyroid Nodules of the American Association of Clinical Endocrinologists and the Associazione Medici Endocrinologi (21,22). FNAC was performed when the nodule showed at least three of the following features: intranodular microcalcifications, hypoechoic structure, increased vascularity, and infiltrative margins. Only one additional suspicious characteristic was required when microcalcifications were present. In all cases, FNAC was performed after clear ultrasound documentation of the presence of the needle tip inside the nodule, as shown in Figure 1.
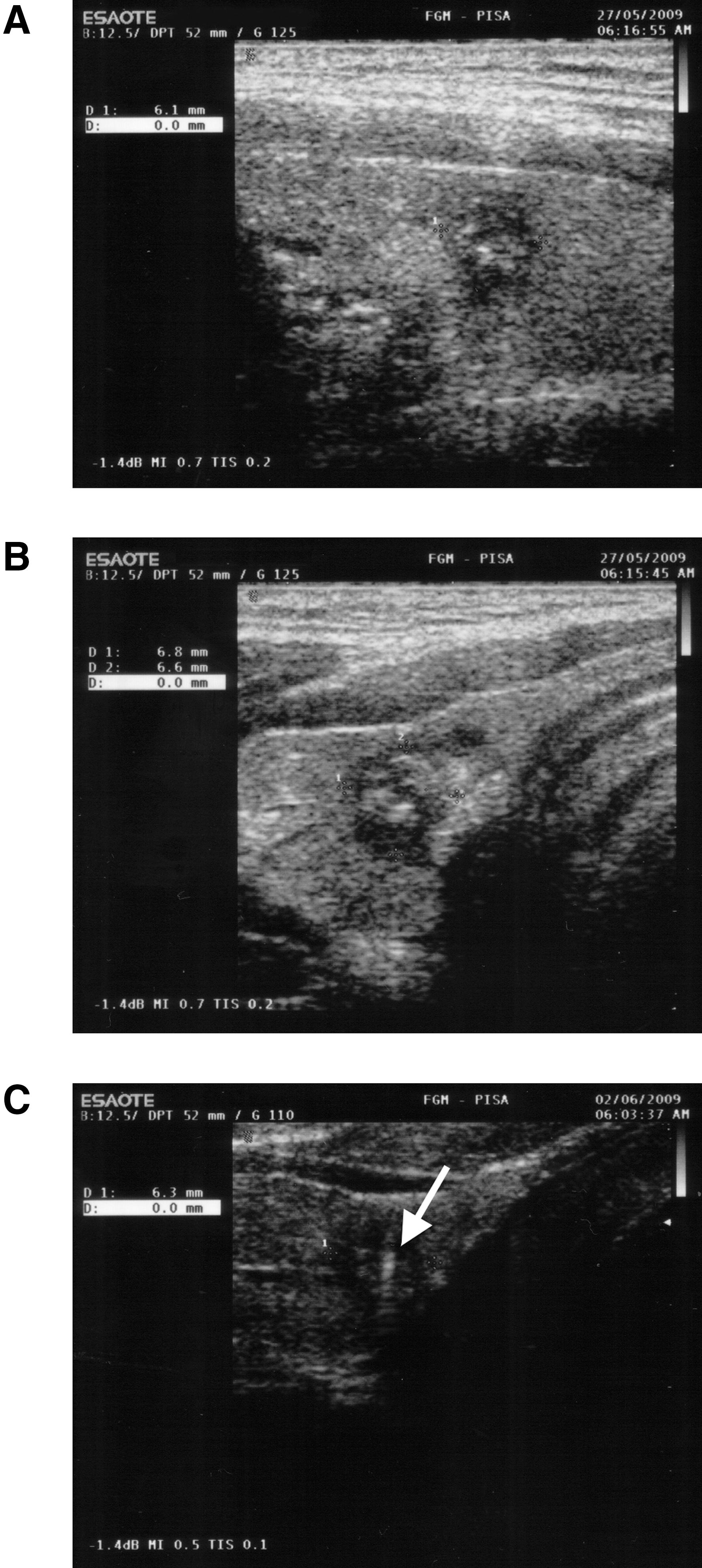
Ultrasound imaging of a suspicious thyroid lesion of ∼0.6 cm in diameter in a 26-year-old male:
Fine needle aspiration cytology
Cytological material was obtained by fine needle aspiration performed with ultrasonographic guidance. The slides were fixed in ethyl alcohol for Papanicolaou staining. The cytological diagnosis was based on the universally accepted microscopic criteria, including cell background, cell arrangement, cell shape, nuclear features, presence of nucleoli, and presence of mitosis (Fig. 2).
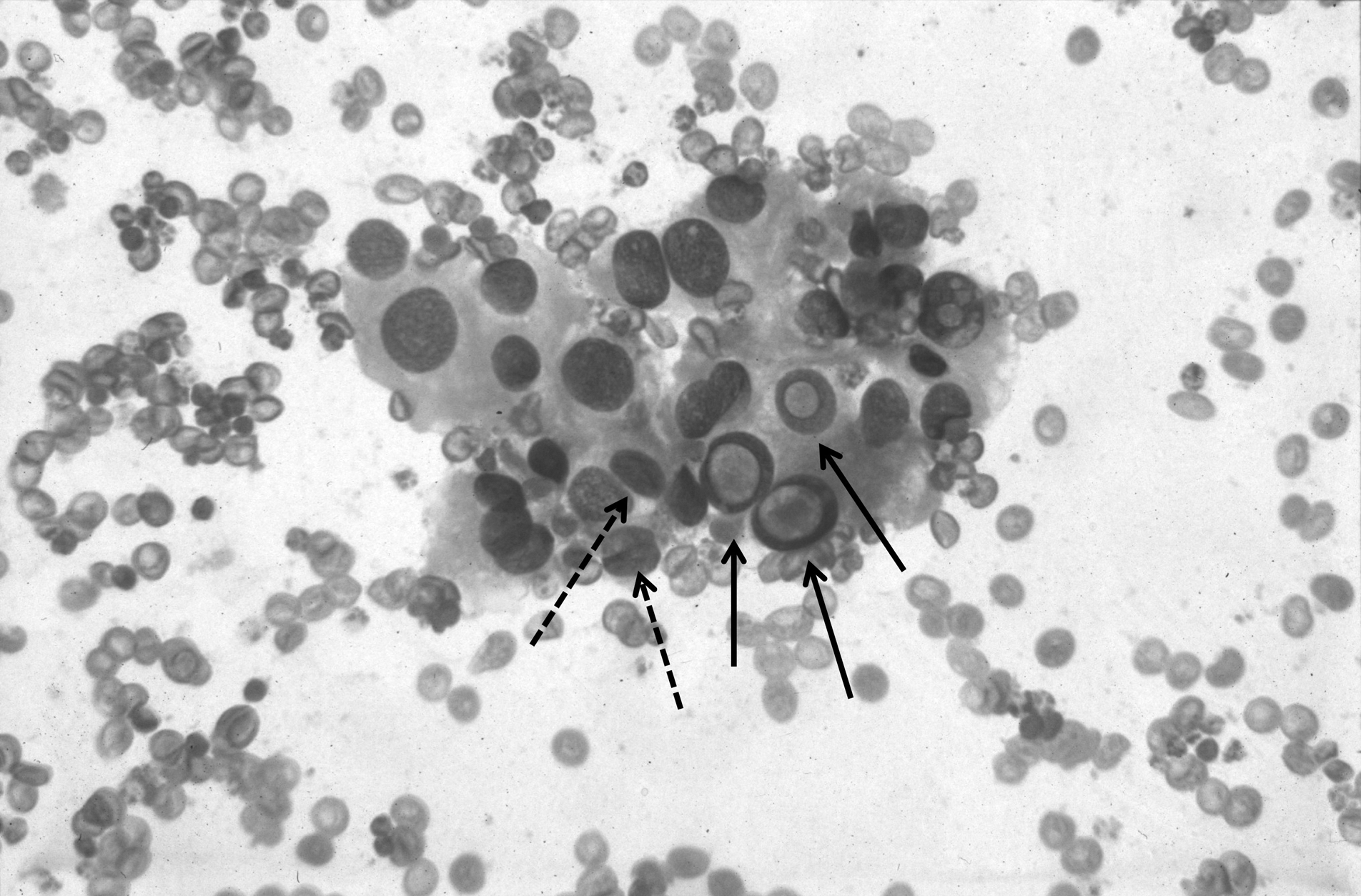
Papillary thyroid carcinoma, same case as Figure 1: the aspirate smear shows neoplastic cells with prominent intranuclear pseudoinclusions (solid arrows) and grooves (dotted arrows; 400×, Papanicolaou stain).
Manual macrodissection of the slides
The methodology chosen for the molecular study has been previously described (19) and is used in our laboratory on a routine basis. The term “manual macrodissection” indicates that tumor cells or suspicious cells are first identified and then selected by the cytopathologist at the microscope from Papanicolaou-stained smears to assure adequate thyroid cell representation and to confirm the cytological diagnosis (Fig. 3). After choosing the most representative slides or after marking the regions of the slide containing numerous lesional thyrocytes, the FNAC slides were kept in xylene for 1 to 3 days until the coverslips detached from the slides. The slides were then hydrated in a graded series of ethanol baths, followed by a wash in dH2O for one minute. The slides were finally air dried, and DNA extraction was performed using a commercially available kit (Nucleospin; Macherey-Nagel) with a modification to the first step. Fifty percent of the lysis solution without proteinase K was initially poured on the slide to scrape off the cytologically stained sample using a single edged razor blade. Any scraped tissue was then collected in a microcentrifuge tube containing the other half of the lysis solution with proteinase K. The extracted DNA was kept at −20°C until used.
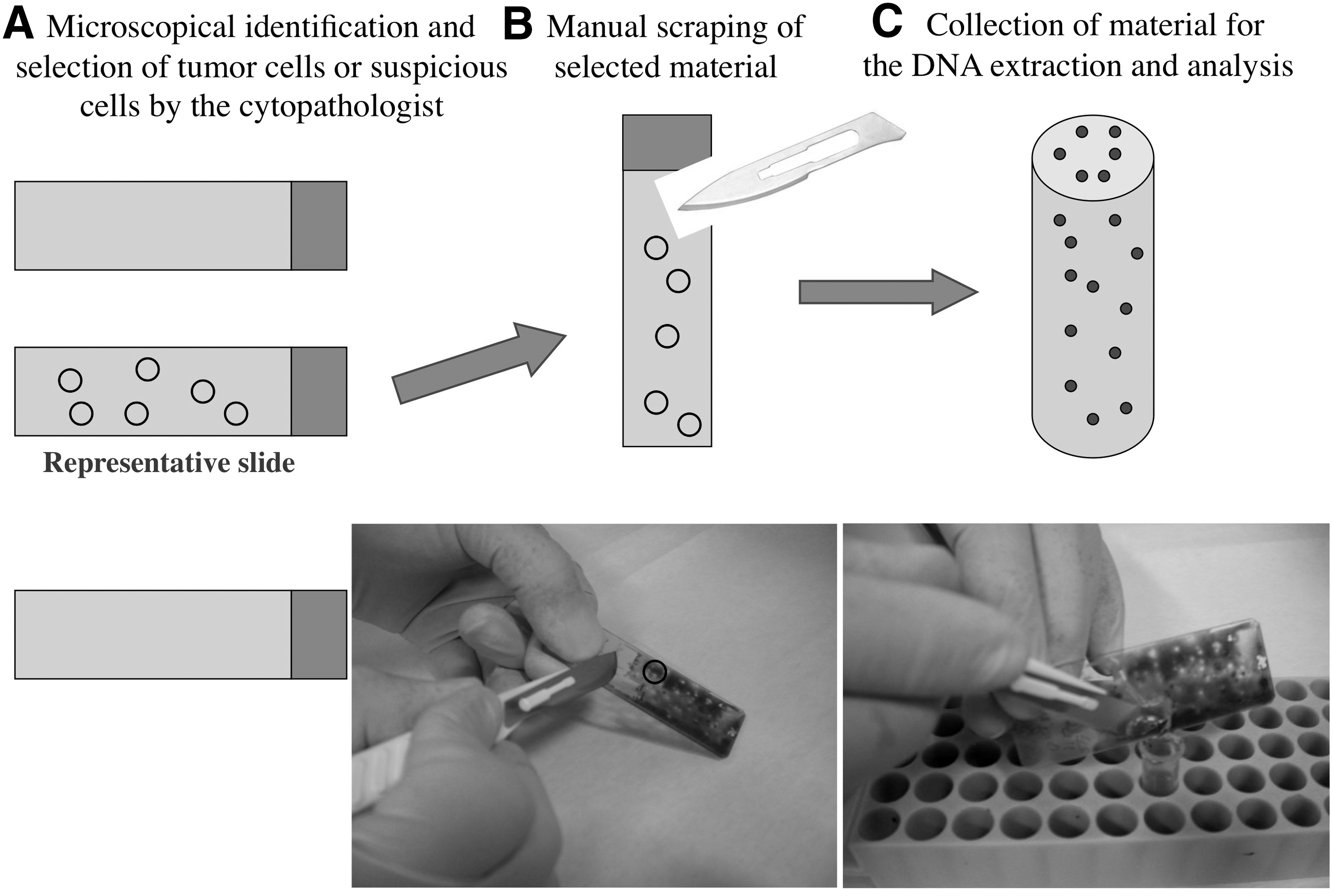
Manual macrodissection of a slide.
BRAFV600E sensitivity threshold strategy
To establish the sensitivity threshold of our mutation detection methodology, DNA extracted from a BRAFV600E homozygous human melanoma cell line was diluted with BRAF wild-type human DNA. Dilutions were made to obtain nucleic acid material mixtures made of 75%, 50%, 25%, and 10% tumor DNA. BRAF mutation analysis was performed on each series of dilutions. BRAF V600E was detectable down to a concentration of 25% tumor DNA. To be sure on the significance of the results, we adopted the criterion of using only slides in which the neoplastic cells represent no less than 50% of the entire cell population.
Detection of the BRAFV600E
The BRAF exon 15 was analyzed by polymerase chain reaction (PCR) followed by direct sequencing. The PCR was performed in a 30 μL final volume containing 2 μL of DNA, 0.05 mM dNTP (Invitrogen), 2.5 ng/μL of each primer (Invitrogen), 1.5 mM MgCl2, 1×PCR Gold buffer, and 0.75 U of AmpliTaq Gold (Applied Biosystems). The PCR reactions were performed on a 9700 GenAmp PCR System (Applera Corporation) with the following cycling conditions: initial denaturation at 94°C for 7 minutes; 40 cycles of 94°C for 45 seconds, 56°C for 45 seconds, and 72°C for 1 minute; a final step at 72°C for 10 minutes. The primers were F–TCATAATGCTTGCTCTGATAGGA and R–GGCCAAAAATTTAATCAGTGGA. The PCR products were run on an agarose gel to confirm the presence of the specific amplification products. PCR bands were cut and purified using a Genelute Gel Extraction Kit, and the purified products were then sequenced on an ABI PRISM 3100 Genetic Analyzer (Applied Biosystems).
We used positive controls known to carry BRAF V600E. The negative controls were benign tumors and NTC were PCR relations run without template.
Surgical pathology
Tumor size was measured during the macroscopic examination of the lobes. The diagnosis of PTC was made according to the standard histological criteria.
The validation of data for BRAF V600E in thyroid FNACs was performed by determining the sensitivity (number of true positives/[number of true positives+number of false negatives]), specificity (number of true negatives/[number of true negatives+number of false positive]), precision (number of true positives/[number of true positives+false positives]), and accuracy ([number of true positives+number of true negatives]/[number of true positives+false positives+false negatives+true negatives]). True positive and the true negative status was based on the histological diagnosis obtained from thyroidectomy specimens.
Results
Histological diagnosis
A diagnosis of mPTC was made in 85 out of 95 cases: 30 of the 85 cases had a tumor size smaller than 0.7 cm. Ten of the 95 cases were diagnosed as goiter.
Cytological diagnosis
In the 85 patients with a final diagnosis of mPTC, the cytological diagnosis was PTC in 38 cases (45%), suspicious for papillary carcinoma in 42 cases (49%), and indeterminate lesions in 5 cases (6%).
A definitive PTC diagnosis was obtained in 15 cases involving nodules that were <0.7 cm and in 23 cases involving nodules that were ≥0.7 cm. Suspicious for papillary carcinoma was diagnosed in 13 cases involving nodules that were <0.7 cm and in 29 cases involving nodules that were ≥0.7 cm. Indeterminate lesions were diagnosed in one case involving a nodule that was <0.7 cm and in four cases involving nodules that were ≥0.7 cm.
The final diagnosis for the remaining 10 patients was that of a nodular follicular goiter. The nodules were cytologically diagnosed as indeterminate lesions with a diameter of <0.7 cm in three cases and >0.7 cm in seven cases.
BRAF gene status
BRAF V600E was detected (Fig. 4) in the FNAC material from 63 of 85 (74%) mPTCs that were examined (63 cases). Mutations were found in 31 of the 38 cases with a cytological diagnosis of PTC (81.6%) and in 32 of the 42 cases with a cytological diagnosis of suspicious for papillary carcinoma (76%). All of the indeterminate lesions were wild type (Table 1).
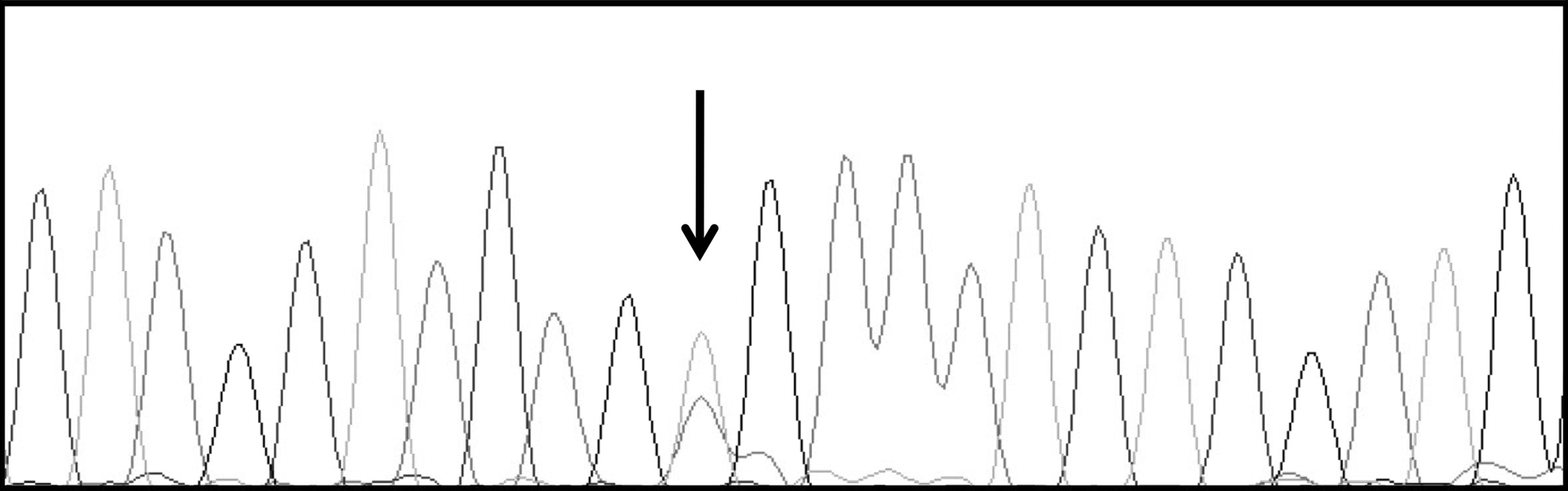
Direct sequencing of the BRAF exon 15 polymerase chain reaction product, same case shown in Figure 1: the BRAF V600E heterozygous mutation is represented by the two overlapping peaks (arrow).
Out of 85 cases.
Out of 42 cases.
PTC, papillary thyroid carcinoma; SPTC, suspicious PTC; MWA, indeterminate lesions (i.e., microfollicular proliferation without atypia).
The detection of the mutation was equally distributed according to the tumor size. Twenty-three of the 29 mPTCs were <0.7 cm (79%), and 40 of the 56 mPTCs were ≥0.7 cm (72%).
BRAF V600E was not detected in any of the 10 goiters; these were diagnosed as cytologically indeterminate lesions.
Molecular cytopathology of mPTC
BRAF V600E was present in 81.6% of the cases with a definitive cytological diagnosis of PTC and in 76% of the cases that were diagnosed as suspicious for papillary carcinoma. If we combine the 32 cases with BRAF V600E in the cytologically suspicious papillary carcinoma group with the group of cases with a definitive PTC cytological diagnosis, the number of cases with a definitive morpho-molecular diagnosis of PTC becomes 70 (82%), and the number of cases that were suspicious for papillary carcinoma cases decreases to 10 (12%). The test's sensitivity was 74% (confidence interval [CI] 63.48% to 83.01%), specificity 100% (CI 69.15% to 100.00%), precision 100% (CI 94.31% to 100.00%), and accuracy 77%.
The morpho-molecular approach is able to increase the percentage of diagnostic accuracy by 37%, from 45% to 82%. The 76% decrease in cases with a diagnosis of suspicious for papillary carcinoma is remarkable.
BRAF status and clinical features
All of the cases affected by mPTC were categorized as clinical stage I according to the Medical Guidelines for the diagnosis and management of thyroid nodules and differentiated thyroid cancer of the American Thyroid Association (22).
As shown in Table 2, multifocal disease was detected in 33/63 (52%), extrathyroidal invasion in 31/63 (49%) and metastases to the local lymph node in 28/63 (44%) of the mPTCs with BRAF V600E. In the 22 mPTCs that were negative for BRAF V600E, multifocal disease was detected in 5/22 (23%) of the cases, extrathyroidal invasion in 7/22 (35%) of the cases, and metastases to the lymph node in 5/22 (23%) of the cases. The χ 2 statistical analysis gave a p-value that was not significant (p=>0.05).
Discussion
Based on what other human cancer models, such as breast cancer and colorectal carcinoma, have taught us about cancer progression, at least a percentage of mPTC cases have to be considered to be an early stage of PTC. Consequently, detection of microcarcinomas represents a means of secondary prevention, that is, of early diagnosis.
The stage at which an infiltrative carcinoma develops an invasive/metastatic genotype/phenotype cannot be predicted simply on the basis of its size. How big must a nodule be to be considered dangerous? Moreover, the literature and clinical practice have numerous examples of cancers with a diameter of a few millimeters, but with a wide metastatic dissemination. The analysis of the molecular characteristics of the lesion can be helpful in characterizing its behavior.
This issue strongly applies to mPTC, which is often multifocal and associated with extracapsular invasion and metastasis (23).
The status of the BRAF gene is considered critical to the etiology and the pathogenesis of PTC. Consequently, its analysis is now considered a relevant diagnostic and prognostic tool. In addition, the relationship between BRAF gene mutational status and therapeutic strategy has been well studied (14).
Notably, data obtained from the analysis of the BRAF gene in mPTC strongly support the hypothesis that thyroid carcinomas of ≤1 cm in diameter are not harmless, occult, neoplastic foci. They are real infiltrative tumors that show clear metastatic behaviors (24,25).
Based on this information, the detection and the characterization of mPTC should be a goal of modern endocrinology.
Because of the lack of research on BRAF gene status assessment in samples obtained from FNAC of mPTC using manual macrodissection, we chose to focus on the preoperative molecular characterization of PTCs with diameters of ≤1 cm. We recently described a simple and robust method for the molecular analysis of cells indentified as neoplastic or suspicious during microscopic observation. These cells can be easily scraped from the slide and processed for DNA extraction and analysis. This “manual macrodissection” of selected slides or selected regions of a slide allows one to choose the correct cell population to be investigated. Moreover, additional aspirates need not be performed, which reduces the possibility of obtaining negative results due to low numbers of tumor cells or due to the presence of nonthyroid cells, such as lymphocytes and/or histiocytes. In this study, all of the smears were independently reviewed by a senior cytopathologist, to assure adequate thyroid cell representation and confirm the cytological diagnosis of the slides in which BRAF gene status was investigated.
There are several previously published reports on the BRAF gene in mPTC. However, these studies involved experiments conducted on paraffin-embedded tissues (18). Our group has recently published a study on BRAF and PTCs with diameters of >1 cm (19), in which we described the molecular approach that is now applied to mPTCs examined by FNAC for the first time. By using this new approach in the present study, we were able to increase by ∼37% the number of definitive diagnoses of mPTC that reached 82%. In fact, 32 of the cases were moved from the “suspicious” group to the “definitive PTC diagnosis” group. The combination of the classic morphological examination and the molecular analysis was able to reduce the number of cases that were suspicious for papillary carcinoma, by a noticeable percentage of >76% (Table 1). The potential usefulness of the new approach in clinical practice is also highlighted by the 100% specificity and precision of the detection of BRAF V600E in PTC in the present study, associated with a good sensitivity and accuracy values (i.e., 74% and 77%, respectively).
The percentage of cases with mutations (74%) in our study was higher than what has been reported previously. The percentage of PTCs with BRAF V600E varies from <20% to >80% (13). This wide range can be explained by considering that the different variants of PTC can develop through different molecular pathways and, consequently, have different BRAF gene statuses. All the microcarcinomas detected in the present study belonged to the classic type subgroup. Therefore, they represent a homogenous group that is characterized by a high incidence of BRAF V600E, reaching 70% (26). Moreover, the reliability of the laboratory has to be considered, as well as the methodology used. In particular, the fact that we selected the cells on which we performed the analysis by “manual macrodissection” has to be taken into consideration. From a clinical perspective, it is also important to emphasize that the BRAF mutation status of samples obtained from FNAC could be a good test for the potential aggressiveness of the tumor and may also be useful in the preoperative management of patients with mPTC, as the utility of BRAF mutation assessment in the management of PTC has clearly been demonstrated (24). In this context, our finding that mPTCs carrying BRAF V600E also show more aggressive behavior than mPTCs with wild-type BRAF (Table 2) confirms the potential clinical utility of BRAF testing for the identification of tumors that require more careful evaluation, regardless of size (18). The clinical strength of BRAF screening of samples obtained from FNAC is also supported by the finding that, in all the goiters with a cytological diagnosis of indeterminate lesion, the BRAF status was wild type. These results confirm the absolute specificity of BRAF V600E assessment in PTC diagnosis and are in agreement with previously reported data (14,17).
Notably, the percentage of cases with BRAF V600E does not vary according to the size; 79% of nodules were <0.7 cm in diameter and 72% of nodules were >0.7 cm in diameter. This information suggests that alterations in the BRAF gene are involved in the early phase of tumor growth (9).
Finally, PTCs with nodules of <1 cm in diameter that carry the BRAFV600E mutation show more aggressive behavior than mPTCs with wild-type BRAF (Table 2), as also been reported previously (18). The analysis of BRAF status in samples obtained during FNAC could be a useful tool for evaluating the aggressiveness in preoperative management of patients with mPTC (24).
In conclusion, this first study on the assessment of BRAF mutational status of samples obtained during FNAC of papillary microcarcinomas demonstrates that molecular pathology (combined morphology and molecular biology) is a powerful tool for the cytological diagnosis of mPTC. Our results also support the data concerning the aggressiveness of PTCs with nodules of ≤1 cm in diameter and confirm the important role of “manual macrodissection” in the molecular analysis of cytological material.
Footnotes
Autho Disclosure Statement
The authors declare that no competing financial interests exist.