
Abstract
Background:
In papillary thyroid carcinoma (PTC), recurrences during long-term follow-up (R-LTFU) occur even in those who appear to have an excellent prognosis after initial thyroid surgery and usually, radioactive iodine (i.e., “primary treatment”). Initial studies that predict R-LTFU are not well defined. Values for serum thyroglobulin (Tg) measurements when serum thyrotropin (TSH) is >30 μU/mL, as a result of either recombinant TSH or L-thyroxine withdrawal, referred to here as stimulated Tg (STg), have been previously evaluated. The aim of the current study was to determine the parameters associated with R-LTFU in patients with PTC categorized as having low-risk disease 9 to 12 months after their primary treatment.
Methods:
This was a retrospective study of 469 patients with PTC with a mean follow-up 5.8±3.9 years. Study patients had to have no uptake in the first postablative diagnostic 131iodine whole body scan (WBS) performed 9–12 months after primary treatment, a normal cervical ultrasonography (C-US), and STg of <2 ng/mL if their test for antithyroglobulin antibody (anti-Tg) was negative. The first two criteria were required for patients with a positive anti-Tg test, and their nominal serum Tg concentrations were not analyzed.
Results:
Twelve patients developed recurrences (2.6%) in cervical region. Greater tumor size, higher STg, and positive anti-Tg tests at initial evaluation were associated with greater R-LTFU. The recurrence rates were 1.5% (7/450) and 26% (5/19), respectively, in patients with negative and positive anti-Tg tests at initial evaluation. Recurrence-free survival was lower in the patients with initial lymph node metastases, positive anti-Tg tests, and STg of ≥0.3 ng/mL at the first postablative WBS (p=0.022, 0.001, 0.035, respectively, by log-rank test). Regression analysis in patients who were anti-Tg negative revealed that STg ≥0.3 ng/mL at this first WBS was the only parameter related to recurrence (p=0.031, odds ratio: 10.30, confidence interval: 1.23–83.3).
Conclusion:
Patients with PTC traditionally categorized as low risk during their first 9 to 12 months after primary treatment have a greater risk of R-LTFU if their postablative STg is ≥0.3 ng/mL, or they have positive anti-Tg, even at this early stage. Periodic C-US is important in these patients and should probably be more frequent in patients with PTC who have positive anti-Tg tests or STg ≥0.3 ng/mL in the first year after diagnosis.
Introduction
The probability of a patient attaining these remission criteria depends on the extent of primary disease, completeness of the primary surgical procedure, effectiveness of the radioactive iodine (RAI) treatment, and tumor characteristics. A more recent guideline paper indicates that patients with STg of <1 ng/mL, as obtained 6–12 months after the primary treatment, can be followed on a long-term basis without further STg measurements (1).
Even in patients with rTSH-STg of <0.5 ng/mL, however, recurrences are observed in about 3% (n=2/62) during long-term follow-up (6). Therefore, we need more information as to how to predict recurrences during long-term follow-up (R-LTFU) even in patients who are in apparent remission. The aim of this study, therefore, was to evaluate the parameters that hypothetically might predict R-LTFU of patients with low-risk papillary thyroid carcinoma (PTC). The study was performed in patients treated and followed at our institution who appeared to be free of disease at the first postablation evaluation that was performed 9–12 months after the first surgical and RAI ablation (n=469).
Patients and Methods
In this study, the data of patients with PTC followed at our institution were retrospectively evaluated. Between 1984 and 2010, medical practitioners at our institution treated and followed 1,882 patients with PTC. Patients with poorly differentiated PTC or PTC that included poorly differentiated or undifferentiated areas were excluded from the study. The remaining patients were included in the study if they had been followed for at least 1 year after their first remission evaluation performed 9–12 months after their first thyroid surgery (and some also had postsurgical RAI remnant ablation), if their thyroid surgery indicated differentiated PTC, and if they had attained remission at the time of this first evaluation. For those who did receive remnant RAI ablation, remission was defined as having a negative WBS, an STg of <2 ng/mL (a time that the serum TSH was >30 μU/mL), having a test for anti-Tg that was negative, and having a negative cervical ultrasonography (C
There were 469 patients (67 men, 402 women) who fulfilled the criteria for the study. Note was taken of PTC tumor histopathology characteristics such as classic, tall cell, columnar cell variant, and diffuse sclerosing, the latter three being associated with a poor prognosis in previous reports. Data regarding patient and tumor characteristics such as age, sex, histopathological subgroup, tumor size, tumor invasion characteristics, presence of initial lymph node (LN) metastasis, presence of multifocality, tumor stage according to tumor-node-metastasis (TNM) classification (AJCC 2002) (7), primary treatment modality, TSH, Tg, anti-Tg measurements at first postablative WBS, follow-up time, presence of recurrence, and recurrence locations were recorded.
The primary surgical procedures for all patients with thyroid cancer were total or near total thyroidectomy. None of our study patients had prophylactic neck dissection. Central and lateral neck dissection was performed in patients with known metastatic LNs preoperatively. In patients with no known metastatic LNs before surgery, only pathologic-appearing nodes detected during surgery were removed. Selected patients received high-dose RAI for remnant ablation. In our study group, 406 patients had undergone total/near-total thyroidectomy and received RAI subsequently as primary treatment. Fixed doses of RAI were used; 30–100 mCi doses were selected for remnant ablation. For patients with LN metastases, 150–200 mCi doses were used. The routine follow-up procedure after thyroidectomy (and RAI treatment) was as follows. A WBS was performed for patients who had received therapeutic doses of RAI approximately 10 days after the high-dose RAI. Uptake outside the neck region was taken as indicative of distant metastasis at presentation. None of our patients had distant metastasis at the time of initial treatment. L-T4 treatment was started promptly afterward, to suppress TSH concentration to values of <0.1 μU/mL during the first year. TSH, Tg, and anti-Tg measurements were repeated at the third month of L-T4 treatment. Patients were also evaluated at sixth months. C-US was performed at that time and thereafter yearly.
A diagnostic 131I WBS was performed at 9th–12th month for patients who had received RAI. TSH, STg (i.e., rTSH-STg, THW-STg), and anti-Tg levels were obtained, and 5 mCi 131I was given followed by the diagnostic131I WBS. This scan was performed after thyroid hormone withdrawal in most patients (n=380); rTSH stimulation was performed in 26 patients. Patients who met the criteria for inclusion in the study (which excluded patients with active disease at this time) had yearly follow-up evaluations.
The follow-up studies in subsequent years were clinical examination, serum TSH, Tg, and anti-Tg measurements while patients were taking L-T4 and C-US. Suspicion that recurrent disease had occurred was based on findings at physical examination, increases of serum Tg to >1 ng/mL while the patient was on L-T4 in association with a negative serum anti-Tg test and suspicious C-US findings. Recurrence was confirmed by cytological and histopathological results in association, when necessary, with diagnostic 131I WBS, X ray findings, and computed tomography/magnetic resonance imaging findings. Cervical LN or local bed recurrences were diagnosed based on C-US findings and on diagnostic WBS studies that indicated definite new uptake in thyroid bed or cervical region. This needed to be confirmed by fine needle aspiration biopsy (FNAB) and measurement of Tg in aspiration (wash-out) material or histopathologically through surgical excision.
The serum TSH, Tg, and anti-Tg concentrations were measured by the Elecsys method at Roche/Hitashi Modular Analytics System. Both analytic and functional sensitivity of this method for Tg measurement was <0.1 ng/mL. The minimum detectable concentration for Tg was 0.1 ng/mL. The analytic sensitivity of the method for serum anti-Tg measurement was <10 IU/mL, and the detection range was 10–4,000 IU/mL. For sera TSH measurements, the detection range was 0.005–100 μU/mL, and the analytic sensitivity was 0.005 μU/mL. These methods have been used in the Central Biochemistry Laboratory of our institution since 2001. Before 2001, Tg concentrations were measured by radioimmunoassay (RIA). Some of the study patients were admitted to our institution before 2001. In those patients who had their first WBS before 2001 and were considered disease free according to the WBS and STg of <2 ng/mL measured by RIA at that time, remission was confirmed by repeated WBS after thyroid hormone withdrawal or rTSH. STg values were also remeasured after 2001. Those who had WBS, TSH, Tg, and anti-Tg measurements during a period of endogenous hypothyroidism (n=80) or after rTSH (n=6) after the year 2001 in order to confirm the presence of remission were included in the study (n=86) if they fulfilled the remission criteria as described earlier. Patients who did not meet remission criteria according to repeated WBS and STg after the year 2001 were excluded. Tg measurements by Elecsys, obtained at the time of repeat WBS in those patients (n=86), were subjected to statistical analysis. In our study, the presence or absence of serum anti-Tg was noted for classification purposes, not the titer of serum anti-Tg. Nominal data for serum Tg concentrations in patients with positive tests for serum anti-Tg at the time of the initial postablative WBS were not included in the statistical analyses.
Statistical analyses were performed by NCSS 2000 software. Descriptive statistical methods were used in addition to chi-square test, chi-square test with Yates' correction, Student's t-test, and Mann–Whitney U test where appropriate. The analyses of prognostic variants for recurrence were made by Cox-regression analysis. Kaplan–Meier survival analysis was applied to determine recurrence-free survival, and log-rank test was used to evaluate the difference between curves. The receiver operating characteristic (ROC) curve analysis was performed to define optimal stimulated Tg cut-off to predict disease recurrence, and area under the curve was calculated. A two-sided p-value <0.05 was considered significant.
The study was performed according to Declaration of Helsinki, and our Institutional Review Board approved the study (Project no: 2009/1544).
Results
The clinical and tumor characteristics of the study group (n=469) are shown in Table 1. The histopathological subgroups of the study patients were as follows: classical PTC (n=261, 55.6%), follicular variant (n=132, 28.1%), diffuse sclerosing variant (n=31, 6.6%), oncocytic variant (n=30, 6.4%), tall cell variant (n=11, 2.3%), and columnar cell variant (n=4, 0.8%) in decreasing order of frequency. The percentage of patients whose PTC was of the histopathological subgroups considered to have a poor prognosis (i.e., tall cell, columnar cell, diffuse sclerosing) was 9.8 (n=46). The mean duration of follow-up was 5.8±3.9 years (median 5/range 2–25). Patients were classified according to the risk stratification of American Thyroid Association (ATA) 2009 guidelines (1). By these criteria, the study group contained 287 patients with low risk (61.2%) and 182 patients with intermediate risk (38.8%) after their primary treatment. Due to our inclusion criteria, none of the study group was in the high-risk category.
SD, standard deviation, tumor size, size of largest tumor when multifocal; RAI, radioactive iodine; mCi, milliCurie; TNM, tumor-node-metastasis.
Three hundred eighty seven patients had serum anti-Tg measurements at the time of first admission. Among them, 58 (15%) had positive anti-Tg. All our patients who had undergone postablative WBS after RAI treatment (n=406) had measured and recorded anti-Tg at the time of that WBS; 19 out of those 406 patients (4.7%) had positive anti-Tg at that time. Therefore, the values for their STg were not included in statistical analysis. During follow-up, 5 out of 19 patients who were anti-Tg-positive developed recurrences. As previously mentioned, 63 patients did not receive RAI after initial thyroid surgery; therefore, these patients did not undergo postablative WBS evaluation.
Twelve of the 469 patients (2.6%) experienced recurrence of PTC during the follow-up period. The study characteristics of 12 patients who experienced recurrence are shown in Table 2. All the patients with recurrence had received RAI ablation after their initial thyroid surgery. Among them, one of the two patients with a tumor size of 0.9 cm had multifocal tumors. The other patient had microscopic soft tissue invasion. The patient with a 0.6 cm PTC had received RAI because of the presence of thyroid capsule invasion. Time to recurrence was 6.9±6.6 (range 2–23) years.
Patients with multifocal tumors (greatest tumor size was recorded).
Became negative after 2 years.
Became negative after 4 years.
Suspicious findings on C-US led to repeat diagnostic WBS.
F, female; M, male, C, central; L, lateral; LN, lymph node; NE, not evaluated; WBS, whole body scan; STg, stimulated Tg at the time of first postablative WBS; C-US, cervical ultrasonography; first WBS anti-Tg, anti-Tg positivity at the time of first postablative WBS; FNAB, fine needle aspiration biopsy; recurrence anti-Tg, anti-Tg positivity at the time of recurrence; ↑, increased.
Five out of 12 patients with recurrence had positive serum anti-Tg tests at the time of their first postablative WBS. During follow-up, the positive anti-Tg tests of three of these patients became negative at second, second, and fourth years after initial thyroid surgery. At the time of recurrence, these patients' tests for serum anti-Tg were negative. In the remaining two patients, tests for serum anti-Tg were positive at the time of recurrences, which developed at the 17th and 23rd years after thyroid surgery. Of the 7 patients with recurrence and tests that had been initially negative for serum anti-Tg, one patient's test for anti-Tg became positive at the time of recurrence.
The majority of recurrences occurred in cervical LNs (8/12-66.6%). Metastatic cervical LNs were mainly confined to lateral cervical region (6/8-75%). Recurrence was suspected by increased Tg concentration when on L-T4 and/or C-US findings and confirmed by fine needle aspiration biopsy and Tg measurement in “washout”-material or surgery. Local bed recurrences (4/12, 33.3%) were confirmed by a definite new uptake in thyroid region on diagnostic WBS in association with C-US that indicated no pathological LNs. One of those four patients with local bed recurrence underwent surgery, and recurrence was confirmed by histopathology. In two patients, increased serum Tg concentrations while on L-T4 in association with normal C-US led to repeat diagnostic 131I WBS, which indicated new uptake in the thyroid region. In a 65-year-old female patient, routine follow-up C-US at 10th year indicated a hypoechoic area at the right thyroid lobe that could not be differentiated from postoperative changes. Tg concentrations remained 0.1 ng/mL on L-T4. Therefore, it was decided to repeat the diagnostic WBS, which showed new uptake in the thyroid bed. Therapeutic doses of 131I were given to those three patients with local bed recurrences, and therapeutic WBS confirmed new uptake in thyroid gland region.
The characteristics of the patients with recurrence and those who remained in remission were compared (Table 3). Mean tumor size, STg at the time of the first postablative WBS, the percentage of patients with positive anti-Tg at the time of the first postablative WBS, and the duration of follow-up were significantly higher in the recurrence group. Nine out of the 14 patients in the remission group had positive serum anti-Tg tests at the time of their first WBS but became anti-Tg negative during follow-up (five patients at second year, three patients at third year, and one patient at fourth year). The remaining five patients still had positive anti-Tg titers at their last follow-up visits (decreasing titers in three patients at third, third, and sixth years of follow-up, unchanged titers in two patients at fifth and sixth years).
Data are presented as mean±SD unless otherwise stated.
p<0.05 is significant (bold).
When patients having positive tests for serum anti-Tg at the time of their first WBS (n=19) were excluded, then the recurrence rate decreased to 1.5% (Table 4). In contrast, in those with positive anti-Tg tests at the time of the first postablative WBS, the recurrence rate was 26% (5/19). The patients who were anti-Tg-negative and experienced recurrence had significantly greater tumor size, higher postablative STg concentrations, and longer total follow-up duration than the patients who were anti-Tg-negative and who remained in remission. The postablative STg was the same in Tables 3 and 4, because serum Tg concentration values in patients with positive tests for anti-Tg were excluded from the analysis.
Sixty-three patients who did not receive radioactive iodine and 19 patients with positive anti-Tg at first WBS are excluded.
Data are presented as mean±SD unless otherwise stated.
p<0.05 is significant (bold).
When the STg obtained at the time of the initial WBS in patients with recurrence was analyzed, an STg value of ≥0.3 ng/mL was chosen as the cut-off point for identifying patients who were likely to experience recurrence. This cut-off point had the best combination of sensitivity and specificity compared with other cut-off points of 0.2, 0.4, 0.5, 0.8, and 1.0 ng/mL (ROC area under the curve=0.772, p=0.014 with a sensitivity of 85.7% and a specificity of 68.7%, positive predictive value 4.8%, negative predictive value 99.6%; data not shown for other cut-off values).
We compared the patients whose postablative STg values were <0.3 ng/mL with the patients whose postablative STg values were≥0.3 ng/mL. Recurrence ratio and tumor size were significantly higher in the patients with postablative STg values ≥0.3 ng/mL (Table 5). Interestingly, the frequency of multifocal tumors was significantly higher in the patients with stimulated Tg <0.3 ng/mL.
Data are presented as mean±SD unless otherwise stated.
According to Kaplan–Meier survival analysis, the recurrence-free survival was significantly lower in the patients with LN metastasis at presentation, with positive anti-Tg at first postablative WBS, and with STg values of ≥0.3 ng/mL at the time of the first postablative WBS as shown in Figures 1 –3 (p=0.022, 0.001, and 0.035, respectively, by log-rank test).

Recurrence-free survival according to presence of initial LN metastasis (p=0.022, log-rank=5.27).
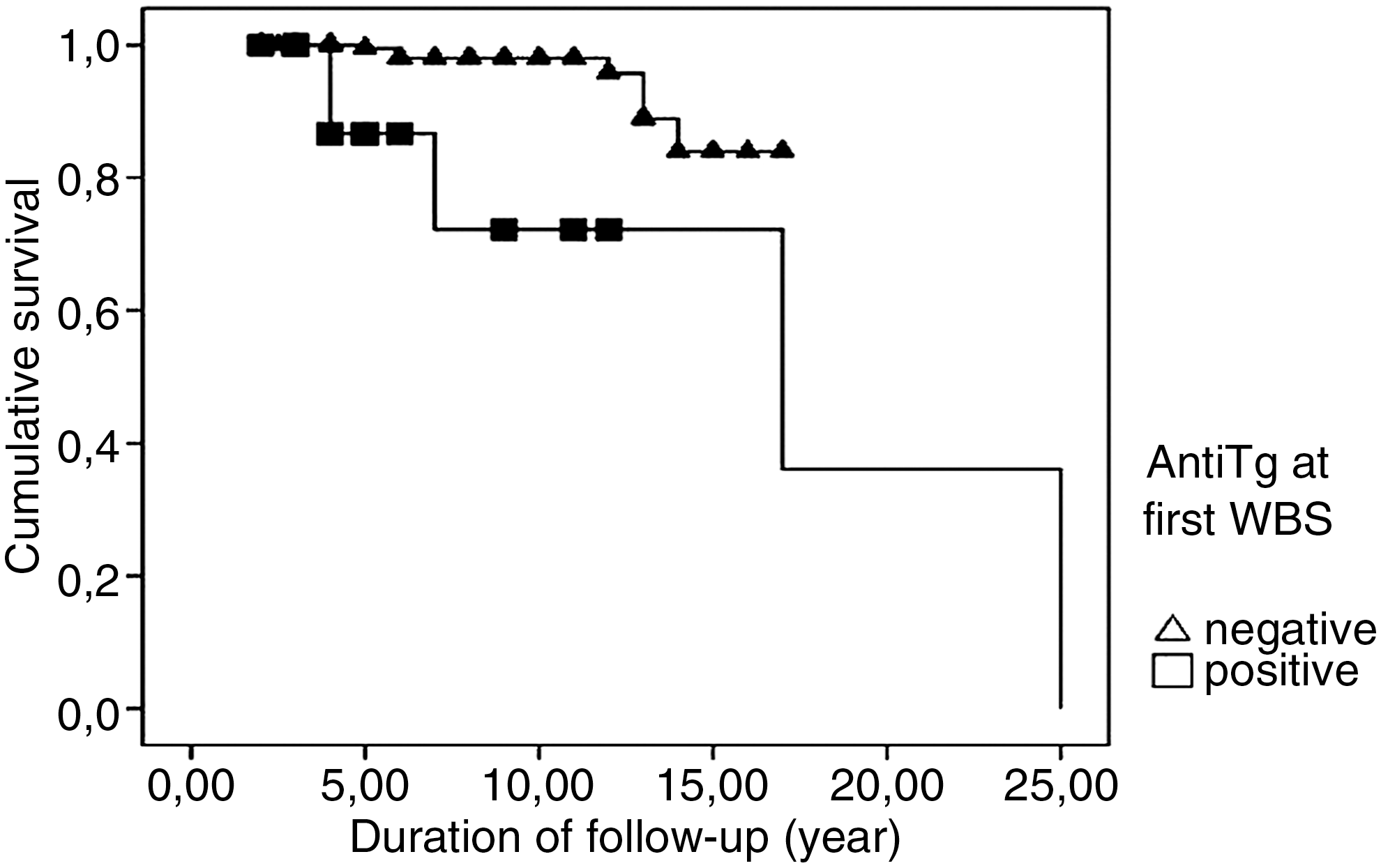
Recurrence-free survival according to anti-Tg positivity at first postablative whole body scan (p=0.001, log-rank=11.67).
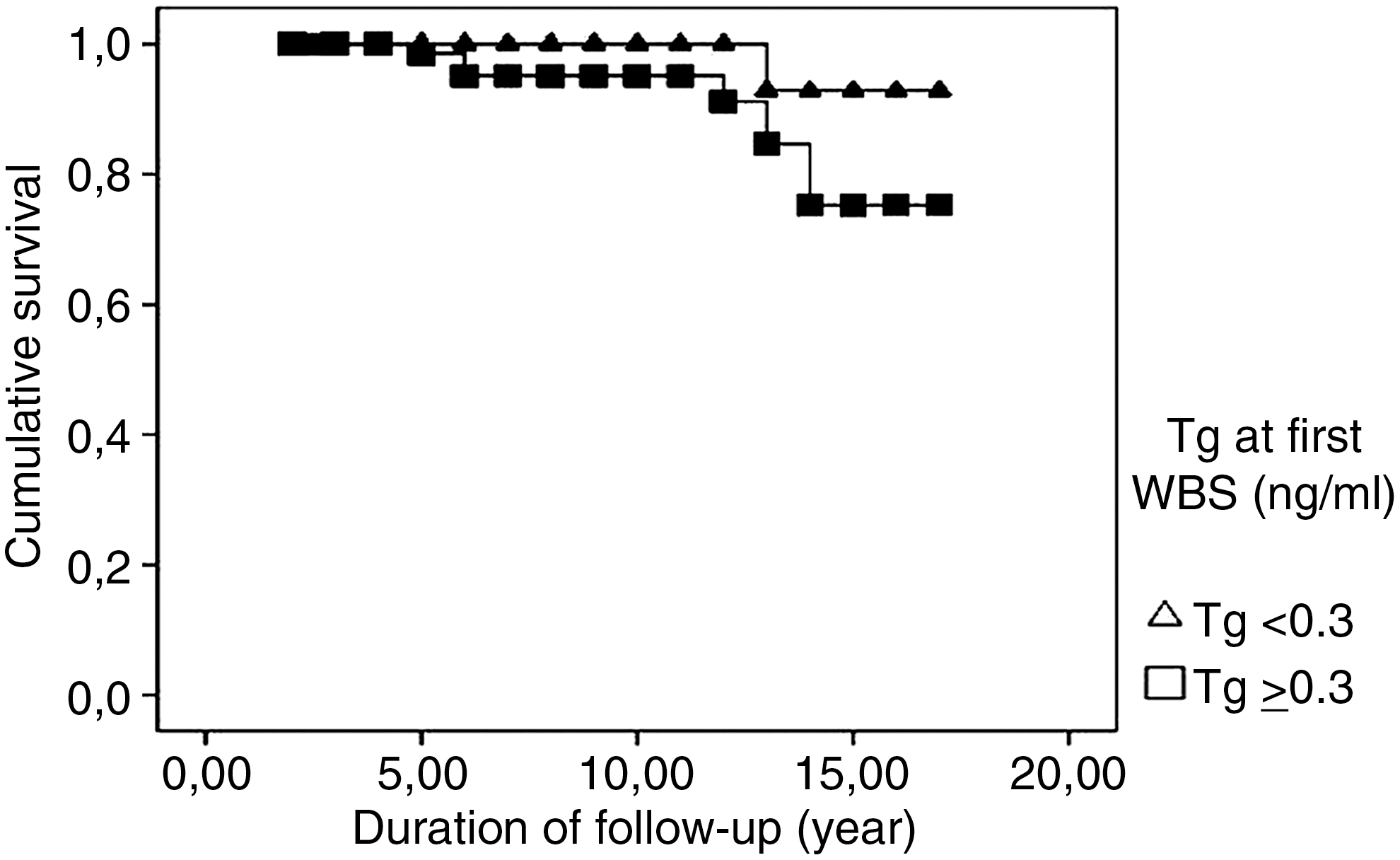
Recurrence-free survival according to postablative stimulated thyroglobulin concentration; <0.3 ng/mL and ≥0.3 ng/mL (p=0.035, log-rank=4.44).
Cox regression analysis revealed that, among several possible prognostic parameters for recurrence (gender, age [<45/≥45 year], vascular invasion, thyroid capsule invasion, soft tissue invasion, initial LN metastasis, tumor size [<1.5 cm/≥1.5 cm], TNM-T stage [T1–T2/T3–T4], multifocality, postablative STg concentration [<0.3/≥0.3 ng/mL], presence of histopathological subgroups related to poor prognosis, belonging to intermediate risk group according to risk stratification of “ATA,” and having positive anti-Tg at the time of postablative WBS), only a postablative STg concentration of≥0.3 ng/mL significantly and independently predicted recurrence (p=0.031, odds ratio [OR]: 10.30, confidence interval: 1.23–83.3).
Discussion
In recent years, many studies have investigated the postablative STg value as a prognostic marker in PTC. STg appeared to have considerable predictive value for R-LTFU of patients with PTC. Recent guidelines from the ATA recommended yearly clinical examinations and Tg measurements while on L-T4 without obtaining further STg values to follow patients with PTC with postablative STg values of <1 ng/mL (1). In patients with PTC who had had a rTSH-STg value of ≤0.5 ng/mL, the prevalence of recurrence was 1.6% during a follow-up period of 3–5 years (8). The patient group in this study was again evaluated, and a recurrence rate of 3% was reported (6). Therefore, even in patients in apparent remission, recurrences may develop during a longer follow-up period. Pelttari et al. (8) retrospectively evaluated 495 patients with low-risk PTC. The recurrence rate in this study was 10.3%, and all the recurrences except one were located in the cervical LNs. Their study group included both patients with PTC and those with follicular thyroid cancer, and the patients received multiple doses of RAI until they were considered disease free, rather than the protocol followed for the patients of our study. They used different methods for measuring serum Tg in various periods of their study. They reported that the finding of serum STg within the measurable range after the first ablation was the best predictor of future recurrence (OR=3.72).
In our study, an initial postablative STg value of >0.3 ng/mL was the only significant predictor of future recurrence as judged by Cox regression analysis; this analysis applies only to patients who are anti-Tg negative. Similar to the study of Pellegriti et al. (9), the first postablative STg values were significantly higher in our recurrence group than in patients in remission, although the clinical importance of such a small but significant difference needs to be explored in a prospective manner (0.51±0.30 vs. 0.30±0.38 ng/mL, p=0.009).
Kloos (6) divided his 107 patients with well-differentiated thyroid cancer into three groups according to their postablative STg: patients with STg <0.5 ng/mL (I), 0.6–2 ng/mL (II), >2 ng/mL (III). Recurrence ratios after a 7-year follow-up period were as follows: 3% in group 1, 11% in group II, and 80% in group III. The percent of patients with recurrence in our study group (2.6%) was similar to that of the first group of Kloos (3%), but with a somewhat longer follow-up period. When patients with positive serum anti-Tg tests at first WBS were excluded, then the recurrence rate was 1.5%.
Pelltari et al. (8) concluded that patients with detectable serum STg after initial thyroid ablation should be followed more closely than those without evidence for circulating Tg. They recommended C-US and measurements of serum Tg while patients were on L-T4 for patients with PTC at a low risk of cancer-specific death with or without detectable postablative STg concentrations, as all the recurrences except one were localized to the neck region.
The results of our study indicate that patients with postablative STg values of <0.3 ng/mL could be safely followed with C-US at intervals of >1 year. The risk of recurrence appears to be very low (1/262-0.4%) for those patients, and recurrence could easily be detected by C-US in experienced hands, as all of our recurrences developed in the cervical region. Patients with relatively higher (≥0.3 ng/mL) STg concentrations at the time of their first post thyroid ablation could also be safely followed with C-US. Further STg measurements did not seem to add benefit to the prediction of recurrence for those patients. The relatively higher postablative STg values in recurrent patients could be explained by the presence of microscopic tumor foci in the cervical region still capable of producing minimal concentrations of Tg. These tumor foci may lead to clinically significant disease in some cases by tumor-specific (i.e., aggressive behavior of tumoral tissue) or patient-specific (i.e., genetic background and host resistance) factors (11,12). At the present time, we are not able to determine clear-cut parameters in tumor tissue and the host that predicts recurrence.
In our study, Kaplan–Meier survival analysis revealed that initial LN metastasis, positive serum anti-Tg tests at the first postablative WBS, and a postablative STg concentration of ≥0.3 ng/mL were also significantly associated with decreased recurrence free survival. The percentage of patients with LN metastasis at presentation was 10.9 in our study. Another study from our department revealed that LN metastasis at presentation was the only factor significantly related to decreased disease-free survival in 138 patients with well-differentiated thyroid cancer (13). Previous studies also indicated LN metastasis as an important risk factor for recurrence (10,14 –16).
The indications for prophylactic neck dissection in well-differentiated thyroid cancer are still controversial. None of our patients underwent prophylactic neck dissection. In our recurrence group, two out of 8 patients with cervical LN metastases had metastatic LN in the central neck region. It is not clear whether initial prophylactic neck dissection would have prevented central neck region LN metastases in these patients.
In our study, the rate of positive tests for serum anti-Tg at the time of the first postablative WBS was significantly higher in the subgroup that had recurrence than those who did not (41.6% vs. 3.0%, p<0.001). Conversely, those with these positive anti-Tg tests at the time of the first postablative WBS had a strikingly high recurrence rate of 26% (5/19). Two patients with recurrence had persistent positive anti-Tg titers until the recurrence time (i.e., 17 and 23 years after primary diagnosis). Persistence of positive tests for serum anti-Tg during follow-up of well-differentiated thyroid cancer has been reported to be associated with recurrent or persistent disease. Conversely, in patients with positive initial tests for anti-Tg, the tests tend to become negative during follow-up in patients who maintain remission. Persistence of positive serum anti-Tg tests imply the continued presence of thyroid remnant or recurrent thyroid cancer, either producing Tg and, thus, stimulating anti-Tg formation (17,18). It is interesting and not completely clear why early presence of serum anti-Tg is such a strong prognostic indicator of future recurrence. In this regard, the observation that Tg antibodies are associated with increased cancer risk in thyroid nodules is of interest (19), suggesting a possible relationship between antigenicity of Tg subtypes and, not only thyroid cancer (19,20), but also aggressiveness of thyroid cancer. Whether or not this hypothesis is correct, and it may have been that the staging of patients who were anti-Tg positive was biased due to inability to measure serum Tg, patients with positive serum anti-Tg tests at the time of their first postablative WBS should be followed-up more closely and in those in whom these tests are persistently positive, the possibility of recurrence should be investigated more vigorously.
The mean duration of follow-up in our study was 5.8±3.9 years. The total follow-up duration was significantly longer in the recurrence group (p=0.001). Longer term follow-up of patients with PTC is associated with increased recurrence rate as previously reported (6,9,15,18). In two of the patients, recurrences were detected 17 and 21 years after primary diagnosis. Therefore, appearance of local recurrence, even in a patient group with apparent remission and low risk, should not be surprising when they are followed long enough. Local recurrences may not decrease survival but may cause morbidity and have negative effects on quality of life.
Conclusion
In our study, the rate of recurrence in a low-risk PTC group who appeared to be in remission after primary treatment was 2.6% (12/469). When patients with positive tests for serum anti-Tg at their first postablative evaluation were excluded, then the recurrence rate was only 1.5% (7/450), but, when only the patients with positive tests for anti-Tg at their first postablative evaluation were considered, then the recurrence rate was 26% (5/19). All the recurrences were localized to the neck. Parameters associated with decreased recurrence-free survival during long-term follow-up in our selected group of patients with PTC were LN metastasis at presentation, postablative STg level ≥0.3 ng/mL, and positive tests for serum anti-Tg at the time of first WBS. In patients who were anti-Tg negative, postablative STg ≥0.3 ng/mL was the sole significant parameter to predict recurrence on Cox regression analysis. These patients, as well as patients with positive anti-Tg, should be followed more carefully for local recurrence. C-US in experienced hands gains utmost importance for long-term management of those patients.
Footnotes
Disclosure Statement
No competing financial interest exist.