
Abstract
Background:
BRAF mutation is the most common genetic event in papillary thyroid carcinoma (PTC); however, the prevalence and patterns of the mutation vary worldwide. We investigated the frequency and type of BRAF mutations based on the histologic subtypes in a large cohort of Korean patients with PTC.
Methods:
A total of 1041 consecutive PTCs were classified according to histologic subtypes. BRAF mutations were examined by denaturing high-performance liquid chromatography and direct sequencing. Rare complex mutations were confirmed by molecular cloning of polymerase chain reaction amplicons and sequencing of the products.
Results:
BRAF mutations were found in 839 (80.6%) of 1041 patients with PTC. The histologic subtype-specific prevalence of BRAF mutation was as follows: 85.3% (249/292) were classic, 45.8% (11/24) were follicular, 79.9% (576/721) were microcarcinoma, and 75.0% (3/4) were other variants. In addition to the usual c.1799T>A mutation, we identified other four mutation types: c.[1795_1796insA;1770_1795dup26], c.[1742-10T>C;1799T>A] and c.[1796C>G;1799T>A], and c.1799_1800TG>AA, respectively. The former three were novel mutations in thyroid tumors. Within the series of microcarcinoma variants, the BRAF mutation rate was lower in tumors with follicular morphology than those with nonfollicular types (66.7% vs. 80.9%, p=0.0145).
Conclusion:
Out of 1041 Korean patients with PTC, 0.4% had rare types of BRAF mutation and three new somatic mutations were identified. The BRAF mutation rate was quite low in PTC with follicular morphology regardless of tumor size. However, the prevalence of BRAF mutation in microcarcinoma and follicular variants of PTC is relatively high in Korea and its analysis may be clinically useful for managing the patients.
Introduction
One nucleotide substitution, T to A, at position c.1799 of the BRAF gene results in a substitution of glutamic acid for valine at amino acid codon 600 (p.Val600Glu mutation). The BRAF Val600Glu mutation is the most common somatic mutation in PTC and is found in 52%–87% of these tumors in the Korean population (2 –4). We have previously reported that the BRAF Val600Glu mutation was found in 162 of 210 (77%) patients with PTC at our hospital (2), which is much higher than that of Western countries (∼45%) (1). In addition to BRAF Val600Glu mutation, other rare BRAF mutations have been reported in PTC. The prevalence and mutational patterns of BRAF mutations vary according to the histologic subtypes of PTC (5). However, the histologic characteristics of patients with BRAF mutations have not yet been studied in Korea.
To further explore the status of BRAF mutation in PTC, we examined the BRAF mutation in a large series of Korean patients with PTC and analyzed the data based on the histologic subtypes of the tumors.
Methods
This study was approved by the Institutional Review Board of Seoul, St. Mary's Hospital, The Catholic University of Korea.
Patients and samples
A total of 1041 consecutive patients (858 women and 183 men) with PTC were enrolled in this study and underwent surgery at Seoul St. Mary's Hospital between October 2008 and June 2010. The age of the patients at the time of surgery ranged from 11 to 81 years (mean 47.2 years). All specimens were collected from patients after informed consent had been obtained in accordance with the institutional guidelines of our hospital.
Tumors were classified according to the World Health Organization classification and included 292 (28.0%) classic PTCs, 24 (2.3%) follicular variants, 721 (69.3%) microcarcinomas, 2 (0.2%) tall cell variants, 1 (0.1%) Warthin-like variant, and 1 (0.1%) solid variant (6).
Genomic DNA extraction from tumor tissue
Genomic DNA was extracted from two 10-μm-thick paraffin sections containing a representative portion of each archival tissue block using the QIAamp DNA Mini kit (Qiagen, Hilden, Germany). Tumor areas were manually microdissected from the tissue sections. In cases with multiple tumor foci, the largest tumors were regarded as the primary lesions and were chosen for the study.
Polymerase chain reaction
A 224 bp fragment of exon 15 of the BRAF gene was amplified by polymerase chain reaction (PCR) using the forward primer (5′-TCATAATGCTTGCTCTGATAGGA-3′) and reverse primer (5′-GGCCAAAAATTTAATCAGTGGA-3′) as previously reported. The PCR conditions were as follows: 35 cycles of 30 seconds at 94°C, 30 seconds at 55°C, and 30 seconds at 72°C. Amplicons were evaluated by 2% agarose gel electrophoresis and purified using a QIAquick PCR purification kit (Qiagen).
Denaturing high-performance liquid chromatography screening
Initial screening for BRAF exon 15 mutations was conducted by denaturing high-performance liquid chromatography (DHPLC), which was conducted using a Transgenomic WAVE genetic analysis system and DNASep column (Transgenomic, Crewe, United Kingdom) packed with alkylated poly (styrene-divinylbenzene) particles as previously described (7). Briefly, PCR products were denatured by heating to 95°C for 5 minutes and then cooled to 25°C over a period of 25 minutes to enhance heteroduplex formation prior to analysis. A total of 20 μL of crude, unpurified PCR products was injected for analysis in each run. The elution temperature was calculated using the WAVEMAKER software (Transgenomic) and was 56.0°C. Wild-type and mutant DNA for the region was used as a reference in all DHPLC runs. Each chromatogram was analyzed visually by two independent observers.
Direct DNA sequencing
Once tumors with an aberrant DHPLC pattern when compared with a control were identified, their purified PCR products were processed for the DNA sequencing reaction as previously reported (2). Briefly, sequencing was conducted in both the sense and antisense directions using the same primers that were used for PCR and an ABI-PRISM BigDye Terminator version 3.1 cycle sequencing kit (Applied Biosystems, Foster, CA) on an Applied Biosystems 3730xl DNA Analyzer. Sequencing reactions consisted of 25 cycles of 10 seconds at 96°C, 5 seconds at 50°C, and 4 minutes at 60°C.
To confirm the authenticity of rare mutations, the following additional methods were used: (i) re-amplification of the exon and repeat DHPLC and bidirectional sequencing analysis on a different day, (ii) re-isolation of genomic DNA from the same tissue block and different tissue block (if available) and repeat DHPLC and DNA sequencing, (iii) bidirectional sequencing analysis using two new sets of primers annealing 209 and 191 bp fragments of BRAF exon 15.
Molecular cloning of PCR amplicons
To better identify the nucleotide composition of novel complex mutations, PCR amplification products were cloned using a TOPO® TA Cloning Kit (Invitrogen, Carlsbad, CA). Briefly, 4 μL of the PCR products was mixed with 1 μL TOPO in a final volume of 6 μL and then ligated at room temperature. For transformation of the plasmid DNA into Escherichia coli, 2 μL of the TOPO cloning reaction was added to a vial of One Shot® Chemically Competent E. coli, after which it was cultured on selective agar plates containing ampicillin. Five white colonies were selected and plasmid DNA was extracted. Purified DNA was sequenced as described previously.
Nomenclature of the mutations
The names of the mutations were assigned according to the guidelines of the Human Genome Variation Society (
Statistical analysis
A chi-square test was used to test for significance of differences in the frequency of BRAF mutations among histologic subtypes. A p-value of less than 0.05 was considered to be statistically significant. All the calculations were conducted using the SPSS statistical software package (version 13.0; SPSS, Inc., Chicago, IL).
Results
After a molecular test based on a combination of DHPLC and DNA sequencing, the presence of a mutation in exon 15 of the BRAF gene was detected in 839 (80.6%) of 1041 patients with PTC. The BRAF mutation data are summarized according to the histologic subtype of PTC in Table 1. The frequency of BRAF mutations was 79.9% (576/721) in microcarcinoma variants of PTC and 82.2% (263/320) in PTC more than 1.0 cm. There was no significant difference in the mutation frequency between the two groups (p=0.3869). The frequency of the BRAF mutations was significantly lower in follicular variants than in other nonfollicular variants (45.8% vs. 81.4%, p=0.0001).
Other rare mutations include c.[1795_1796insA;1770_1795dup26], c.[1742-10T>C;1799T>A], c.[1796C>G;1799T>A], and c.1799_1800TG>AA.
All but four of the BRAF mutations were the usual c.1799T>A mutation. Other rare mutation types included c.[1795_1796insA;1770_1795dup26], c.[1742-10T>C;1799T>A], c.[1796C>G;1799T>A], and c.1799_1800TG>AA. The former three mutations of BRAF have not been reported in PTC. Direct DNA sequencing of the PCR products showed heterozygous mutation patterns overlapped with the wild type. Complex mutation was confirmed as a true mutation within the same allele by subcloning of PCR amplicons and DNA expansion of specific clones followed by DNA sequencing. Analysis of the unaffected thyroid tissue demonstrated that the mutation was of somatic origin.
The clinicopathological data of four patients with rare mutations are summarized in Table 2. Examples of an aberrant DHPLC pattern are shown in Figure 1. Sequence analysis of case 1 showed an insertion of nucleotide A between position c.1795 and c.1796 of the coding DNA sequence (c.1795_1796insA) followed by a duplication of the sequence from nucleotide c.1770 to c.1795 (c.1770_1795dup26). These mutations lead to an insertion of the amino acid lysine between codon 598 and 599 (p.Ala598_Thr599insLys) followed by a duplication of eight amino acids (Lys-Ile-Gly-Asx-Phe-Gly-Leu-Ala) from codon 591 to 598 (p.Lys591_Ala598dup) (Fig. 2A). The mutation of case 2 consisted of one nucleotide substitution, T to A, at position c.1799 of BRAF exon 15 (c.1799T>A) and another substitution of one nucleotide, T to C, at position c.1742-10 of BRAF intron 14 (c. 1742-10T>C) in the same allele (Fig. 2B). The mutation of case 3 consisted of two substitution mutations, C to G at position c.1796 (c.1796C>G) and T to A at position c.1799 (c1799T>A). These mutations led to the substitution of two amino acids, threonine-valine to arginine-glutamic acid at codons 599 and 600 (p.Thr599_Val600>ArgGlu) (Fig. 2C). The c.1799_1800TG>AA mutation of case 4 resulted in a p.Val600Glu amino acid substitution that was the same as the amino acid change caused by the commonly seen c.1799T>A mutation of the BRAF gene (Fig. 2D), and was previously reported in two cases of one lymph node–metastasized PTC and one primary PTC, respectively (9,10).
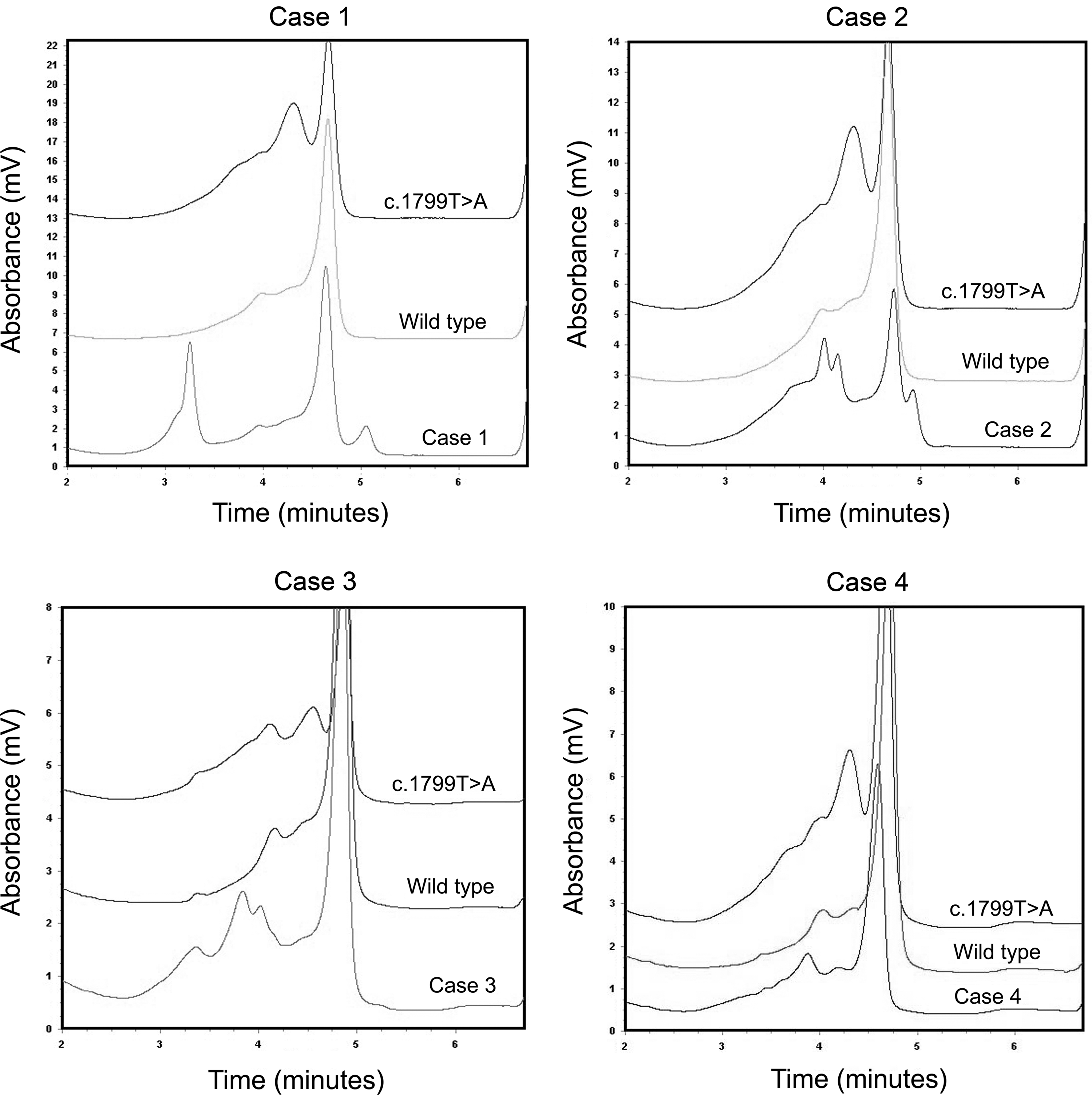
Denaturing high-performance liquid chromatography chromatograms of four patients with rare mutations show aberrant patterns in comparison with the wild-type and c.1799T>A mutation of BRAF gene.
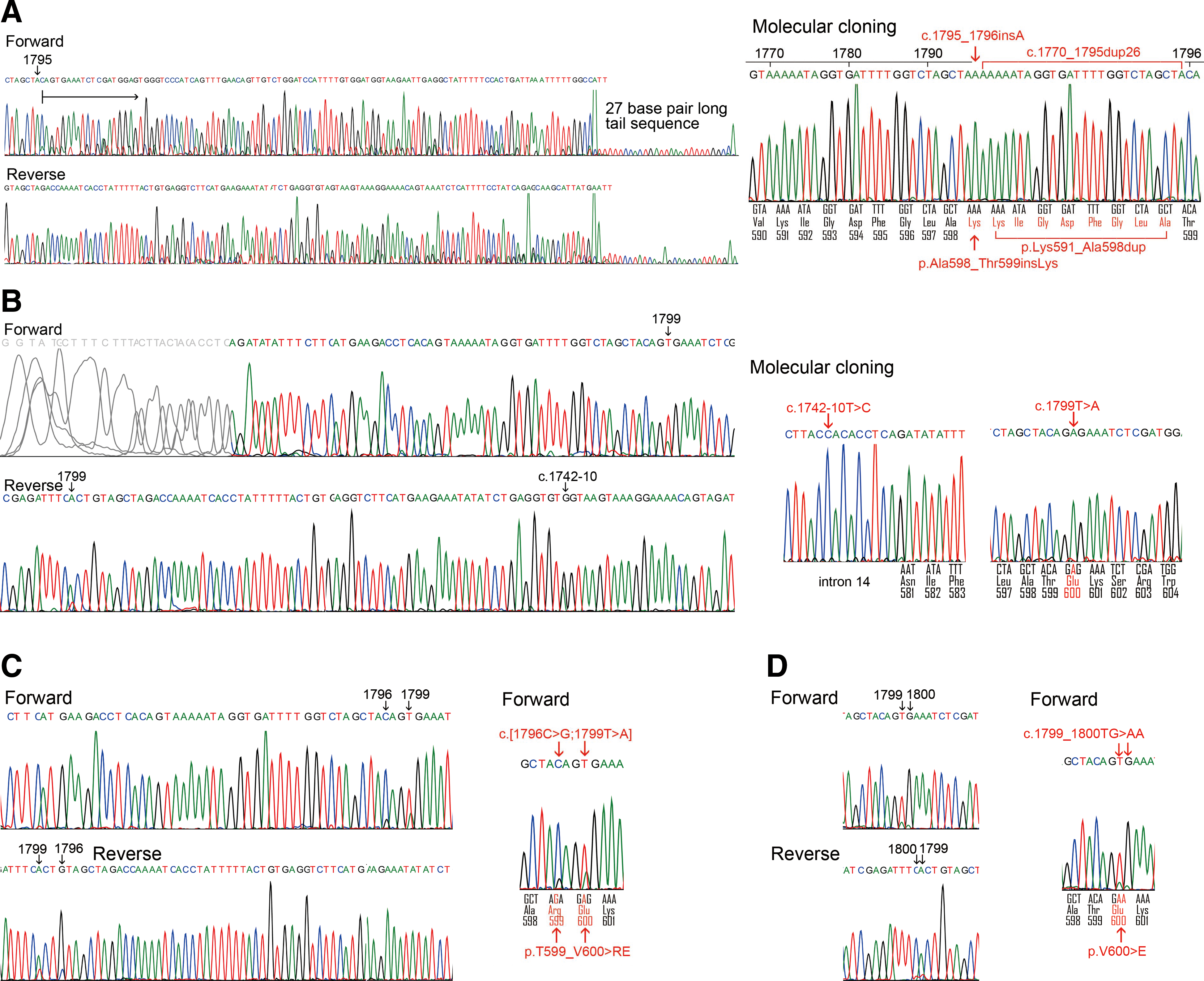
Forward and reverse sequence electropherograms of four patients with rare mutations.
Within the series of microcarcinoma variants defined as PTCs measuring 1 cm or less in size, the tumors were further subcategorized by histologic findings as classic papillary, follicular, tall cell, and Warthin-like morphology (Table 3). The BRAF mutation rate was also lower in microcarcinomas showing follicular morphology than those showing nonfollicular types (66.7% vs. 80.9%, p=0.0145).
Other rare mutations include c.[1795_1796insA;1770_1795dup26], c.[1796C>G;1799T>A], and c.1799_1800TG>AA.
Discussion
Most PTCs carrying the BRAF Val600Glu mutation are classic PTCs, tall cell variants, and Warthin-like variants (5,11). The mutation is present in about 20% of follicular variant of PTC and absent from the cribriform-morular variant (5,12 –14). The low percentage of follicular variants with the BRAF mutation seems to result from poor interobserver and intraobserver reproducibility for the histologic diagnosis of follicular variants of PTC (15,16). The diagnosis of follicular variants is not straightforward and some of tumors included in the molecular test may have been true benign follicular lesions in which the BRAF mutation has not been found. Indeed, in a study conducted by Wallander et al. (16), the BRAF Val600Glu mutation was found in 25% of cases with a complete agreement among pathologists regarding the diagnosis of follicular variants of PTC, whereas none of the cases with a low consensus of diagnosis of the follicular variant showed the BRAF mutation. Moreover, the molecular profile of encapsulated follicular variant of PTC is similar to that of follicular adenoma and carcinoma with a high prevalence of RAS and low BRAF mutation rate, and infiltrative follicular variants of PTC have a higher BRAF mutation rate than do the encapsulated variants (17). Therefore, the BRAF mutation rate of the follicular variant may vary depending on whether or not the tumor is encapsulated. In the present study, the prevalence of BRAF mutations was high in PTC (80.6%) but remained in the range usually reported for this gene in Korea (2 –4,18). Out of 1041 cases, 24 (2.3%) were classified as a follicular variant of PTC and 45.8% of the follicular variants showed the BRAF Val600Glu mutation. This prevalence is relatively high in Korea compared with Western countries and maybe explained by the fact that the BRAF mutation in PTC is highly prevalent in Korean patients, and that its prevalence also varies among geographical regions and ethnic groups, as well as with iodine intake (18,19).
Microcarcinoma variants of PTC, which are defined by strict criteria, are true incidental PTCs measuring ≤1 cm in size that are found in surgical specimens resected due to benign thyroid nodules or during laryngectomy. However, in the present study, most of the tumors were preoperatively diagnosed or suspected to be malignant since preoperative ultrasound sonogram and fine-needle aspiration cytology were conducted for most of our patients. Specifically, we applied only the size criterion to define the microcarcinoma variant, similar to many other studies that have been conducted to date. Therefore, the microcarcinomas in the present study may not be true occult cancers. The frequency of microcarcinoma was 69.3% among total PTCs and this high rate may explain the reasons for the current rapid increase that is being observed in the incidence of PTC. The BRAF mutation rate did not differ between microcarcinoma variants and PTCs of more than 1.0 cm in size. Among all PTCs, the BRAF mutation rate was lower in follicular variants of PTC than in nonfollicular variants. Within the series of PTC ≤1 cm in size, microcarcinomas showing follicular morphology also had a lower mutation rate than those showing nonfollicular findings. These molecular results support the idea that BRAF mutation occurs at an early stage during PTC development and microcarcinoma variants may only be early detected PTCs rather than a specific disease entity.
Mutation of c.1801A>G substitution of the BRAF gene leading to the substitution of a lysine by a glutamate at codon 601 (p.Lys601Glu) has been detected in up to 9% of cases of the follicular variant of PTC and in very rare cases of follicular adenoma (5,20). However, the mutation has not been found in other histologic subtypes of PTC. In the present study, there were no cases of PTC showing BRAF Lys601Glu mutation. We only detected one case of minimally invasive follicular carcinoma with BRAF Lys601Glu mutation in the other study (data not shown).
Other rare BRAF mutations in PTC are summarized in a study by Chiosea et al. (21) and on the web site of the Sanger Institute (
In human tumors, over 40 mutations of the BRAF gene have been found (22,23). Most oncogenic BRAF mutations are located in the glycine-rich P loop (residues 462–471) and activation segment (residues 593–622) (22,23). The Glu586Lys, Val600Glu, Val600Asp, Val600Lys, Val600Arg, and Lys601Glu mutations were classified as a high kinase activity group, while nine other mutations, Gly464Glu, Gly464Val, Gly466Ala, Gly469Glu, Asn581Ser, Phe595Leu, Leu597Val, Leu597Arg, and Thr599Ile, were classified as an intermediate kinase activity group (22,23). However, four mutations, Gly466Glu, Gly466Val, Gly596Arg, and Asp594Val, have lower kinase activity than the basal wild-type BRAF activity (22,23). Activation of wild BRAF requires phosphorylation of Thr599 and/or Ser602 residues within the activation segment (22). The BRAF Val600 mutations mimic phosphorylation of Thr599/Ser602 and destabilize interactions between the residues within the hydrogen bond network in BRAF, rendering the BRAF constitutively active (22,24). In the present study, the functional consequence of the c.[1795_1796insA;1770_1795dup26] mutation of case 1 has not been characterized. Case 3 showing p.Thr599_Val600>ArgGlu was considered to have strong kinase activity although we did not conduct a study to functionally characterize the novel mutations.
In conclusion, BRAF Val600Glu mutation is very frequent among Korean PTC patients and 0.4% of the patients have other rare mutation types. Three new somatic mutations were found in a functionally critical region of the BRAF gene. The BRAF mutation rate is quite low in PTCs with follicular morphology regardless of tumor size. However, the relative prevalence of BRAF mutation in both microcarcinomas and follicular variants of PTC is still high in Korea and its analysis may be clinically useful for managing patients with the tumors.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.