
Abstract
Background:
Anterior compartment syndrome (ACS) and rhabdomyolysis are rare complications of hypothyroid myopathy. We report the case of a young man with rapid onset of ACS who presented with simultaneous primary hypothyroidism and adrenal insufficiency associated with acute renal failure, hyponatremia, and hyperkalemia.
Patient Findings:
A 22-year-old man presenting with a one-month history of tiredness, hyperpigmentation, and cramps in his calves was found to have severe bilateral foot drop. Investigations revealed severe primary hypothyroidism and adrenal insufficiency, renal failure, and evidence of rhabdomyolysis with myoglobinuria. Abnormal biochemical findings included serum sodium of 110 mM, serum potassium of 6.9 mM, and serum creatine kinase (CK) of >25,000 IU/L. Magnetic resonance imaging (MRI) of his legs showed changes of myonecrosis confined to anterior tibial muscles typical of ACS. After treatment with intravenous fluids, potassium-lowering therapies, thyroxine, and hydrocortisone, his renal and metabolic function returned to normal, but irreversible bilateral foot drop persisted.
Summary:
A young man with primary hypothyroidism, adrenal insufficiency, hyponatremia, and hyperkalemia presented with severe myopathy, such that muscle necrosis, apparently confined to the anterior tibial compartment on MRI, led to rhabdomyolysis, acute renal failure, and irreversible bilateral peroneal nerve damage. It is possible that other patients with primary hypothyroidism and marked elevations of CK without widespread myopathy or rhabdomyolysis may demonstrate evidence of differential muscle effects in the anterior compartment when assessed by MRI, but that this patient also had adrenal insufficiency raises the possibility that this was a contributing factor.
Conclusions:
Severe thyroid myopathy and rhabdomyolysis may be associated with anatomic susceptibility to ACS, particularly in the presence of concomitant adrenal insufficiency. MRI examination reveals a distinctive appearance of myonecrosis confined to the anterior compartment.
Introduction
Patient
A previously well 22-year-old male university student presented to the emergency department with a one-month history of shin splints, tiredness, and cold intolerance. His feet had been swollen and tingling for 3 days. There was no history of unusual or excessive exercise or of his having taken statins or other drugs or alcohol.
On examination, he was lethargic with mild skin hyperpigmentation. His heart rate was 65 per minute and supine blood pressure was 150/110 mmHg without postural change. There was nonpitting edema of the lower legs without muscle wasting, absent ankle tendon reflexes, and 1/5 power of ankle dorsiflexion bilaterally.
His serum sodium concentration was 110 mM, potassium 6.9 mM, creatinine 410 μM, creatine kinase (CK) >25,000 IU/L (normal <220 IU/L), free thyroxine 2.5 pM (normal 12–22 pM), thyrotropin >100 mIU/L (normal 0.3–4 mIU/L), and urine myoglobin 20.1 mg/L (normal <1 mg/L).
The provisional diagnosis was of rhabdomyolysis and consequent acute renal failure with associated bilateral lower leg anterior compartment syndrome (ACS) associated with severe primary hypothyroidism. Primary adrenal insufficiency, suspected because of the presence of recent skin hyperpigmentation, was confirmed by an early-morning serum cortisol of 79 nM (normal 200–700 nM) and plasma adrenocorticotrophic hormone of 969 pM (normal 2–11 pM). Antithyroid peroxidase autoantibody titer was 1580 U (normal <60 U), and the adrenal autoantibody titer to steroid-21 hydroxylase was 8.3 U (normal <1 U).
Hyperkalemia was urgently treated with nebulized salbutamol, intravenous calcium gluconate, plus dextrose, and insulin infusion as well as oral calcium resonium. Normal saline was infused to counter any prerenal failure and the severe hyponatremia. With these measures, there was clinical and biochemical improvement after 3 hours to serum sodium of 116 mM, potassium 4.7 mM, creatinine 330 mM, and narrowing of the QRS complex on the electrocardiogram from 145 to 110 milliseconds.
He was treated with hydrocortisone 100 mg every eight hours, and the dosage was tapered from the third day to 30 mg daily after 1 week, fludrocortisone 100 μg daily, and thyroxine 500 μg as a stat dose orally, and then 200 μg daily. He steadily improved and renal failure resolved within one week. Serum CK remained elevated at >25,000 IU/L on discharge 1 week after admission and was still mildly elevated at 840 IU/L 4 weeks later when thyroid function was normal.
Magnetic resonance imaging (MRI) of his legs at presentation showed changes consistent with swelling, inflammation, and necrosis confined to anterior tibial muscles typical of ACS, with sparing of posterior calf muscles (Figs. 1 and 2). Over the ensuing 8 weeks, dorsiflexion did not improve, nerve conduction studies confirmed bilateral common peroneal nerve paralysis, and repeat MRI was unchanged. Bilateral tibialis posterior to tibialis anterior tendon transfers were later performed to enable him to walk without ankle-foot orthoses.
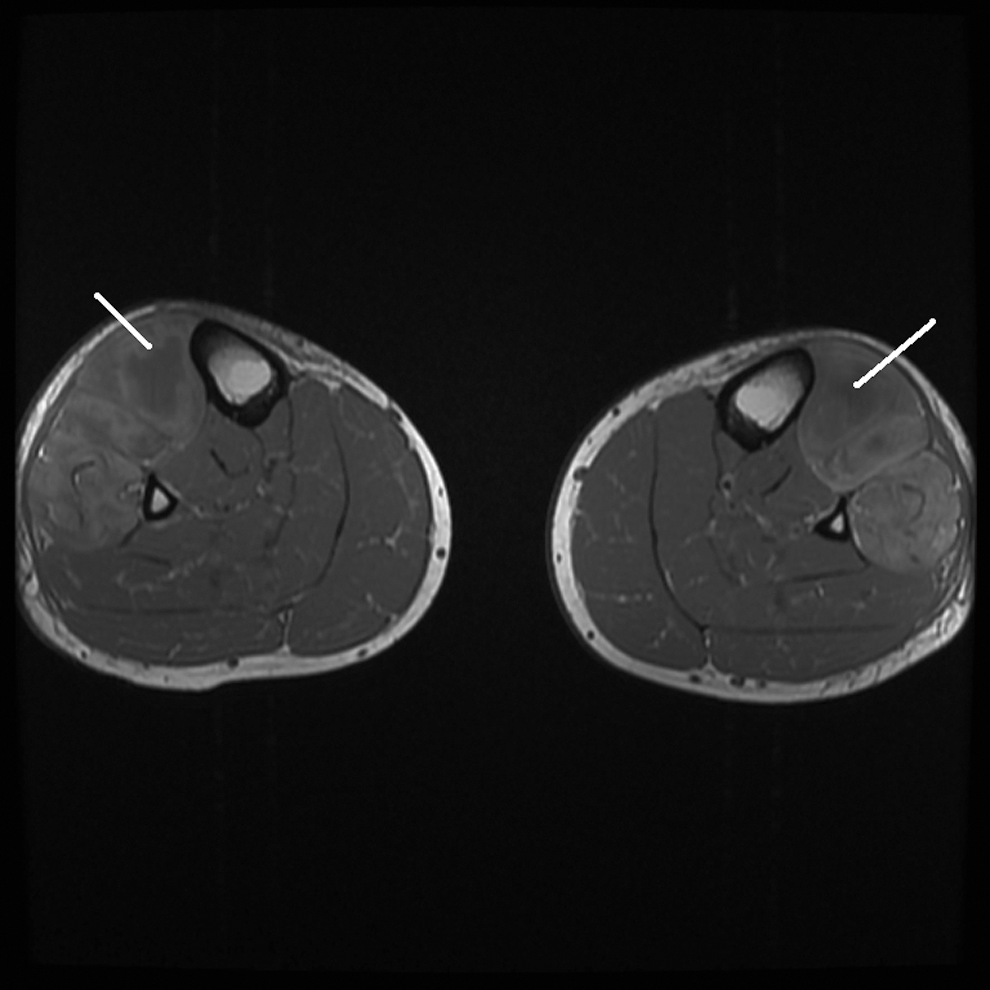
Lower leg magnetic resonance imaging axial T1 with anterior compartment muscles showing altered signal swelling and loss of normal muscle striations.
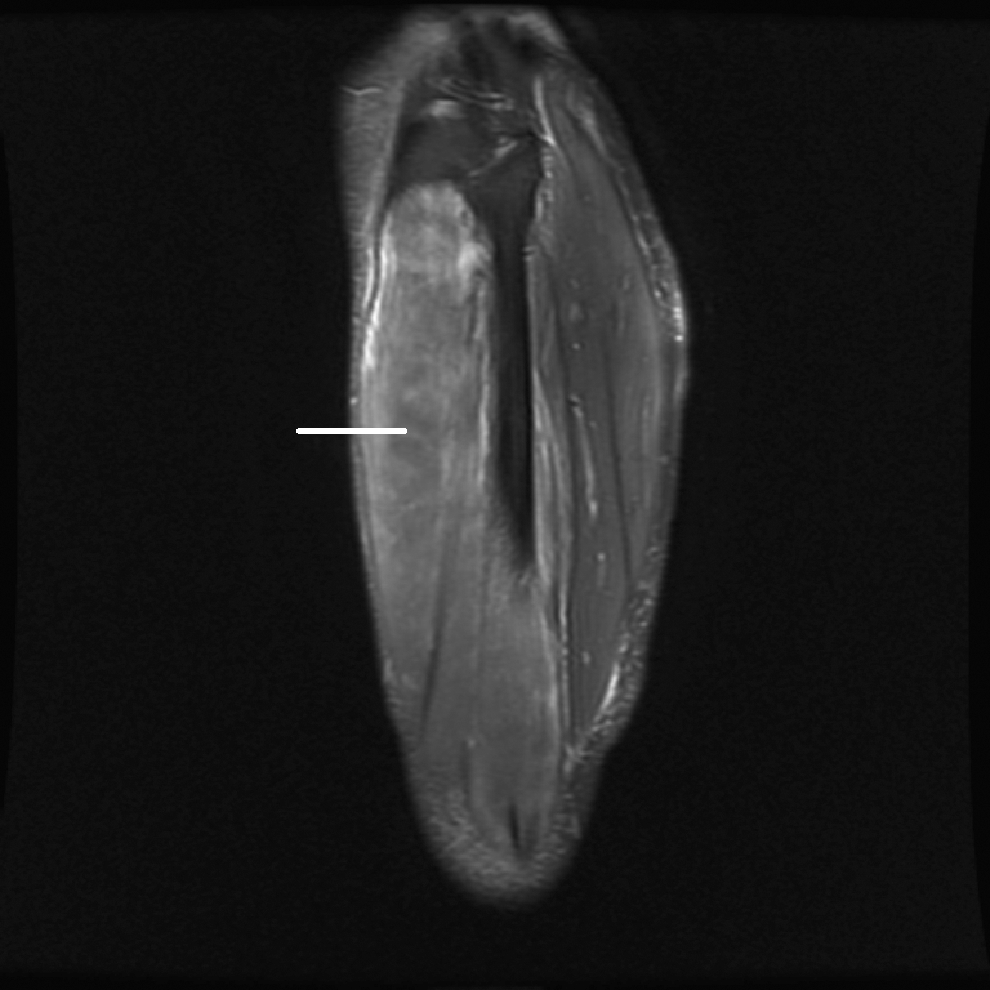
The sagittal view of right lower leg with fat saturation emphasizes the difference between the two compartments.
Discussion
This young man had an unusual combination of severe autoimmune primary hypothyroidism, adrenal insufficiency, myopathy, hyponatremia, and hyperkalemia leading to ACS, rhabdomyolysis, and reversible acute renal failure. A loading dose of oral thyroxine was chosen for the acute management of myxedema coma and in view of the lack of availability to us of parenteral triiodothyronine that might otherwise have provided faster reversal of hypothyroidism. The severity of his bilateral ACS caused irreversible pressure damage to both common peroneal nerves despite his short history, prompt diagnosis, and treatment. Because his was a chronic ACS, present >48 hours in contrast to acute trauma, urgent decompressive fasciotomy was not performed.
Rhabdomyolysis has been reported in adrenal insufficiency and in combined autoimmune primary adrenal and thyroid failure or Schmidt's syndrome, as here (1,2). More commonly, even in severe hypothyroidism, there are only minor symptoms of hypothyroid myopathy such as stiffness, aching, and modest CK elevation (3). Muscles may be enlarged and pale when examined, because of interstitial edema and mucinous deposits, but frank muscle necrosis with rhabdomyolysis is rare, perhaps requiring an anatomic predilection related to the anterotibial compartment.
ACS in a patient with hypothyroidism was first reported in 1993 (4) and a second case 2 years later (5). ATC surgical release was performed in each case, but without benefit (4,5). In our patient, the interstitial myositis, myopathy, and perhaps the physical structure of his anterior compartment may have combined to cause local muscle necrosis without symptoms or signs of myopathy elsewhere, as demonstrated by the normal clinical findings and MRI appearance in muscle groups outside the ATC. We speculate therefore that there may be an anatomic susceptibility to ACS in selected patients with severe primary hypothyroidism. In contrast to the reversibility of acute traumatic ACS, the spontaneous development of the syndrome over several days to weeks, associated with complete foot drop and severe muscle necrosis on MRI, argues against the utility of decompression as an aid to peroneal nerve recovery. In a related context, it has been suggested that postexertional MRI may have a useful screening role in the investigation of chronic compartment syndrome that usually presents with recurrent episodes of pain on exercise (6). Future investigation by MRI of the lower legs in hypothyroid patients with myopathy and raised serum CK without rhabdomyolysis may show evidence of differential anatomic muscle appearances short of frank necrosis.
Footnotes
Disclosure Statement
The authors disclose no potential conflicts of interest.