
Abstract
Background:
Since patients with thyroid cancer have a very good prognosis overall, clinicians may often assume that their quality of life is comparable to the general population. We hypothesized that quality of life of thyroid cancer patients is lower compared with the general population while controlling the effect of age and gender.
Methods:
At the beginning of their stay at an inpatient rehabilitation clinic, a cohort of n=121 patients with thyroid cancer were assessed using the quality of life core questionnaire of the European Organisation for Research and Treatment of Cancer (QLQ-C30). Data for comparison were derived from a representative German community sample with n=2037.
Results:
The patients reported significantly more problems than the community sample participants independent of gender and age effects in all but two domains, namely constipation and diarrhea. The strongest effects of the group (patients vs. general population) were found in the following domains: insomnia (B=−43.7, p<0.001), fatigue (B=−38.0, p=<0.001), and role functioning (B=29.7, p=<0.001). Significant interactions between age and group occurred in the social functioning, role functioning, fatigue, nausea/vomiting, and financial difficulties domains. Quality of life was unrelated to the stage of the disease, except in the physical function and global health status domains.
Conclusions:
At the beginning of inpatient rehabilitation, patients with thyroid cancer often experience more problems than controls from community samples, independent of their age and gender. Clinicians should be aware of the fact that quality of life is not directly related to the severity of the cancer prognosis.
Introduction
Indeed, some authors have shown that individuals with thyroid cancer generally have a quality of life that it is comparable to those in the general population (6,7), but findings have been mixed; others have reported impaired quality of life compared with community samples or healthy controls (8 –12), and compared with patients with other tumor entities such as laryngeal cancer (13). In some studies, findings have varied between individual quality of life parameters. For example, a group of 341 patients with differentiated low-risk thyroid cancer reported fewer problems with symptoms and discomfort but more problems with sleep, speech, and distress than a large community sample (14). In another study, quality of life decreased before and 3 months after thyroid cancer surgery but recovered 6 months after baseline so that no difference existed any more between patients and general population but in social functioning (15).
With increasing age, quality of life gets generally worse in thyroid cancer patients (14,16,17), whereas anxiety and depression is higher in younger patients (18). Women sometimes reported more problems than men (6), sometimes no gender differences were observed (5,16).
A key weakness of a number of studies to date has been a lack of data on age and gender, both of which may be important confounders and/or effect modifiers. The aim of our study was to compare the quality of life of thyroid cancer patients with that of the general population while controlling the effects of age and gender directly by using raw data from a large representative community sample.
Methods
Design and procedure
This study was a single center cross-sectional study using comparison data from the general population. Between 2006 and 2010, at the beginning of their stay in an inpatient rehabilitation clinic in Bad Oexen, Germany, all consecutive patients with thyroid cancer were approached and asked to complete a questionnaire. In Germany, all cancer patients have access to inpatient rehabilitation free of charge for 3 weeks shortly after finishing their initial oncological treatment, and most take up the opportunity. They can also attend the clinic within the first year after diagnosis for little money. Thus, approaching patients in rehabilitation clinics represents an effective way of collecting data from a presumably representative sample.
Data from the general population were collected by conducting face-to-face interviews using the same questionnaire. Individuals were sampled randomly via the Random Route technique (19).
Informed consent was obtained from each study participant after full explanation of the purpose and nature of data collection and storage. This research meets the ethics guidelines of the institution where the study was performed, including adherence to the legal requirements of Germany.
Assessment methods
The instrument used to measure health related quality of life was the Quality of Life Core Questionnaire of the European Organisation for Research and Treatment of Cancer (EORTC QLQ-C30). It is a 30-item self-report instrument, comprising five functioning scales (physical functioning, social functioning, role functioning, emotional functioning, and cognitive functioning), a scale for global quality of life and nine symptom scales (fatigue, nausea/vomiting, pain, dyspnea, sleep disturbances, appetite loss, constipation, diarrhea, and financial difficulties). The QLQ-C30 was developed specifically for cancer patients and is widely used in field studies and clinical trials throughout the world (20). Scores of the functional and symptom scales are constructed by summation, imputation of missing values, and transformation. The scales computation procedure is described in detail elsewhere (20).
Sociodemographic and medical parameters including age, gender, stage of disease, and type of thyroid cancer were collected from the medical records.
Statistical analysis
Univariate comparisons between the patients and the community sample were performed using chi-square tests for frequencies and two-tailed Student's t-tests for quantitative variables. Differences between subgroups of thyroid cancer patients were investigated using one-way analysis of variance or the nonparametric Kruskal–Wallis equality-of-populations rank test, according to the distribution of the data.
Full linear regression models, that is, with all possible interaction terms, with the independent variables gender, group (general population vs. patients), and age (centered on the mean) were computed to investigate multivariate associations.
Distribution of the residuals and multicollinearity were checked to ensure that the method of ordinary least squares was appropriate. Potential heteroskedasticity was investigated by visual inspection of residual versus fitted values plot and using the Cook–Weisberg test. If heteroskedasticity was present, robust standard errors were used. All statistical analysis was performed using STATA 11 (21).
Results
Sample
Patients
During the study period, a total of 148 thyroid cancer patients were admitted to the rehabilitation clinic of which 121 (81.7%) could be enrolled for this study. Nonparticipation was mainly associated with insufficient command of German, age >80 years, and illiteracy.
Most of the study participants were female (n=98, 81%) and under the age of 50 (n=71, 59%). The type of cancer was mostly papillary (n=86, 71%) or follicular (n=24, 20%), representing the usual incidence pattern of thyroid cancer. Further details are presented in Table 1.
p-value for comparison between thyroid cancer patients and general population.
NA, not applicable.
Thirty-four of the patients came into the clinic shortly after their initial oncological treatment (on average 2 weeks later) and 87 came within the first or second year after diagnosis (on average 7 months after completion of oncological treatment). Data on lymphadenectomy status are unfortunately incomplete; therefore no reporting is possible here.
General population
Comparison data of 2037 subjects from the general population were available. In this group, 1142 participants (56%) were female, that is, fewer than in the patient group. Therefore, adjustment of gender effects was performed in the multivariate analyses. The age distribution was similar in both groups (see Table 1).
Quality of life in patients
Within the patient group, men reported better emotional functioning than women (mean value 60.5 compared with 46.7, p=0.03); no other gender differences were observed. Patients with papillary or follicular cancer also reported worse emotional functioning than patients with medullary or anaplastic diseases (mean values 47.2 and 51.0 compared with 76.4. and 83.3). Mean scores in all other domains appeared to be similar between the different histology types (see Table 2). No statistical tests were performed here because of the small sample size in the medullary and anaplastic histology patient groups.
SD, standard deviation.
Patients with large tumors (T4) indicated worse physical functioning (60.0 vs. >75 in all other patients, p=0.02) and a decreased global health status (39.4 vs. >54 in all other patients, p=0.03). Tumor size was not associated with other quality of life domains (Table 3). No significant differences were found between patients with and without lymph node metastases. Prevalence of distant metastases was associated with decreased cognitive functioning (41.7 vs. 65.9, p=0.05).
T, tumor size; N, lymphnode metastases status; M, distant metastases status.
Quality of life in the general population
Within the representative community sample, women reported significantly worse functioning and more symptoms than men in all domains except diarrhea and financial difficulties (see Table 4; all p<0.05). With increasing age, quality of life decreases linearly.
B, B coefficient of linear regression analysis (corresponding to mean difference between patients and general population); ES, effect size for comparison between patients and general population; CI, confidence interval.
Quality of life in patients versus general population
Univariate analyses
The comparison of patients' and the general population's quality of life revealed more symptoms and decreased functioning in all domains in the patient group (see Table 4 and Fig. 1). Large differences were seen in the following domains: fatigue (difference 39 points), role functioning (33 points), insomnia (33 points), emotional functioning (29 points), and financial difficulties (28 points). All differences between the two groups were statistically significant (with p<0.01).
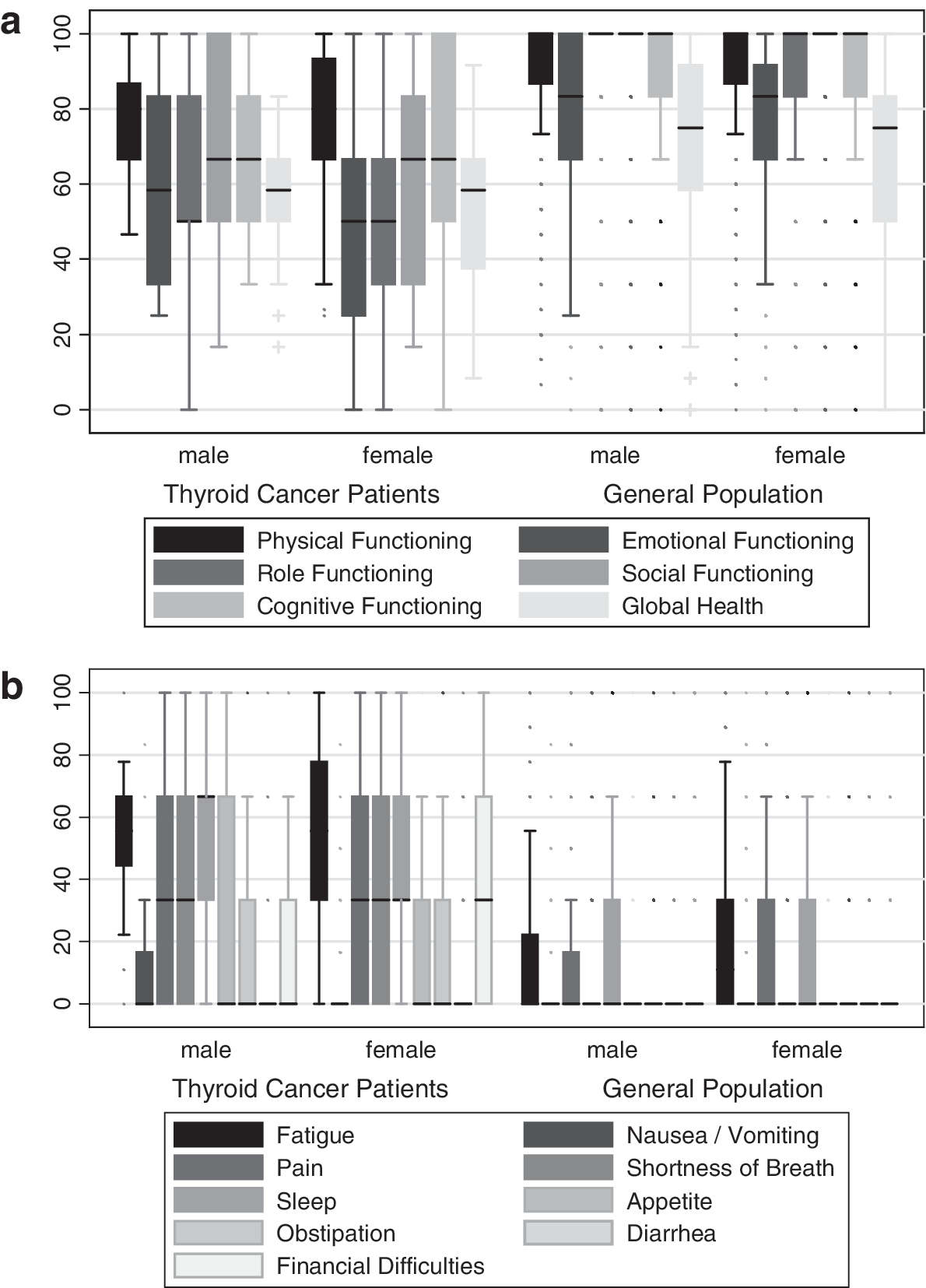
Quality of life in the patients with thyroid cancer (n=121) and in the general population (n=2037).
Multivariate analysis
To control potentially confounding effects of age and gender, multiple linear regression was performed. Table 5 shows that in all but two domains, namely constipation and diarrhea, the patients reported significantly more problems than the community sample participants independent of gender and age effects. The strongest effects between the groups (patients vs. general population) were found in the following domains: insomnia (estimated difference in means [B]=−43.7, p<0.001), fatigue (B=−38.0, p=<0.001), and role functioning (B=29.7, p=<0.001).
Displayed are the B coefficients of multiple linear regression analyses.
Indicates the use of robust standard errors.
BL, baseline category.
Significant interactions between age and group occurred in the domains social functioning, role functioning, fatigue, nausea/vomiting, and financial difficulties, the last representing the strongest interaction. An interaction implies that, for example, the difference in financial difficulties between patients and the general population varies by age. To illustrate that relationship, age was dichotomized at a cutoff of 45 years (see Fig. 2). While financial difficulties usually are found more frequently in older people, patients have more problems at younger ages. Interactions between gender and group were observed in nausea and vomiting only.
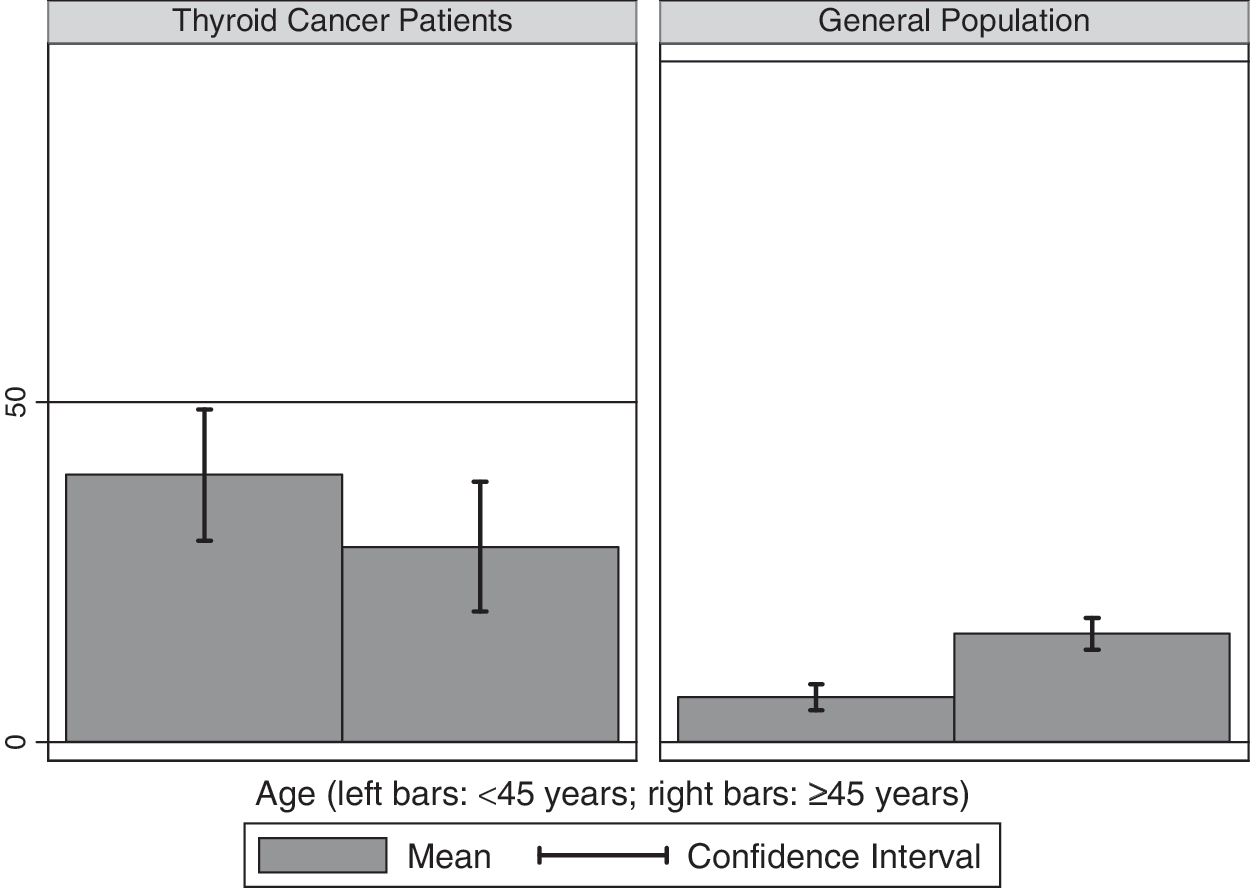
Financial difficulties in thyroid cancer patients versus general population. Illustrated is the effect modification by age. Displayed are the mean values in each group (high scores represent more problems) and the 95% confidence intervals.
Discussion
The results of this study suggest that patients with thyroid cancer at the beginning of inpatient rehabilitation do suffer from significantly more symptoms and worse functioning than the general population, independent of age and gender effects. In other words, the decreased quality of life in the patient group is not just a result of the fact that usually women report more problems than men (19) and that incidence of thyroid cancer is higher in women than in men.
The most frequent complaints of the patients were fatigue, sleep disturbances, and decreased emotional and role functioning and the largest differences between patients and general population, adjusted for age and gender effects were in sleep problems, fatigue, role functioning, cognitive functioning, social functioning, and financial difficulties.
This result is in accordance with most other studies (8 –12) but in contrast with two investigations that found no difference between patients and general population in some domains (6,7). Similarly, Roberts et al. who had used the same EORTC core questionnaire for their quality of life assessment, found much better scores in their patient sample (22). One possible explanation for that difference is that the time since diagnosis plays a role, that is, it is possible that quality of life improves with time. Some of the symptoms, for example, fatigue, sleep problems, and impaired cognitive functioning, could be related to postoperative thyroxine withdrawal. In the Crevenna study, patients were investigated on average 5 years after diagnosis and Roberts et al. had seen 57% of their patients >3 years after diagnosis, whereas our patients were seen shortly after their initial treatment. On the other hand, a number of cross-sectional studies reported that there was no association between the quality of life and the time since diagnosis (16,23,24); and patients reported more problems than the general population with sleep, speech, and distress even years after the diagnosis (14). Another explanation is that selection bias led to better results in the study by Roberts et al.: only 43% of patients returned their questionnaires and the proportion of well educated participants in that study was very high. If education level is associated with quality of life then this could explain the different results, though at least two studies have found no such association (5,18). Unfortunately, no data on education level were available in the present study.
Our study sample is likely to represent the population of thyroid cancer patients in Germany adequately: all cancer patients nationally have access to inpatient rehabilitation that is paid for by the insurance companies, and most take the opportunity. According to the statistics of the insurance companies in the year 2004, n=1310 thyroid cancer patients (0.94% of all cancer patients) attended inpatient rehabilitation clinics whereby 75% of them were female and the average age was 50.8 years (25). In our group, 81% of the patients were female and they were 46.5 years old on average.
To ensure our sample was unbiased, we analyzed tumor registry data of the years 2008 and 2009 of a large city in Germany (Leipzig), comprising n=10,680 incident cases of cancer. Of these, n=103 (0.96%) were thyroid cancer patients, aged 60.2 years on average and 68% being female. Thus, in our sample, female and younger patients are slightly overrepresented (however, this was controlled by adjusting the effects of age and gender), and the percentage of patients in inpatient rehabilitation clinics represents the incident cases fairly well.
Overall, there is strong evidence for a decreased quality of life in the patients compared with the general population especially regarding fatigue, insomnia, role functioning, and mental health. This is important to note as some clinicians tend to overestimate patients' well-being due to the fact that their prognosis is relatively good. However, better prognosis does not necessarily translate to better quality of life (26 –29) or better emotional functioning (30), and our results suggest that doctors need to directly assess and address all aspects of their patients' quality of life, regardless of their tumor stage or progression.
Even within our patient group we saw this counter-intuitive relationship: Emotional well-being was decreased especially in patients with papillary and follicular thyroid cancer although these cancer types have a better prognosis than anaplastic or medullary cancers.
Generally, few differences between patient subgroups were seen in our study. It is possible that this is an effect of the questionnaire chosen. Although it is an instrument specifically developed for cancer patients, it is possible that some thyroid-specific symptoms are not covered by it. Unfortunately, no thyroid-specific module of an EORTC Questionnaire exists that could be used in surveys or clinical trials. Consequently, most studies so far have used generic quality of life instruments such as the SF-36 (6,7,9 –11,24,31) and often no subgroup differences were investigated. Thyroid-specific modules have been used only rarely (3,15,17,32); these instruments have a different concept than the EORTC Questionnaires. Since many EORTC QLQ-C30 data of clinical and community samples exist and are available for comparison, an EORTC thyroid-specific module would be a useful tool, if developed in future.
Another limitation of our study was the cross-sectional character of the data collection. Although it was an advantage to have a relatively homogeneous patient population due to collecting the data consistently at the beginning of inpatient cancer rehabilitation, no follow-up was conducted. There might have also been a selection bias as older people (aged over 80 years) tended to decline study participation more frequently. Even though we did not find a strong effect of age on quality of life, we cannot rule out that such a selection mechanism might have affected our results.
Another feature of this study was both an advantage and a disadvantage. As we contacted the patients personally and not with a mailed questionnaire, we could increase the response rate, thus minimizing possible selection bias. On the other hand it is possible that participants might have exaggerated their problems in a face-to-face setting, for example, if they felt that this would result in more physician attention, and this could have introduced an information bias. The use of a standardized questionnaire should have reduced any such effect but it cannot be ruled out entirely.
Finally, the distribution of histology subtypes in this study was not equal, making it more difficult to compare subgroups. This distribution most likely reflects the incidence pattern of thyroid cancer rather than any biased selection of patients. However, the power of statistical testing is reduced if the samples are small, making it more difficult to detect small differences between patient groups. In most studies so far, this problem was dealt with by excluding all patients with medullary or anaplastic cancer. In our view, this is a suboptimal technique as it makes it hard to gather more information on those patients. We preferred to report their data descriptively and to use nonparametric analyses to test differences between them.
In summary, we have shown that patients with thyroid cancer at the beginning of inpatient rehabilitation appear to experience more quality of life problems than controls from community samples, independent of their age and gender. Clinicians should be aware of the fact that quality of life is not directly related to the gravity of the cancer prognosis, and therefore of the importance of separately assessing their patients' quality of life.
Footnotes
Disclosure Statement
All authors declare that there is no conflict of interest that could be perceived as prejudicing the impartiality of the research reported. This research did not receive any specific grant from any funding agency in the public, commercial, or not-for-profit sector.