
Abstract
Background:
Thyroid surgery is common, but complications may occur. High-intensity focused ultrasound (HIFU) is a minimally invasive alternative to surgery. We hypothesized that an optimized HIFU device could be safe and effective for ablating benign thyroid nodules without affecting neighboring structures.
Methods:
In this open, single-center feasibility study, 25 patients were treated with HIFU with real-time ultrasound imaging 2 weeks before a scheduled thyroidectomy for multinodular goiter. Thyroid ultrasonography imaging, thyroid function, were evaluated before and after treatment. Adverse events were carefully recorded. Each patient received HIFU for one thyroid nodule, solid or mixed, with mean diameter ≥8 mm, and no suspicion of malignancy. The HIFU device was progressively adjusted with stepwise testing. The energy level for ablation ranged from 35 to 94 J/pulse for different groups of patients. One pathologist examined all removed thyroids.
Results:
Three patients discontinued treatment due to pain or skin microblister. Among the remaining 22 patients, 16 showed significant changes by ultrasound. Macroscopic and histological examinations showed that all lesions were confined to the targeted nodule without affecting neighboring structures. At pathological analysis, the extent of nodule destruction ranged from 2% to 80%. Five out of 22 patients had over 20% pathological lesions unmistakably attributed to HIFU. Seventeen cases had putative lesions including nonspecific necrosis, hemorrhage, nodule detachment, cavitations, and cysts. Among these 17 cases, 12 had both ultrasound changes and cavitation at histology that may be expected for an HIFU effect. In the last three patients ablated at the highest energy level, significant ultrasound changes and complete coagulative necrosis were observed in 80%, 78%, and 58% of the targeted area, respectively. There were no major complications of ablation.
Conclusion:
This study showed the potential efficacy of HIFU for human thyroid nodule ablation. Lesions were clearly visible by histology and ultrasound after high energy treatments, and safety and tolerability were good. We identified a power threshold for optimal necrosis of the target thyroid tissue. Further studies are ongoing to assess nodule changes at longer follow-up times.
Introduction
Therefore, there is considerable interest in identifying therapeutic alternatives to surgery. Recent studies have suggested several nonsurgical, minimally invasive approaches for treating symptomatic disease, including ethanol injection, percutaneous laser ablation, or radiofrequency ablation (1,2,5 –10). Side effects are not rare, including pain, vocal cord palsy, and extrathyroid fibrosis and can affect further surgical strategies. Thus, most expertise centers are interested in finding less invasive alternative treatments.
High-intensity focused ultrasound (HIFU) is a thermal ablation now routinely used in several centers worldwide to treat localized prostate cancer (11). HIFU is currently under development for gynecological tumors (12,13) and hepatocellular (14) or renal-cell carcinomas (15 –17). A pilot study was recently reported on HIFU ablation for hyperparathyroidism (18). In addition, our previous studies indicated that HIFU could induce necrosis in ewe thyroids (19). The safety and reproducibility of this method were confirmed in a larger series of 27 ewes and showed that HIFU ablation could successfully destroy thyroid tissue (20). This justified the initiation of clinical trials in humans using a modified version of the Ablatherm HIFU device (EDAP, Vaulx-en-Velin, France) and also emphasized the need for precise targeting and optimization of the firing parameters (ultrasound intensity, duration, and cooling time) to treat the whole thyroid nodule without damaging the surrounding key structures. We reported the first human series of 25 patients treated with HIFU for benign thyroid nodule before a scheduled thyroidectomy. The primary goals of this feasibility study were first, to assess safety, and second, to determine technical treatment parameters for precise necrosis of the targeted thyroid nodule without any clinically significant adverse events. Two weeks after HIFU treatment, evidence of nodule destruction was obtained by macroscopic and microscopic histological examinations of thyroid tissue removed during surgery. We tested different acoustic treatment parameters to optimize the treatment for further clinical development. To our knowledge, no previous or ongoing studies have investigated these issues in the field of thyroid disease.
Materials and Methods
Study design
The study was a monocentric, open-label, nonrandomized, noncontrolled trial. From 2003 to 2006, we enrolled 25 consecutive patients with multinodular goiter who were scheduled for thyroidectomy. These patients had undergone HIFU treatments before surgery. INSERM and Theraclion SAS supported these trials.
Patients
The study population was composed of 5 men and 20 women, aged 25–82 years (mean age, 49 ± 15 years). Entry criteria were (i) at least two thyroid nodules, with at least one indicated for surgery; (ii) the nodule targeted for HIFU treatment was located at least at 3 mm from the trachea, the esophagus, the recurrent nerve, the carotid artery, and the skin; (iii) the selected nodule for HIFU treatment was different from the one indicated for surgery to avoid disturbing the histological examination. No maximal limits of volume were defined for the targeted nodule.
Exclusion criteria were (i) suspicion of malignancy in the nodule (positive FNA biopsy or suspicious cervical lymph nodes), neck irradiation, previous surgery, or previous radioactive iodine treatment; (ii) any cystic component that exceeded 20% or any large calcifications; and (iii) inability of the patient to remain in a stable position with the neck hyperextended.
Written informed consent was obtained from all 25 patients. All patients were informed of the known possible adverse effects of HIFU ablation (skin burn, pain, vocal cord palsy, tracheal and esophageal injuries, and recurrence of the treated nodule). The study was approved by the French Institutional Review Board (CCPPRB Saint Louis Hospital, Paris, France: October 18th 2002) and approved by AFSSAPS (French Agency for the Safety of Health Products: February 18, 2003, number 2002/10/026).
The date of thyroid disease onset was between 1987 and July 2005 for twenty patients, and was unknown for five patients. Nine patients declared taking concomitant medication that did not interact with the HIFU treatment. Two patients were receiving treatment for thyroid disease (patient #4 was taking suppressive therapy with levothyroxine 100 μg daily, and patient #19 was taking carbimazole 20 mg and levothyroxine 25 μg for Grave's disease).
The results of thyroid palpation (n = 24) were normal for three patients, and abnormal for twenty-one patients. The mean body mass index (BMI) was 27 ± 6 (n = 18); three patients had a BMI > 30: #1 (BMI 39), #6 (BMI 35), and #10 (BMI 34).
Eleven patients had at least one FNA. Seven of these FNAs yielded a suspicion of malignancy (but not in the nodule treated with HIFU).
Laboratory and imaging evaluation
At baseline, the patients underwent blood tests to determine the levels of thyrotropin (TSH; immunochemoluminometric assays), free triiodothyronine (FT3), free thyroxine (FT4; radioimmunometric assays), calcitonin, and thyroglobulin.
Each patient also underwent high-resolution ultrasonography imaging (10 MHz linear transducer; Toshiba). Numerous exploratory parameters were carefully recorded to characterize and describe the nodule targeted for HIFU treatment, including its height, width, thickness, location, distance to trachea, distance to esophagus, distance to the carotid artery, and distance to the skin. The target nodules were also assessed for echostructure, echogenicity, calcification, outline, halo, aspect of Doppler vascularization, and energy (Table 1). The nodule volumes were calculated according to the spherical ellipsoid formula: vol (mL) = depth × width × length (cm) × π/6.
DIPAE, depth-independent pulse acoustic energy.
Baseline hormonal values were obtained in all patients except patient #24. This patient had normal levels of hormones at all the other time points of the study.
The mean TSH value was 1.28 ± 1.55 mU/L at baseline (n = 24). Two patients had abnormal results. Patient #19 had a TSH level of 7.9 mU/L, which indicated subclinical hypothyroidism, because FT3 and FT4 were at normal levels. This was consistent with the treatment she received for ongoing Grave's disease. Patient #25 had a TSH level of 0.03 mU/L, with normal FT3 and FT4 hormone levels. She was 82 years old, with an indication of thyroidectomy for pretoxic goiter.
The mean FT4 value at baseline was 16 ± 2 pM, and the mean FT3 was 3.84 ± 0.61 pM (n = 24). These values were normal for this study population. The mean thyroglobulin value at baseline was 322 ± 579 μg/L (n = 24). This highly variable result was expected for benign goiters.
Calcitonin at baseline was normal (<8 ng/L) in all patients except patient #15, who had an elevated baseline calcitonin level (1294 ng/L); this level remained stable over time. At the final histological examination, it was found to correspond to a unifocal medullary cancer contralateral to the HIFU-treated nodule.
After the HIFU session, patients were examined at 1, 3, 8, and 15 days. At each visit, they were assessed by the same physician for weight, blood pressure, heart rate, and cervical palpation. Careful patient questioning and physical examinations were performed to determine possible side effects or adverse events.
Laboratory tests were assessed at 1, 8, and 15 days after HIFU treatment. Thyroid sonography was performed at 3, 8, and 15 days after treatment. The ultrasonography examiner had no access to previous findings about the nodule. Ultrasonographic changes were defined as at least one change in the following: echostructure (solid to mixed), echogenicity (hyper- or iso- to hypoechoic), or power Doppler (a one-step decrease at least from +++ to 0).
Thyroid scintigraphy scans were not included in the selection criteria, but were available for 10 patients. These showed low fixation except for patient #19, who had Grave's disease.
HIFU ablation
HIFU is a minimally invasive technique that allows for elective thermal tissue destruction (coagulative necrosis and cavitation) within a few seconds by focusing a beam onto a given target. When ultrasound waves enter the tissue interface (the skin and the muscles), the beam is wide and the power density is low, ensuring that no damage occurs to these superficial structures. During a HIFU treatment, the computer-controlled device will incur small adjacent lesions (2 mm diameter by 8 mm in depth) that destroy the selected volume.
Different treatment parameters were used to induce different sizes of lesions at different positions by modifying the power, pulse duration, pulse delay, intensity, and acoustic frequency. The ranges for these parameters were based on previous treatments for human prostates and sheep thyroids (19,20).
The device
A modified HIFU device (Theraclion SAS, Paris, France) was built for this first human trial. Its design was based on the device built to treat the thyroid gland in ewes (19,20). The focused energy was delivered from an external treatment unit that contained both ultrasound and imaging transducers.
The ear-nose-throat (ENT) HIFU (Theraclion SAS) is a computer-driven system composed of an electronics cabinet, an extracorporeal probe (3 MHz frequency) mounted on a gantry and moved by stepper motors, a cooling unit, and an ultrasound imaging scanner (Bruel & Kjaer Model Falcon 2101; 7.5 MHz 128 element imaging linear array). The elements of the ENT HIFU are controlled with a PC-type computer running a specially designed software package.
The treatment head was improved with a series of prototypes, as follows:
The first prototype (head IA) had a movable firing and imaging transducer. Either the linear array imaging transducer or the treatment transducer could be positioned to face the target. This version did not allow for continuous monitoring of the treatment site.
In the second prototype (head II, V1 and V2), the linear array imaging transducer viewed the target through a slot in the treatment transducer. This allowed continuous monitoring of the treatment site. The first version of head II (V1) had a treatment transducer emitting area that was not maximized, and the focus was 45 mm. The head II,V2 design was improved for skin protection; the treatment transducer emitting area was maximized; and the focal point was reduced to 38 mm (56 mm diameter, 38 mm focal length, and focal region dimensions 2.5 × 8 × 1.8 mm).
The body of the probe can rotate around the acoustic axis, allowing alignment with the target in either the transverse or longitudinal plane. The system includes a patient movement-sensing device that immediately interrupts treatment when the patient moves or swallows.
Treatment
The procedure was performed by a specialist in ultrasonography on an outpatient basis under real-time ultrasound guidance using a transducer. The patients were placed in the supine position with the neck extended. Local anesthesia was administered; lidocaine with 1% adrenaline was used for some patients.
The imaging and targeting were conducted with the linear array transducer included in the device. The nodule was spotted and drawn on the screen of a computer-controlled treatment unit. Safety distances were based on data obtained in the preclinical study conducted in sheep. The device achieved submillimetric targeting accuracy; thus, a 3 mm margin was implemented for safety in this first human trial. The computer sequentially moved the ultrasound beam over the nodule, creating multiple, contiguous, millimetric foci of necrosis. When the patient moved, treatment was automatically stopped. In a typical treatment, it took less than half an hour for the treatment head to cross over the entire treatment zone.
When no significant reduction in vascularization was observed in the treated nodule by Doppler ultrasonography and/or when no ultrasonographic changes were observed, a second HIFU session was planned on day 8 (two patients).
To achieve complete destruction of the nodules, the acoustic energy was increased stepwise for different groups of patients. The actual acoustic energy delivered to the nodule depended on several factors, including pulse duration, reference acoustic energy, number of shots, and depth. When the nodules were deep, the actual acoustic energy was increased to take into account the absorption by the tissue located between the skin and the nodule. Thus, we calculated the depth-independent pulse acoustic energy (DIPAE) to provide a measure of the pulse energy that can be compared among patients or treatments.
Twenty-two patients were analyzed for efficacy in four different treatment groups, as follows:
Group 1 (n = 4): Patients #1, #2, #3, and #4 were treated with treatment head IA, no sedation, and a DIPAE of 35 J. Group 2 (n = 4): Patients #5, #6, #7, and #8 were treated with treatment head II,V1; patients #5 and #6 had no sedation, and patients #7 and #8 had a subcutaneous injection of lidocaine with 1% adrenaline. DIPAE was 34 J for patient #5, then increased to 45 J for the others in this group. Group 3a (n = 6): Patients #11, #12, #14, #15, #16, and #17 were treated with treatment head II,V2; all had general sedation. DIPAE was gradually increased from 38 to 51 J. Group 3b (n = 5): Patients #18, #20, #21, #22, and #23 were treated with the same treatment head II,V2, but had different sedation and energy management: a local intranodular lidocaine with 1% adrenaline injection was added, and the DIPAE was increased from 58 to 85 J. Group 4 (n = 3): Patients #24, #25, and #26 were treated with treatment head II,V2; all received oral and local intranodular sedation and a DIPAE of 94 J.
Safety assessment
The safety of the treatment was assessed by evaluating adverse events that occurred during and after the HIFU session. Pain was subjectively assessed on a visual analog scale of 0 to 100.
Surgery and evaluation of thyroid nodule destruction
The indication for surgery was a multinodular goiter and toxic multinodular goiters in 22 and 3 cases, respectively.
After HIFU treatment, the thyroid lobe that contained the targeted nodule was removed during surgery, fixed with formaldehyde, and sent to the pathologist for macroscopic and microscopic examinations. One expert pathologist (B.F.) performed all pathologic assessments. The HIFU-induced lesion was assessed macroscopically for targeting precision and microscopically for a qualitative assessment of necrosis. The efficacy endpoint was the extent of nodule destruction. A pathology report of the whole thyroid specimen was performed for each patient.
Histological slides were prepared for the treated nodule, colored, and photographed. For each figure that shows a nodule, the most representative slide was selected.
The pathologist defined zones of destruction and zones undamaged by HIFU. A specific analysis of the treated area was based on previous observations of sheep thyroids to facilitate the identification of pathological lesions attributable to HIFU (PLAH) (19,20). The PLAH were defined by the presence of coagulative necrosis, multiple fibrotic scars, thrombosis, and a cystic area surrounded by typical lesions. Other putative nonspecific lesions, such as noncoagulative necrosis, hemorrhage, nodule detachment, cavitations, and cysts, were considered due to HIFU when concomitant ultrasound changes were observed.
The % of nodule destruction was estimated with a semiautomatic morphometric analysis. One tissue section per case was selected that corresponded to the tissue section with the largest PLAH. The corresponding slide was digitized with a Nikon coolscan 5 image scanner, and the transferred image was subjected to a semiautomatic estimation of the treated area. The treated area and the PLAH were outlined in different colors with a Wacom® Graphire®4 pen. Areas were color-coded as follows: black for total nodule area, green for typical HIFU lesions (PLAH), red for putative HIFU lesions (noncoagulative necrosis, hemorrhage), and blue for cavitations.
The percentage of destruction was the ratio of the surface area with signs of HIFU destruction to the total surface area of the targeted nodule. It was determined for each treated nodule by counting pixels in each colored zone (Table 2).
The putative HIFU lesion area was larger than the treated nodule area.
DIPAE, depth-independent pulse acoustic energy; PLAH, pathological lesions attributable to HIFU (coagulative necrosis, multiple fibrotic scares, thrombosis, cystic area surrounded by typical lesions).
Results
Safety and treatment tolerance
The most frequent adverse events were local pain, mild skin burns, and cough; during treatment, local pain occurred in nine patients (#1, #2, #6, #9, #11, #13, #22, #23, and #25), mild skin burns appeared in seven patients (#5, #6, #8, #10, #16, #19, and #21), and cough appeared in two patients (#16 and #19).
Out of the 25 treated patients, 3 were discontinued for pain (patient #13) or skin micro-blister (patients #9 and #10). Thus, these were excluded from the efficacy analysis.
Among the seven patients with blister, five had slight skin burns that spontaneously resolved within a few days; one had a large blister. The device was modified (see below) to resolve this problem, and no blisters occurred with the latest device head.
Patient discomfort and pain increased proportionally with increases in delivered energy, and pain ceased between pulses. The average subjective pain score was 25/100. Thus, it was necessary to adapt the analgesia to the degree of energy delivered. A local lidocaine intranodular anesthesia was introduced as a premedication.
Stepwise improvements in technical parameters
Technological innovations were implemented to develop a prototype capable of continuous targeting and to control proper treatment head positioning for safety. Targeting the delivered HIFU pulses was improved by integrating an image system.
The energy of the pulses was gradually increased throughout the study from 35 to 94 J to achieve a level that provided satisfactory coagulation on histological examination. The increases were implemented first by changing the pulse duration and then by changing the nominal acoustic power.
The first three patients were treated with parameters based on those used in the published series of sheep (19), and only a small volume was targeted in the center of the nodules. The intent for patients #4–#25 was to target the whole nodule within an external safety margin.
Skin blisters appeared with increasing energy levels. Thus, to eliminate these cutaneous problems, the treatment head and treatment parameters were progressively adapted by reducing the radius of curvature of the transducer to reduce the focal point. When the focal point is decreased, the zone of acoustic energy delivered through the skin is decreased, and this lowers the temperature at the skin; however, this strategy maintains an efficient temperature at the targeted focal point. The immediate result of these technical modifications was successful destruction of the largest nodule area without cutaneous or other side effects. The last three patients exhibited optimal tissue necrosis; this indicated that the optimal DIPAE was 94 J.
Response to HIFU treatment
Biological results
Patient #24 (82 years old) had a pretoxic goiter with a low TSH level at baseline and showed an isolated increase in FT3 at day 8. Apart from that, there were no significant changes in TSH, FT3, or FT4 after HIFU treatment. A transient peak (twice the baseline level) of thyroglobulin was observed the day after HIFU treatment (day 1) in five patients (#19–#23).
Ultrasonographic and pathological results
All 25 patients received HIFU shots in a selected thyroid nodule; 3 patients received an insufficient number of HIFU shots, and efficacy was not assessed. Out of 22 cases, 17 showed no change in nodule size at 15 days.
After treatment, ultrasonography detected significant changes in at least one of the following: echostructure (solid to mixed, n = 10), echogenicity (hyper- or iso- to hypoechoic, n = 7), or blood flow (at least a one step decrease from +++ to 0 in a power-Doppler examination; n = 9). A total of 16 out of 22 patients evaluable for ultrasonography showed changes that were expected due to HIFU (echostructure becoming mixed, an echogenicity decrease, or a vascularization decrease assessed by the Doppler energy score; Table 2).
In the total series, pathology reports of the treated nodules showed 17 macrofollicular adenomas, 4 microfollicular adenomas, and 1 atypical adenoma (Table 2). Twenty-two patients had nodule destruction that ranged from 2% to 80%. Among this group, five patients had over 20% PLAH (20%, 32%, 38%, 58%, 69% respectively). Seventeen cases had putative lesions, including nonspecific necrosis, hemorrhage, nodule detachment, cavitations, and cysts. Among these 17 cases, 12 had both ultrasound changes and cavitation. In the last group of three patients (#24, #25, and #26), the pulse acoustic energy was 94 J. The extent of the nodule destruction assessed by pathology of the targeted nodules was 80%, 78%, and 58%, respectively (Table 2).
Discussion
Patients with growing euthyroid benign nodules should be considered for surgery based on compressive symptoms and clinical concern (3). Nevertheless, physicians commonly find it difficult to recommend surgery due to the risks and constraints of thyroid surgery. Medical suppressive therapy with levothyroxine is no longer recommended for routine use due to the adverse cardiovascular and skeletal effects (3). Therefore, recent research studies have suggested that nonsurgical, minimally invasive treatments, including ethanol injection, percutaneous laser, or radiofrequency ablation, might be relevant alternatives for treating symptomatic patients (1,2,5 –10).
Percutaneous ethanol injection has successfully treated cystic nodules (3,10,21 –24), but is no longer recommended for solid benign thyroid nodules (2,3,10,21,25,26). Moreover, ethanol sclerotherapy has some unavoidable drawbacks, including pain, laryngeal nerve palsy, and extraglandular fibrosis that could impede subsequent surgery in case of treatment failure (25). Interstitial laser photocoagulation has been successful for treating benign thyroid nodules (2,27 –30). Studies of percutaneous laser ablation are numerous and have included controlled trials and homogeneous groups of patients (2,31 –36). Lazer ablation has been shown to achieve 45%–60% reductions in nodule size. Radiofrequency thermal ablation, such as the HIFU procedure, leads to nodule destruction by thermal ablation. Baek et al. recently reported that radiofrequency ablation was effective for reducing nodule volume and relieving nodule-related clinical symptoms. The results were compared with those of a similar control group, and spontaneous nodule reduction could be excluded. Nevertheless, the procedure is invasive; it requires an 18-gauge needle or a hook-umbrella needle (6,7,37). Repetitive sessions allow more complete nodular destruction (7). Radiofrequency thermal ablation appeared to be slightly more effective than percutaneous laser ablation, and the adverse effects appeared to be milder than those reported with laser ablation. Nevertheless, both procedures require local anesthesia, several punctures with large needles, a careful preablation assessment of the transthyroid approach for inserting the electrode, and experienced hands with a consensus among multiple practitioners to limit secondary effects. Moreover, it is important to note that both techniques are very operator dependent. They require careful estimations of safety margins between the nodule and the vital structures of the neck for safe insertion of the tips. Precise data regarding safety margins are lacking in most published reports.
In this study, safety profiles were improved by implementing progressive technological developments. To ensure safety in the absence of previous human data regarding HIFU treatment, the first patients received an initial acoustic energy that was one-third of that used in the previous animal trials (19). This safety measure explained the absence, in some patients, of histological evidence of HIFU shots. We tested HIFU efficacy with a DIPAE that increased from 35 to 94 J. To improve the tolerance of HIFU pulses, premedication, and, in some cases, local anesthesia were provided to relieve patient discomfort. Other alternative therapies, such as laser treatment or radiofrequency, caused various degrees of pain for many patients (1,5). In contrast to the secondary effects reported in other alternative treatments, we observed no dysphonia or vocal cord palsy in this study. Moreover, with the latest modified device head, no skin burns occurred.
In nearly half the patients (10/22), the treated thyroid nodule was clearly necrotic subsequent to HIFU. The extent of nodule destruction that could be unmistakably attributed to HIFU varied from 2% to 69% (Table 2). However, this did not include putative lesions (noncoagulative necrosis, hemorrhage, nodule detachment, cavitations, or cyst). Moreover, from the pathologist's standpoint, empty areas could be due to a HIFU effect (cyst formation, cavitation), an artifact, or a pre-existent lesion. When cavitation was considered a HIFU-induced lesion, nodule destruction was observed in 21 out of 22 patients, and the extent of nodule destruction varied from 2% to 80%. For example, in patient #12, no specific lesion changes were observed, but 27% destruction was observed when we included cavitation (Table 2). In patient #23, the correlation with ultrasonography was quite useful: after 15 days, the solid nodule became cystic (Fig. 1).
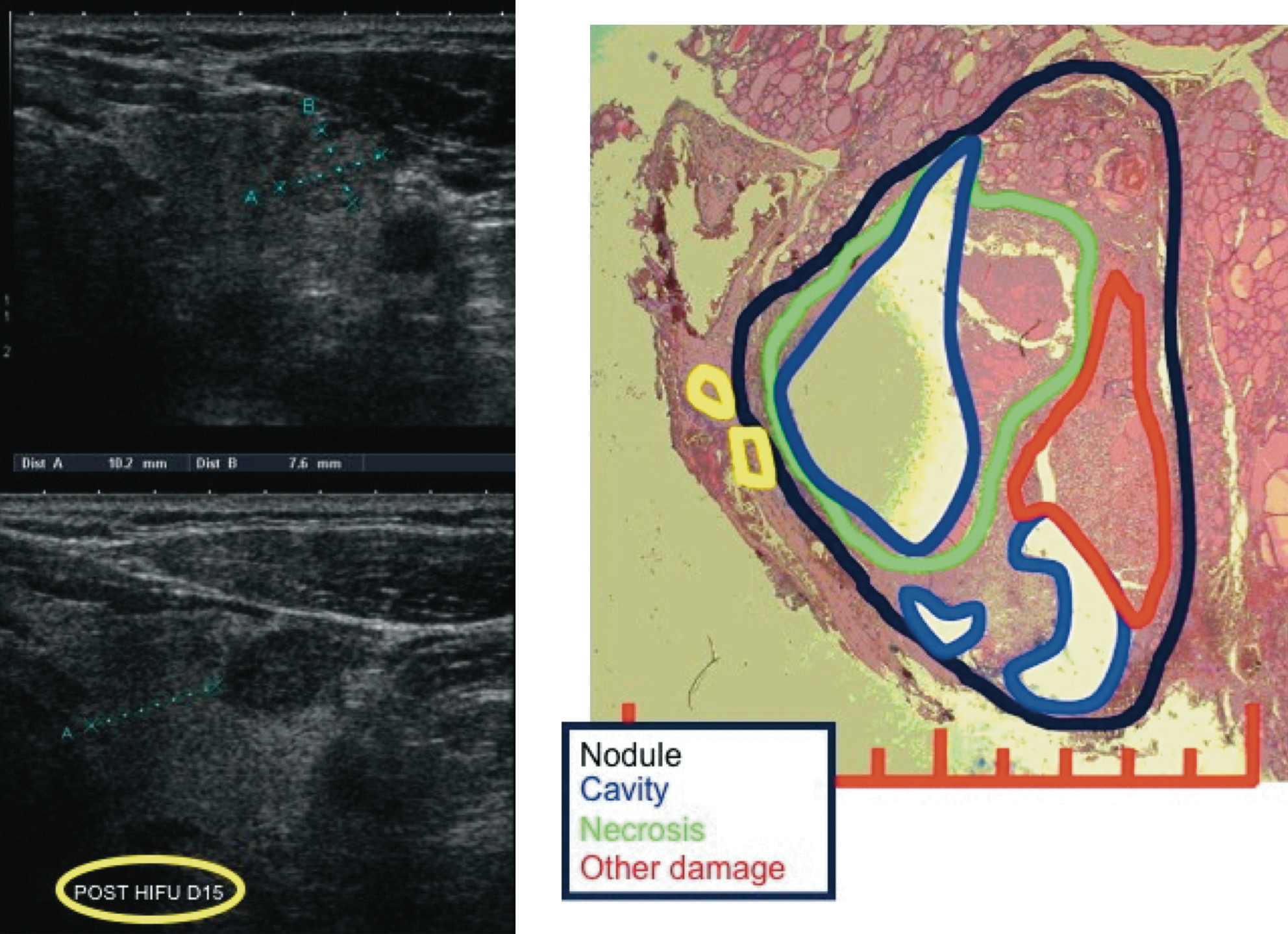
Ultrasonograms before (upper left) and on day 15 (lower left) after HIFU treatment of thyroid nodule tissue. (Right) Within the nodule area (black outline), histological destruction due to HIFU (green outline) is shown separately from destruction due to nonspecific injury (red outline), extranodular HIFU lesions (yellow outlines), and cavitation (blue outline). Scale represents 1 cm. Tissue section is from patient #23.
For patient #5, the treatment zone was larger than the small nodule; this explained the extranodular lesions observed histologically.
In the last group of three patients (#23, #24, and #25), with a DIPAE of 94 J, the extent of PLAH was 69%, 0%, and 58%, respectively. The ultrasonographic readings showed an enhanced hypoechogenicity and a decrease in vascularization. For patient #24, the pathology readings did not show any typical HIFU lesion (0%) due to the presence of a major cavitation. The baseline sonogram showed an initial solid echostructure of the nodules; the post HIFU sonograms showed that the echostructure had become mixed. Thus, we concluded that the cavitation was attributable to HIFU, and that the total nodule destruction by HIFU amounted to 78% (Figs. 2 and 3). With this interpretation, the targeted nodule destruction for the last group of patients ranged from 58 to 80%.
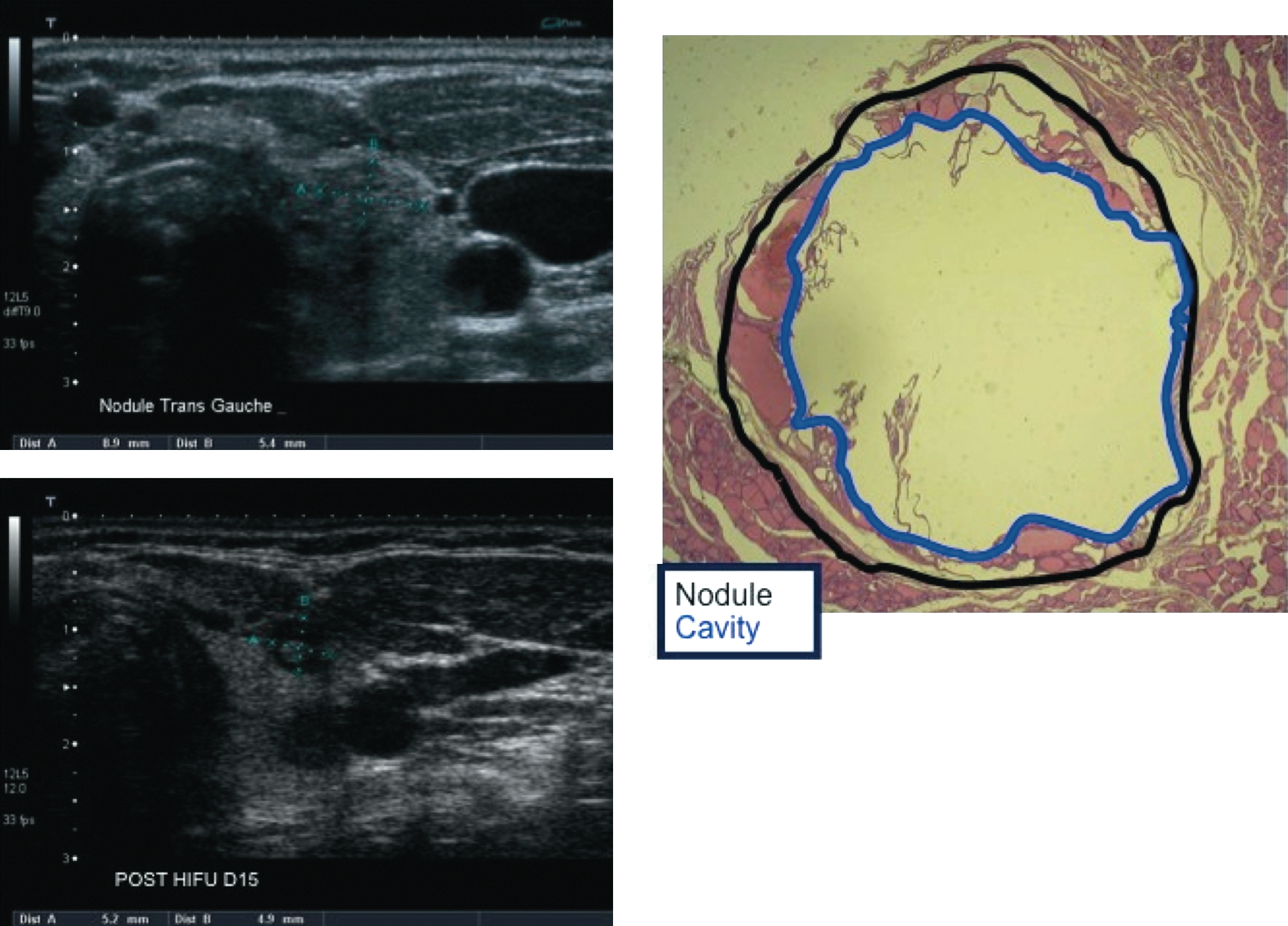
Ultrasonograms before (upper left) and on day 15 (lower left) after HIFU treatment of thyroid nodule tissue. (Right) Within the nodule area (black outline), histological destruction due to cavitation (blue outline) is indicated. Tissue section is from patient #24.
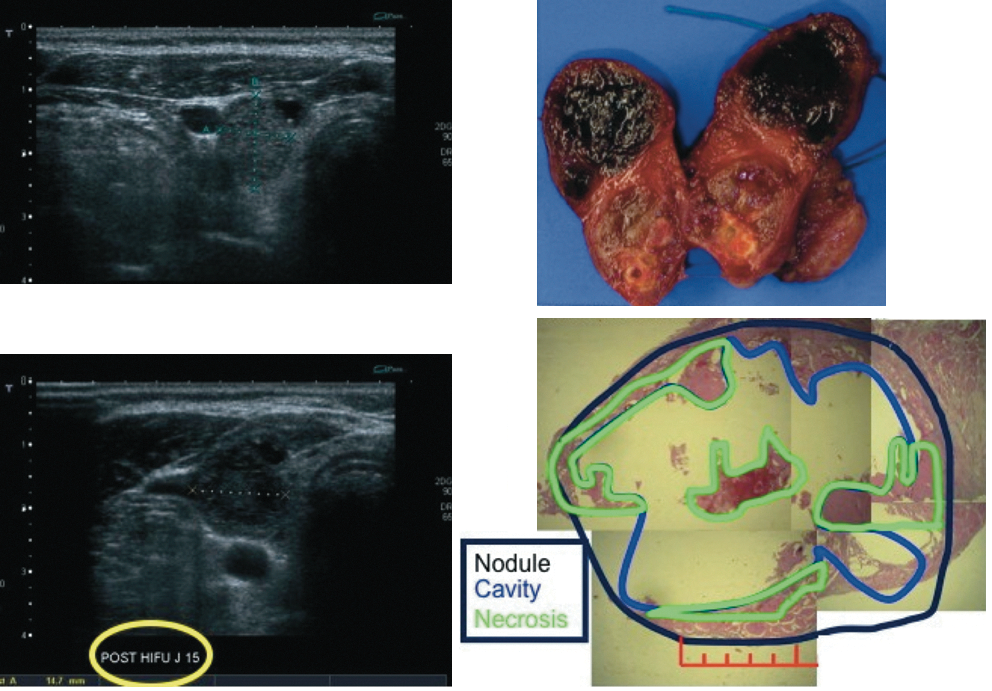
Ultrasonograms before (upper left) and on day 15 (lower left) after HIFU treatment of thyroid nodule tissue. (Right) Macroscopic (upper right) view of necrotic tissue (black regions). Microscopic (lower right) histological analysis indicates the percentage of destruction within the nodule area (black outline) caused by necrosis (green outlines) and cavitation (blue outlines). Scale represents 1 cm. Tissue section is from patient #25.
However, the histological assessment after 2 weeks is only preliminary evidence of the HIFU efficacy. The evolution of the lesions over time can include further hemorrhage, cavitation, or cyst formation in the areas neighboring the typical HIFU lesions. These may also be of interest for assessing the global decrease of the thyroid nodule. It has been shown with other HIFU applications that the targeted tissue will collapse to a thin layer of scar tissue (20).
We tried to identify several potential factors related to the patient and/or technical parameters that may alter the efficacy of the HIFU procedure, as follows:
Regarding the patient: • A large nodule volume makes the HIFU treatment longer and more difficult, • Echostructure, vascularization, and type of adenoma: HIFU results in this study were not precluded by these factors; further studies on a larger scale are needed to identify ultrasonographic factors predictive of successful HIFU effects, • Thyroglobulin plasma level; the expected short-term increase after HIFU treatment due to thyroid tissue destruction, followed by a decrease to baseline was observed in some patients; however, it did not correlate to the energy level or to the extent of tissue necrosis.
Regarding the technical parameters: • The energy delivered to thyroid tissue. Low energy incurred no lesions, and nodule destruction was near complete with high energy (last 3 patients). • The location of the nodule. Deep nodules require higher pulse acoustic energies to overcome the absorption by tissues between the skin and the nodule.
In addition, we noted some limitations in making precise assessments of HIFU efficacy: • Mapping and targeting: Some results may be underestimated due to nonoptimal mapping and targeting of the nodule and difficulties in precisely assessing the area of the nodule that had been treated. • The extent of the treated area: when the HIFU was targeted at the center of the nodule, we noted that the destruction of the vascularizing artery caused complete necrosis and thrombosis of the central feeding vessel (patient #1; Fig. 4). Therefore, failure or sub optimal efficacy may result when the whole nodule is not targeted or when the energy level is limited, because this may allow persistence or re growth of the nodule. • Lidocaine/epinephrine was injected into the nodule for the last 8 patients. This could have caused dissipation of thermal energy due to the locally induced edema. Conversely, local vasoconstriction may have decreased the energy required for ablation and theoretically may have enhanced the effect of the focal temperatures generated per joule per shot. Theoretically, this may be considered a form of adjunctive therapy. • Evaluation of the nodule surface rather than nodule volume may have introduced a bias. • Tissue handling, preparation, and cutting might give rise to artifacts. Homogeneous nodule slicing was difficult; thus, the slide evaluations were based on the zone of necrosis from the central nodule slice.
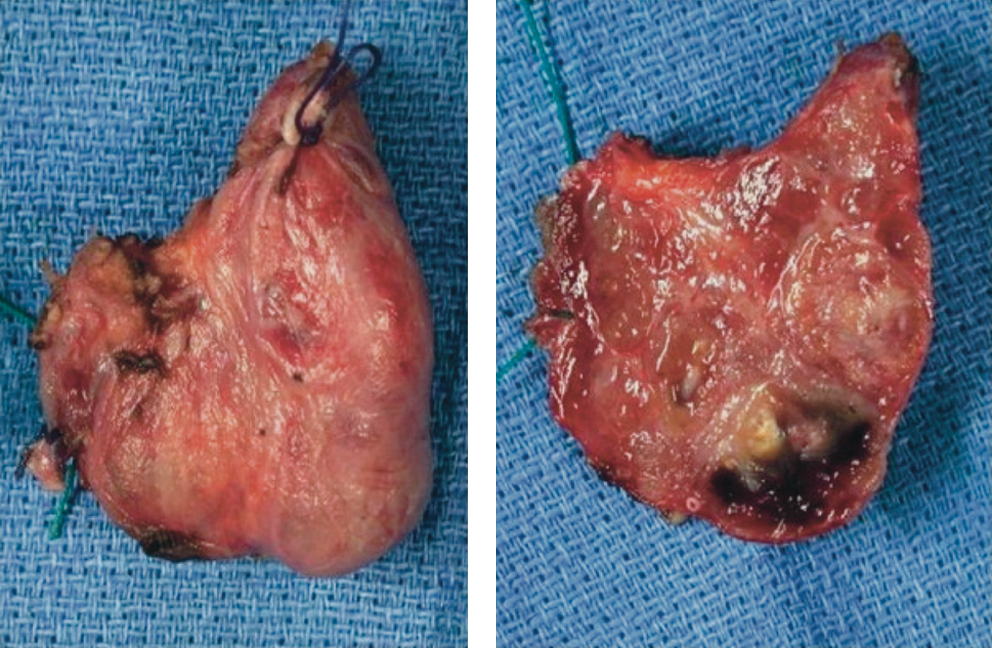
Macroscopic evidence of HIFU ablation. (Left) Left lobe; (Right) same specimen divided in half. Tissue necrosis is evidenced by the black tissue. Tissue section is from patient #1.
This study was the first to show a dose-response relationship for HIFU of thyroid tissue. We demonstrated that HIFU treatment was suitable for single thyroid nodules and it induced reproducible, clinically relevant lesions with irreversible cell damage in an appropriate application time. Moreover, the HIFU procedure does not require insertion of large needles. Compared with radiofrequency and laser ablation, HIFU required smaller safety margins, which should lead to a more complete treatment, and it was less operator dependent, because the energy was delivered in shots of a more precise calculated volume.
Conclusions
The preliminary results from this first human feasibility study indicated that HIFU represents an interesting minimally invasive alternative treatment for thyroid nodule destruction. At the present time, and due to the small number of patients treated, it is difficult to compare HIFU treatment with other alternatives, such as nodular destruction by laser, ethanol injections, or radiofrequency. However, the HIFU treatment is totally extracorporeal and easily repeated when necessary.
Our results indicated several factors that could be considered for improving the HIFU technique, including patient selection, preoperative localization of the nodule, treatment-targeting assessments of the volume treated, and duration of follow-up. A better understanding of the factors that influence HIFU-induced tissue destruction and an improvement in preoperative assessments with imaging techniques may lead to an improved outcome.
Footnotes
Acknowledgment
The authors thank Francoise Arnaud for her assistance with this study.
Disclosure Statement
INSERM and Theraclion SAS have supported this study. The authors declare that there is no conflict of interest that could prejudice or jeopardize the impartiality of the research reported.