
Abstract
Background:
Intramedullary spinal cord metastasis (ISCM) is an uncommon complication of malignancy. ISCM from thyroid cancer is extremely rare, only a few cases had been reported and most were found at autopsy. Here we report a patient with progressive lower leg weakness due to ISCM from papillary thyroid carcinoma who had a good response to surgery.
Patient Findings:
A 44-year-old woman presented with bilateral lower leg pain in December 2009. She underwent a total thyroidectomy in 1997 because of large mass in the right neck, which was diagnosed as papillary thyroid carcinoma. She had repeated I-131 therapies, but brain metastasis developed in 2002. When she was admitted, lower leg pain and weakness progressed rapidly. We performed magnetic resonance of the spine and whole-body fluorodeoxyglucose (FDG)-positron emission tomography scan, which demonstrated a 2×6 cm intramedullary mass enhanced by gadolinium with FDG-uptake. She underwent emergency laminotomy with subtotal tumor removal. Pathology revealed metastatic papillary thyroid carcinoma. After the emergent operation she could walk without help.
Conclusion:
We report a patient with ISCM from papillary thyroid carcinoma. Surgical resection should be considered in patients with ISCM from papillary thyroid carcinoma. Early diagnosis and surgical resection could improve the quality of life and the neurologic deficits.
Introduction
Papillary thyroid carcinoma is considered less aggressive with a slower growth rate and a low prevalence of distant metastasis. The most common metastatic site is the lung; metastases to the central nervous system are much less common. ISCM from thyroid cancer is extremely rare. Only a few cases have been reported and most were found at autopsy (1,3 –5). Here we report an interesting patient with ISCM from papillary thyroid carcinoma who was investigated because of the development of progressive lower leg weakness.
Patient
A 44-year-old woman presented in December 2009 with a 2-month history of lower back pain and tingling sensation in both legs. She had had total thyroidectomy in 1997 because of large mass in right neck that originated from the thyroid. There was extension to the mediastinum, compression of the trachea, and encasement of the right subclavian, common carotid, and innominate arteries. Histologic examination revealed papillary thyroid carcinoma. In a preoperative chest radiography, small multiple lung nodules were found.
She received two treatments with 7.4 GBq 131-I. Subsequently post-therapeutic whole-body scans showed uptake by lung nodules, the lymph nodes in the lower neck, and the mediastinum. Subsequently, diagnostic whole-body scan and Tc-99m-MIBI SPECT did not show evidence of residual carcinoma. She was maintained on levothyroxine.
In 2002, whole-body fluorodeoxyglucose (FDG)-positron emission tomography (PET) scan showed multiple small focal hypermetabolic lesions in the lower lobes of both lungs and the mediastinum. She additionally underwent three treatments with 7.4 GBq 131-I. Post-therapeutic whole-body scan showed persistent areas of uptake in the lung and mediastinum. Moreover, focal increased uptake at right parieto-occipital region appeared in the post-therapeutic whole-body scan. This was considered to be a metastasis of papillary thyroid carcinoma in the skull.
Brain metastases were diagnosed in November 2008. She underwent surgical excision of the metastatic nodule in right parietal lobe, gamma-knife surgery to the cerebellar mass, and whole brain radiotherapy. However, MR of brain in July 2009 still showed variable sized multiple peripheral enhancing nodules in both cerebral hemispheres.
In October 2009, she felt lower back pain and experienced symmetrical lower leg weakness. Lumbar spine radiography showed no abnormal findings. After 2 months, her leg weakness slowly progressed and she had fecal incontinence. On neurologic examination, power in both lower legs was decreased to 3/5. Deep touch sensibilities and anal tone were also diminished. MR of spine disclosed a 2×6 cm intramedullary mass at T12-L2, which had slightly low intensity on T1-weighted images and focal high signal intensity in T2-weighted images with gadolinium enhancement (Fig. 1). Whole-body FDG-PET scan showed a hypermetbolic lesion in T12-L2 spinal canal (Fig. 2). Cytology of cerebrospinal fluid showed only atypical cells.
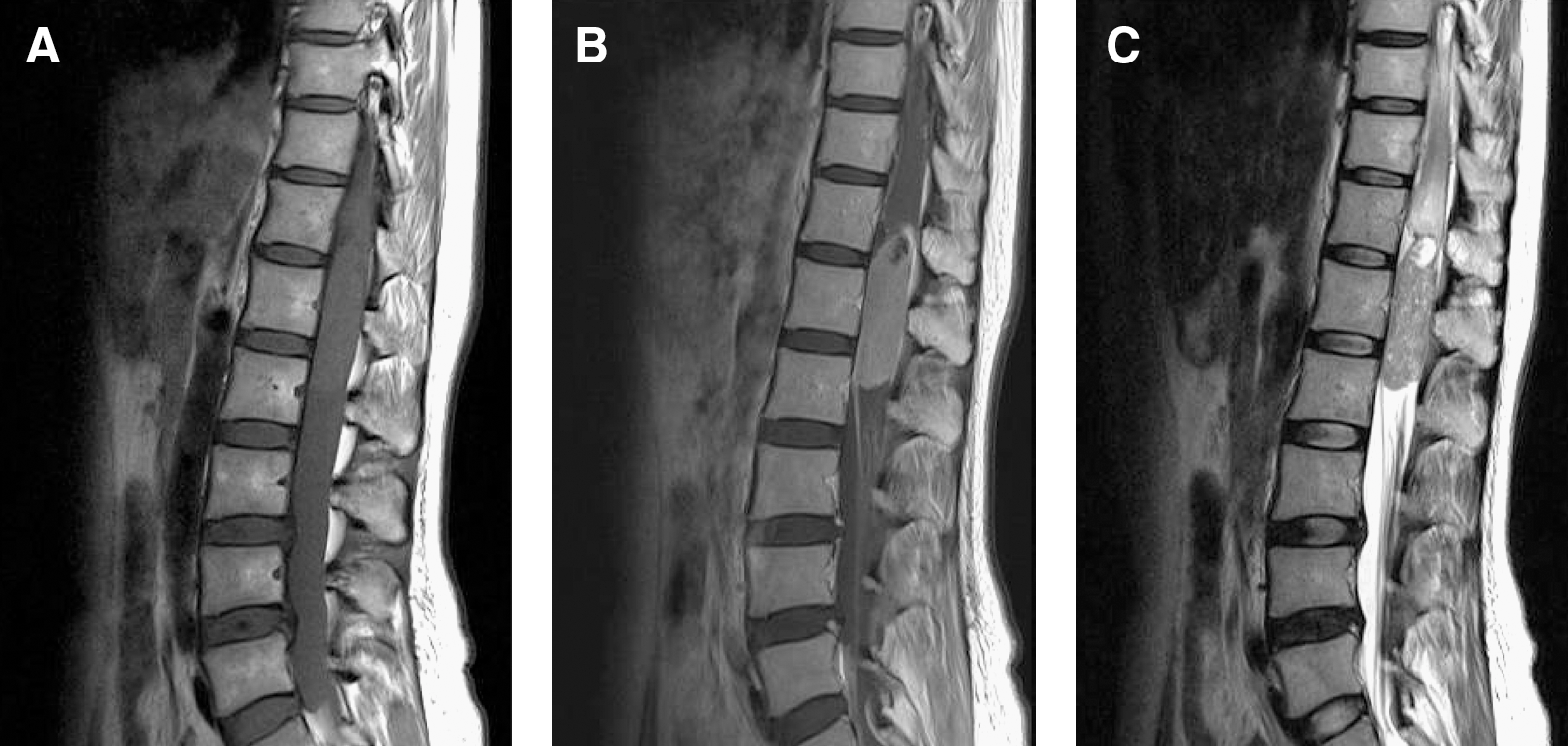
Magnetic resonance of spine shows a 2×6 cm intramedullary mass, enhanced and associated with edema of the thoracic spinal cord.
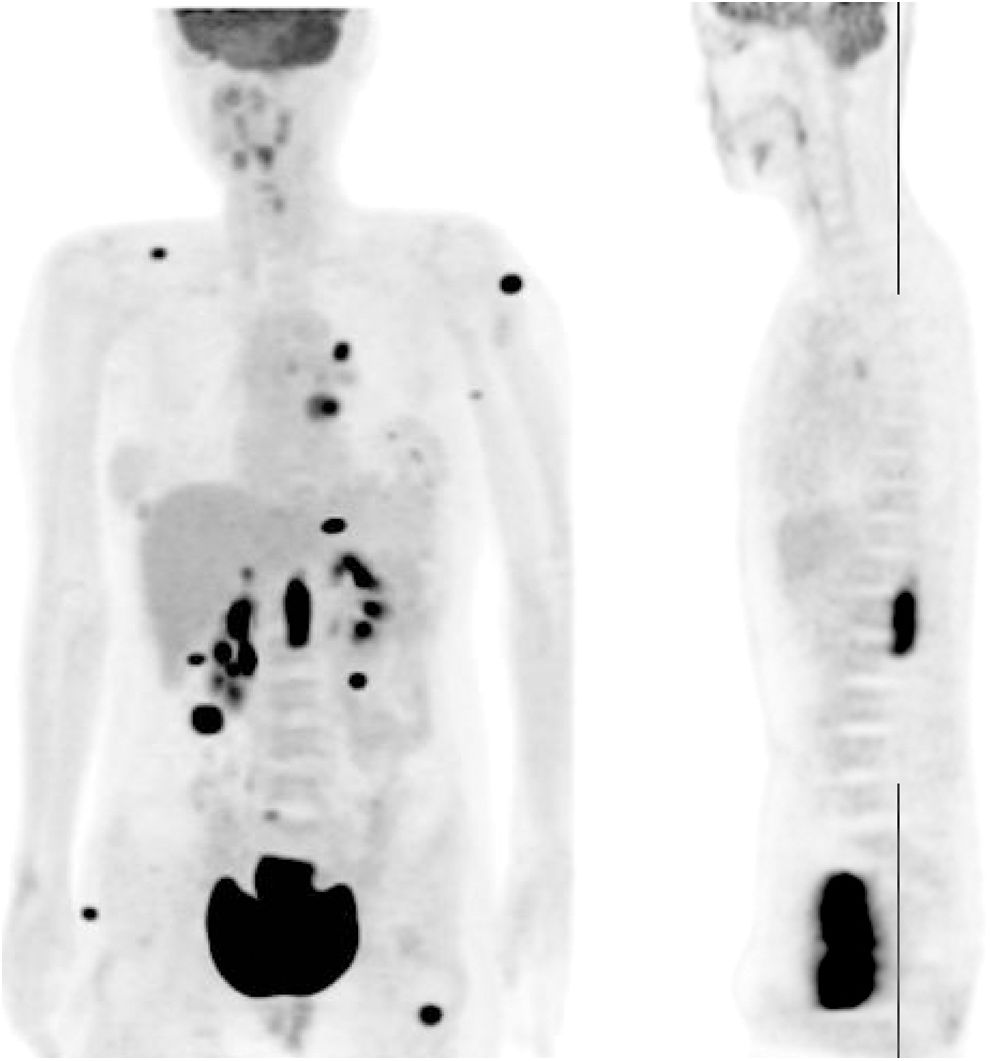
Whole-body fluorodeoxyglucose/positron emission tomography image reveals hypermetabolic lesion in the spinal canal from T12 to L2 level. (SUVmax 10.9).
An emergent laminotomy with subtotal removal of the tumor was performed. The tumor was grayish and not well encapsulated, and had mild vascularity. Histological diagnosis was reported as metastatic papillary thyroid carcinoma (Fig. 3). External beam radiotherapy to spine was also performed (3750 cGy, 15 fractions). She was able to walk without help about 1 month after the operation. In April 2011 she was alive, this being 15 months after diagnosis of ISCM. She has been taking sorafenib 400 mg twice a day. However, the disease continues to progress.
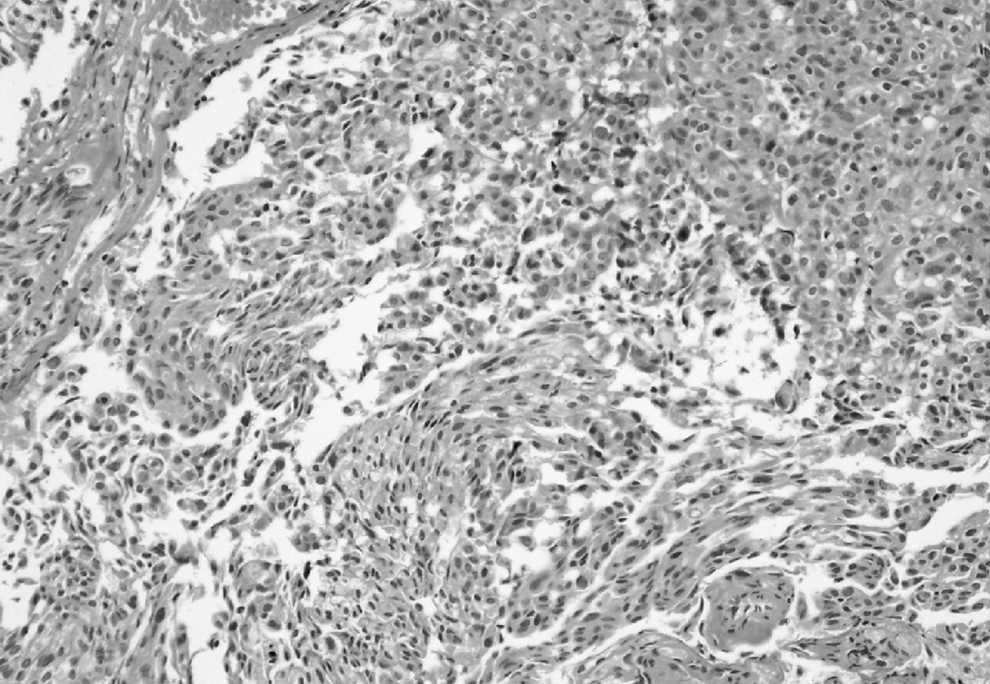
Pathology of spinal cord tumor (hematoxylin and eosin stain, ×400).
Discussion
ISCM is a rare complication of cancer. In general, the presence of ISCM means extensive and advanced systemic malignancy. Thus, at the time of diagnosis, most patients have systemic, including brain, metastases (1,3). ISCM occurs by hematogenous dissemination and can develop at every level of the spinal cord. Weakness is the most frequent symptom. Sensory loss, urinary incontinence, and Brown-Sequard syndrome are the other developments. The neurologic deficit is a prognostic indicator (6,7). The duration of symptoms at the time of diagnosis ranges from 3 days to 18 months.
Gadolinium MR imaging is the most helpful and sensitive study to identify ISCM. T2-weighted images show high intensity signal that is due to the edema associated with metastasis. The gadolinium enhancement helps distinguishing of tumor margins from the edema. FDG/PET scan is not appropriate for the detection of brain metastases because of high glucose uptake in the normal brain, but it is useful in the diagnosis of ISCM by showing metabolic activity (3,8).
Optimal treatment of ICSM remains controversial; there are no definite guidelines. In general, conservative approaches such as external beam radiation with concomitant corticosteroids are preferred. They slow disease progression and decrease pain; the response to radiation treatment is poor when paraplegia develops (1,3,6). Surgery is often avoided because it is not considered curative, or due to the poor general medical condition of the patients and their increased surgical risks. Kalayci et al. reviewed 138 cases of ISCM in the literature. Surgical resection was performed in 32 patient. None of them developed new neurological deficits after surgical treatment and partial neurological improvement was achieved in 66%. The median survival was 9.4 months in the surgically resected group. This was nearly two times longer than the conservatively treated group (3).
Patients with ISCM have a very short life expectancy with a median survival of 3 to 4 months from the time of diagnosis. However, one patient with ISCM from papillary carcinoma survived for 2 years after surgical resection of the tumor (4) and the patient presented here has been alive for >15 months. Gasser et al. reported that the histological composition of the tumor was the only determinant of patient survival (9). Surgical resection should be considered in patients with ISCM from papillary thyroid carcinoma as those patients usually survive longer than those with other malignancies.
In conclusion, ISCM is an uncommon, deteriorating complication of malignancy and a neurosurgical emergency. Early diagnosis and early surgical resection likely reduce the neurologic deficits and improve the quality of life.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.