
Abstract
Background:
Acute suppurative thyroiditis (AST) is a rare, life-threatening thyroid infection characterized by a tender neck mass and fever. As these features are shared with self-limited subacute thyroiditis (SAT), it is important to differentiate between the two disorders.
Patient Findings:
We report a case of AST in a 21-year-old woman who presented with steadily worsening throat pain for 3 weeks, a tender left neck mass, and thyrotoxicosis. She was initially given prednisone for treatment of presumed SAT but then it acutely worsened. Fine needle aspiration yielded pus on gross examination, and she required intubation and emergent surgical drainage to maintain her airway. Culture of the abscess isolated Streptococcus F and Porphyromonas, a gram-negative intracellular anaerobe not previously reported to cause AST. She improved quickly after surgery, developed transient hypothyroidism that did not require treatment with thyroid hormone, and is currently euthyroid. An abnormal piriform sinus fistula was identified on the left using an esophagram.
Summary:
AST may be difficult to clinically differentiate from SAT. Fine needle aspiration revealing pus, culture yielding bacteria or fungi, abscess on ultrasonography and computed tomography, and left-sided predominance are important in the diagnosis of AST.
Conclusions:
AST should be considered in any patient with SAT who does not rapidly improve following institution of steroids. Further, the presence of thyrotoxicosis does not eliminate AST as an initial diagnosis.
Introduction
Patient
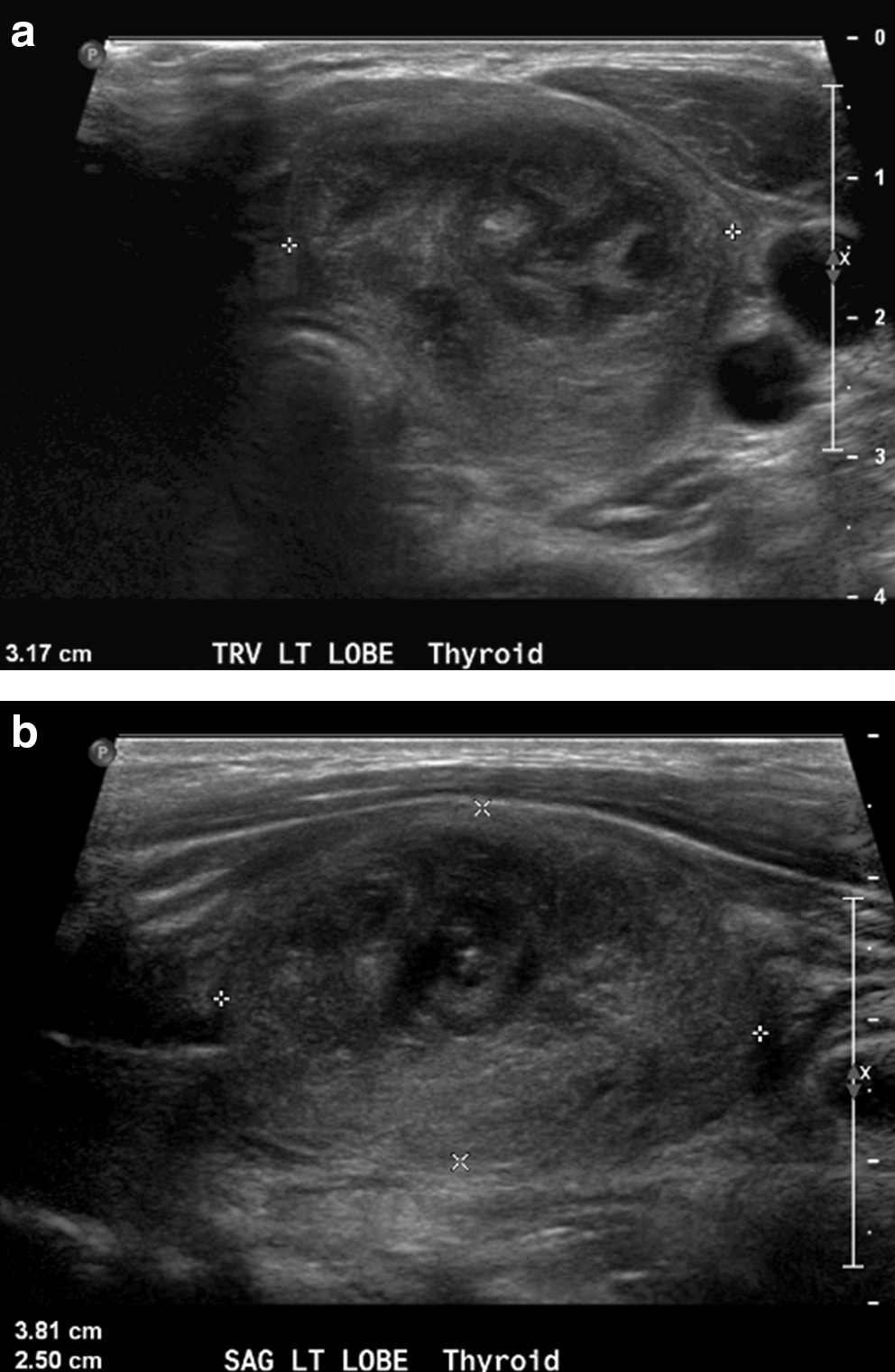
A 21-year-old woman was referred to our clinic for steadily worsening throat pain for 3 weeks. She reported odynophagia, dysphagia, occasional tiredness, palpitations, and alternating heat and cold intolerance. Left neck swelling accompanied her throat pain and increased gradually. She initially presented to an urgent care clinic with similar symptoms 2 weeks prior and was advised to take naproxen 500 mg by mouth twice daily, which was ineffective in controlling her symptoms. She reported developing a fever to 38.9°C 9 days previously, but had subsequently become afebrile. Physical examination, when we saw her, revealed a pulse of 112 beats per minute and a tender left thyroid mass measuring 3×3 cm without erythema. Lab tests were significant for thyroid stimulating hormone (TSH) of 0.1 μIU/mL (normal range, 0.35–5.5), free thyroxine 1.74 ng/dL (normal range, 0.85–1.82), white blood count (WBC) 11,200/μL (normal range, 4500–11,000), absolute neutrophil count (ANC) 8400/μL (normal range, 1800–7700), erythrocyte sedimentation rate (ESR) of 65 mm/h (normal range, 0–20), and thyroid peroxidase antibodies 404 international units/mL (normal range, <35). Thyroid ultrasound revealed a hypoechogenic, heterogeneous nodule measuring 3.8×3.2×2.5 cm (Fig. 1) and numerous enlarged lymph nodes measuring up to 1.1×0.6 cm. The right thyroid lobe measured 4.8×1.5×1.5 cm in size and was homogeneous. Thyroid I-123 uptake was 0.6% at 24 hours (expected 15–30%). Radiotracer on thyroid I-123 scan was faintly visualized in the right lobe, whereas no uptake was visualized in the left lobe. The patient was diagnosed with SAT and started on prednisone 40 mg by mouth once daily, which she took that evening with marked improvement in her symptoms.
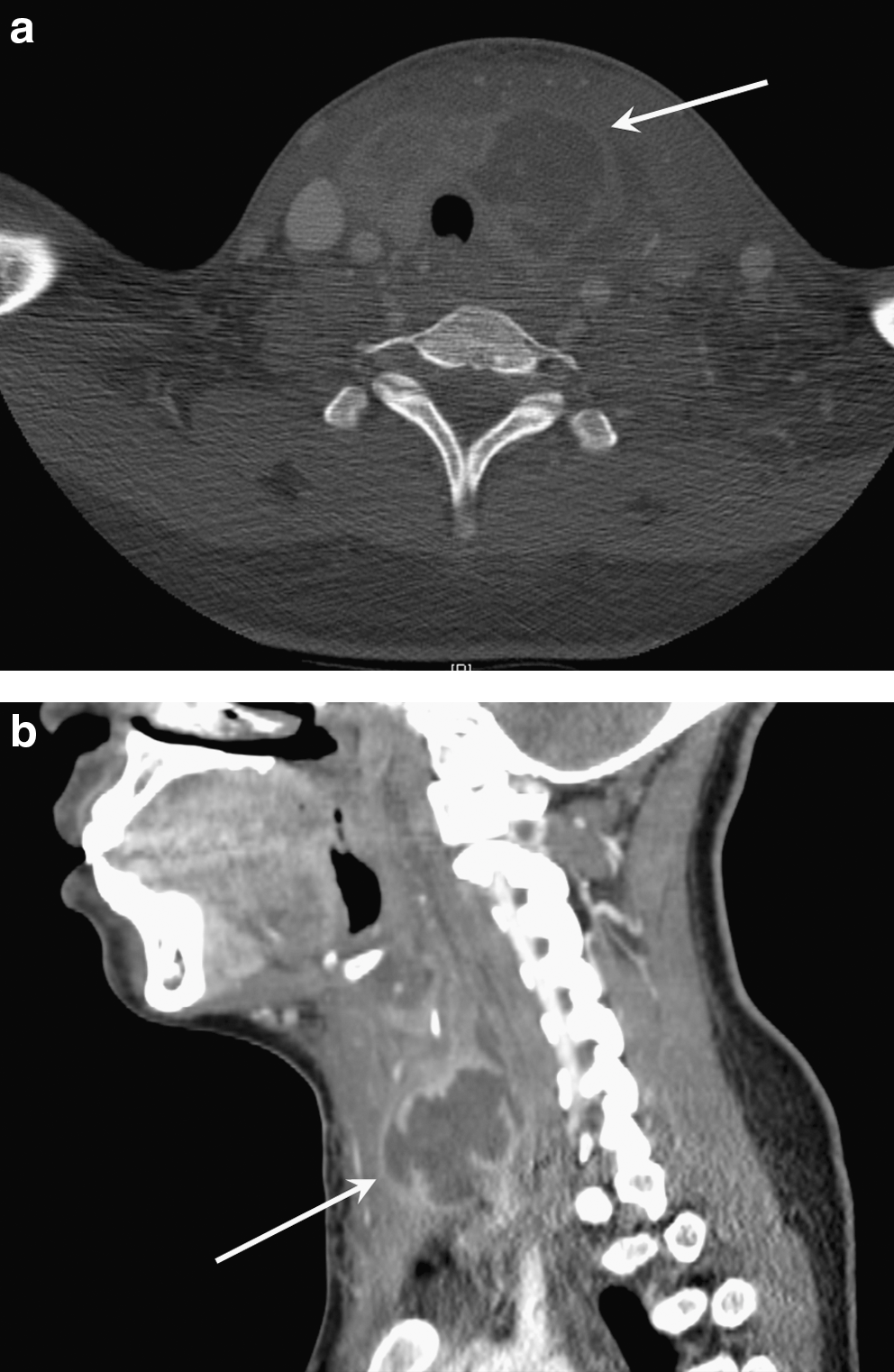
The next day (day 1), she took prednisone in the morning and felt better. However, her pain and dysphagia rapidly increased that night. On day 2, she could no longer tolerate fluids by mouth, for which she presented to the emergency room. Temperature was 40°C, pulse was 139 beats per minute, blood pressure was 125/69 mmHg, and respiratory rate was 18 per minute. On physical exam, she was drooling, had limited range of motion of her neck, and was severely ill appearing. A computed tomography (CT) scan of the neck with contrast revealed replacement of the left thyroid lobe with an abscess measuring 4.0×3.9×3.4 cm, which extended into the retropharyngeal soft tissues and displaced the trachea to the right (Fig. 2). WBC was 27,100/μL, ANC was 25,200/μL, and ESR was 95 mm/h. Fine needle aspiration of the mass produced pus, which confirmed the diagnosis of AST, and was sent for culture and sensitivity. Despite treatment with prednisone 40 mg by mouth, methylprednisolone 16 mg IV, ketorolac 30 mg IV, clindamycin 600 mg IV, and acetaminophen 650 mg by mouth, all given by the emergency medicine team, she appeared increasingly more toxic. Emergent incision and drainage of the abscess was performed, during which an indentation was noted along the lateral aspect of the left piriform sinus. The patient remained intubated postprocedure due to pharyngeal swelling. Dexamethasone 10 mg IV every 8 hours for 2 days was ordered by the ear, nose, and throat surgeons to reduce pharyngeal swelling. Vancomycin 600 mg IV every 6 hours and piperacillin/tazobactam 3.375 g IV every 6 hours were initiated.
On day 5, the patient was extubated. Dexamethasone was reduced to 10 mg IV every 12 hours and then stopped. Pathology from the incision and drainage revealed microabscesses and necrotic tissue. Cultures of the abscess grew Streptococcus F and Porphyromonas, a gram negative anaerobe. Her antibiotic regimen was changed to metronidazole 500 mg by mouth three times daily and amoxicillin-clavulanate 875–125 mg by mouth twice daily on discharge, which was continued for another 25 days after discharge. Human immunodeficiency virus testing was negative. Esophagram on day 26 revealed linear extension of contrast inferiorly from the left piriform sinus, consistent with an abnormal left piriform sinus tract (Fig. 3). TSH rose and then declined, while free thyroxine indices normalized, during 105 days of follow-up (Fig. 4). She is currently euthyroid and has not required thyroid hormone replacement.

Esophagram (arrow points at contrast in the abnormal left piriform sinus).
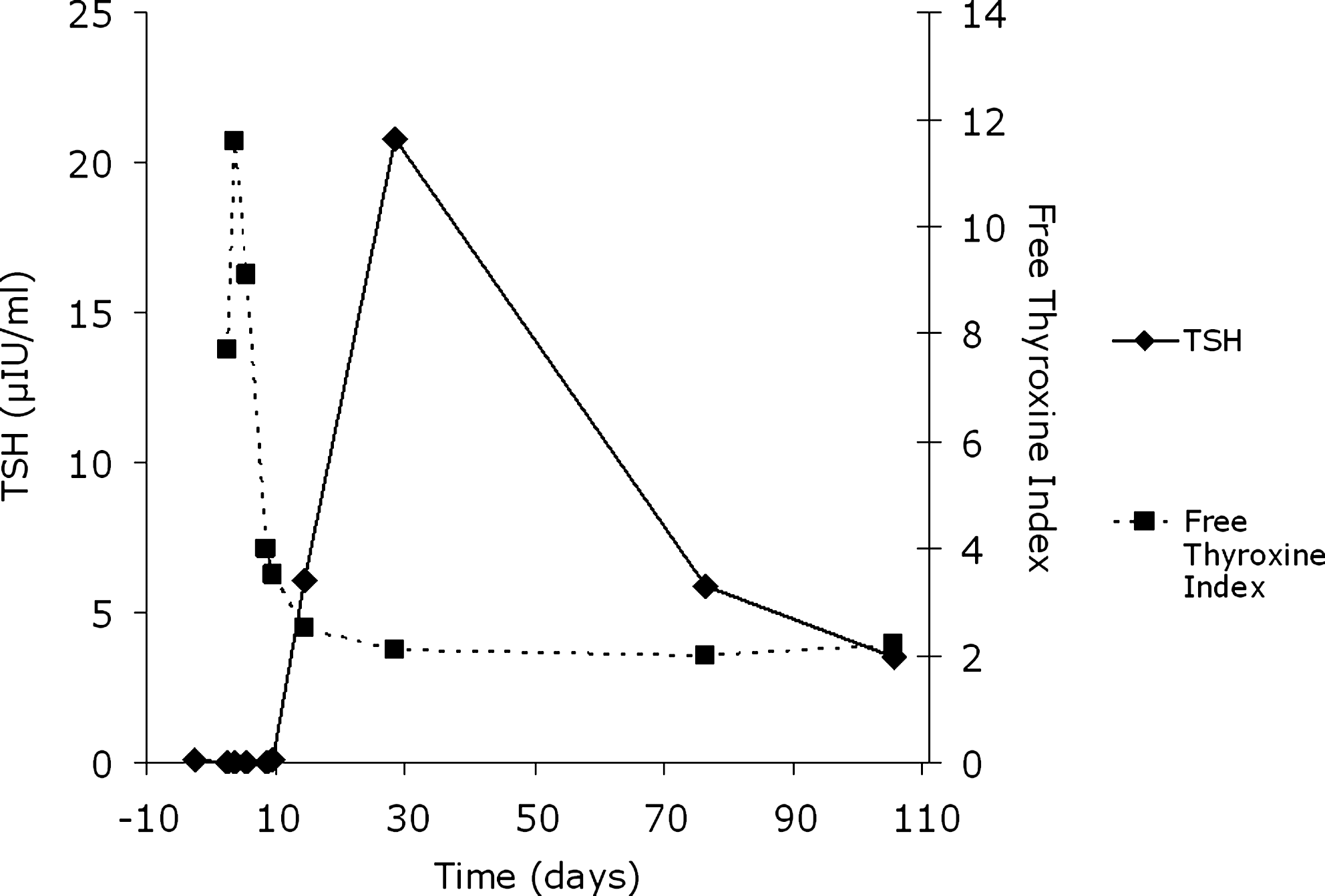
Thyrotoxicosis, hypothyroidism, and then normalization of thyroid function in acute suppurative thyroiditis.
Discussion
The majority of patients presenting with AST are euthyroid. In a review of 95 reported cases of AST, thyrotoxicosis was noted in 12% and hypothyroidism in 17% (3). Similarly, a case series of 13 patients with AST described thyrotoxicosis in only one patient (8%) (4). In contrast, thyrotoxicosis is much more common with SAT. An undectable TSH has been reported in 52% and 65% of SAT patients within 7 and 30 days of neck pain, respectively (5). This patient was thyrotoxic on presentation, which contributed to the initial of diagnosis of SAT. She then became hypothyroid, with normalization of thyroid function tests after ∼3.5 months of follow-up (Fig. 4). This pattern is also typical of SAT. It is possible that the severity of her infection contributed to her rapid thyroid hormone shifts. Nonetheless, the severity of her infection did not impair her ability to produce thyroid hormone during convalescence.
The pathogens responsible for this patient's AST are noteworthy. Porphyromonas is a gram-negative intracellular anaerobe, colonizes the gingival epithelium, and causes periodontitis (6). Despite being part of the oral flora, this is the first report of AST due to Porphyromonas. Streptococcus F, also isolated from this patient, is a type of viridans Streptococcus and consists primarily of the species milleri (7). As part of the oral flora, Streptococcus F has a propensity to form head and neck abscesses and is known to cause AST (7,8).
Despite initial improvement in her thyroidal pain, our patient worsened acutely within 48 hours. A similar deterioration has been reported after treatment with prednisilone (9). Thus, it is important to closely follow patients with presumed SAT who have been treated with oral steroids and to consider AST as a diagnosis if the patient does not rapidly respond clinically.
While the biochemical confirmation of thyroxicosis was consistent with the initial diagnosis of SAT, our patient demonstrates that this was misleading. Features that distinguish between AST and SAT are shown in Table 1. In particular, pus on fine needle aspiration, bacteria or fungi on culture, left-sided predominance, and abscess on ultrasonography and CT scan are important in distinguishing between AST and SAT. Ultrasound images of this patient featured a hypoechoic and heterogeneous left thyroid gland. Although these images are not classic for SAT, they are compatible with the diagnosis (1,5). In retrospect, the ultrasound images could also be attributed to an evolving abscess, and CT later clearly featured a left thyroid abscess. Fine needle aspiration of pus was the key to arriving at a definitive diagnosis for this patient. Younger age may influence the diagnosis because SAT is more common in older patients. One review reported the average age of 852 patients with SAT to be 48 years old (5). Absence of radioiodine uptake in the area of suppuration on nuclear scintigraphy, as noted for this patient, is typical of AST (1). However, low radioiodine uptake occurs in SAT as well (1).
CT, computed tomography.
A piriform sinus fistula is present in >95% of patients with AST, including this patient, and results from a congenital malformation of the ultimobranchial body (1,10). The ultimobranchial body gives rise to C cells of the thyroid and derives from the caudal portion of the fourth pharyngeal pouch (10). Because development of the ultimobranchial body is restricted or absent on the right side, AST rarely involves the right thyroid (10).
In summary, we report a case of AST presenting with thyrotoxicosis in which the patient clinically decompensated after treatment with oral steriods. This case suggests that AST should be considered in any patient with SAT who does not rapidly improve following the institution of steroids. Further, the presence of thyrotoxicosis does not eliminate AST as an initial diagnosis.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.