
Abstract
Background:
Pleuropulmonary blastoma (PPB) is a rare and aggressive intrathoracic neoplasm that is associated with other dysplastic or neoplastic conditions. The prognosis, especially of type II (cystic and solid) and type III (solid) PPB, is poor. High-dose chemotherapy (HDC) and hematopoietic stem cell transplantation (HSCT) have been attempted to improve survival rates. We report the development of follicular thyroid carcinoma in a girl who was treated at a young age for PPB.
Summary:
A 23-month-old girl was evaluated for a clinical diagnosis of pneumonia and was found to have a mass in the left lung that grew rapidly. It was removed and diagnosed as a PPB. At the age of two, she was referred to our hospital for further treatment. She received adjuvant chemotherapy for 6 months but developed a recurred mass in her back at 4.3 years of age. After removal of the mass, she was given a salvage chemotherapy followed by HDC and HSCT but not radiation treatment between 4.4 and 4.9 years of age. At the age of seven, after 2 years without treatment, she presented with multiple thyroid nodules in both lobes that steadily grew over the next 2 years. At the age of nine, she underwent total thyroidectomy, which revealed an invasive follicular carcinoma. She remained without clinical evidence of thyroid cancer for one year since the surgery. Radiation therapy was not administered because of the concerns of causing another malignancy. A literature search combined with the present case indicated that, of the five living patients who had been treated with HDC and HSCT, three developed a follicular thyroid carcinoma.
Conclusions:
The high prevalence (3/5, 60%) of follicular thyroid carcinoma in patients with PPB who were treated with HDC and HSCT is striking. This suggests that, in patients with PPB, either HDC or HSCT contributes to the development of thyroid cancer. Clinicians should be advised of the high risk of thyroid carcinoma occurrence when HDC and HSCT are being contemplated in children with PPB.
Introduction
PPB is associated with other dysplastic or neoplastic conditions (6,7). Adenomas or carcinomas of the thyroid, medulloblastoma, rhabdomyosarcoma, and cystic nephroma have occurred in patients with PPB (6 –9). Two cases of follicular carcinoma of the thyroid occurring after the diagnosis of PPB have been reported (8,10). We report another patient with thyroid follicular carcinoma that occurred after HDC with autologous peripheral blood stem cell transplantation (PBSCT) for PPB. Informed consent was obtained to review the medical records of our patient with PPB according to the regulations of the National Cancer Center Institutional Review Board.
Patient
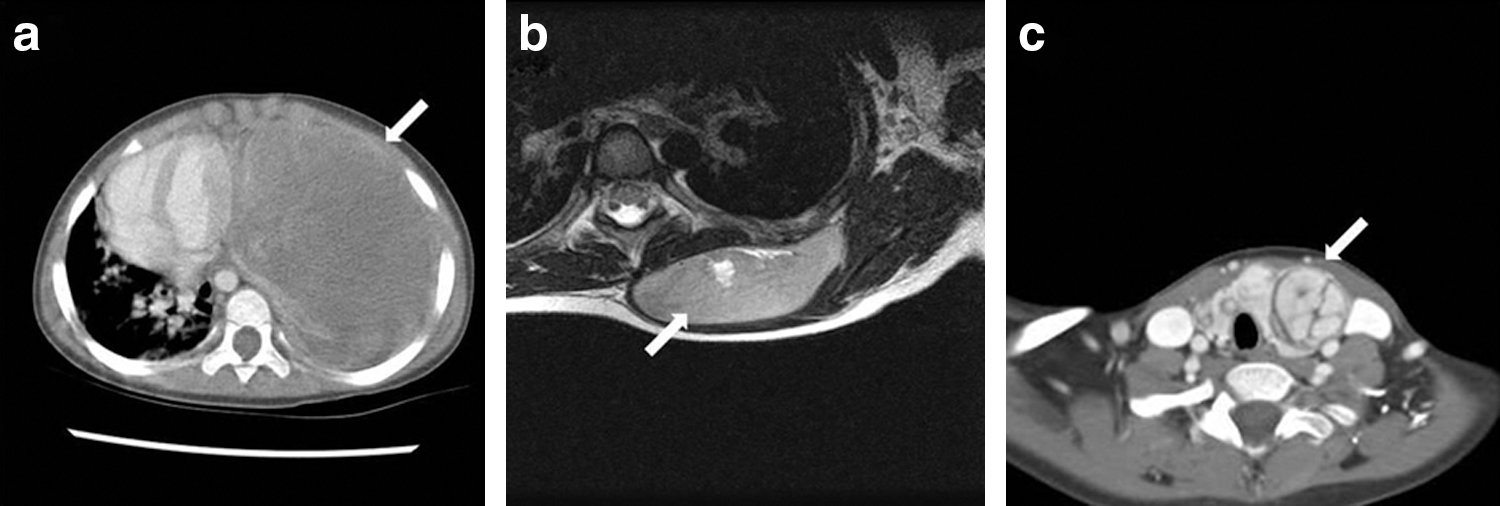
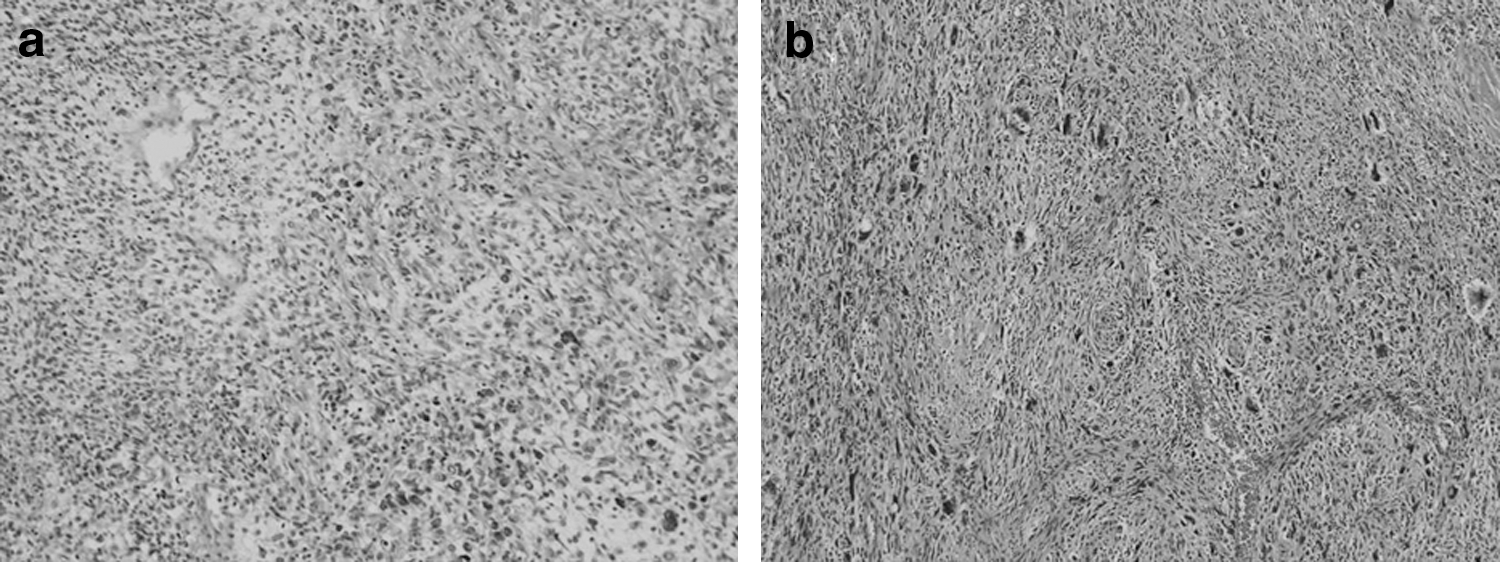
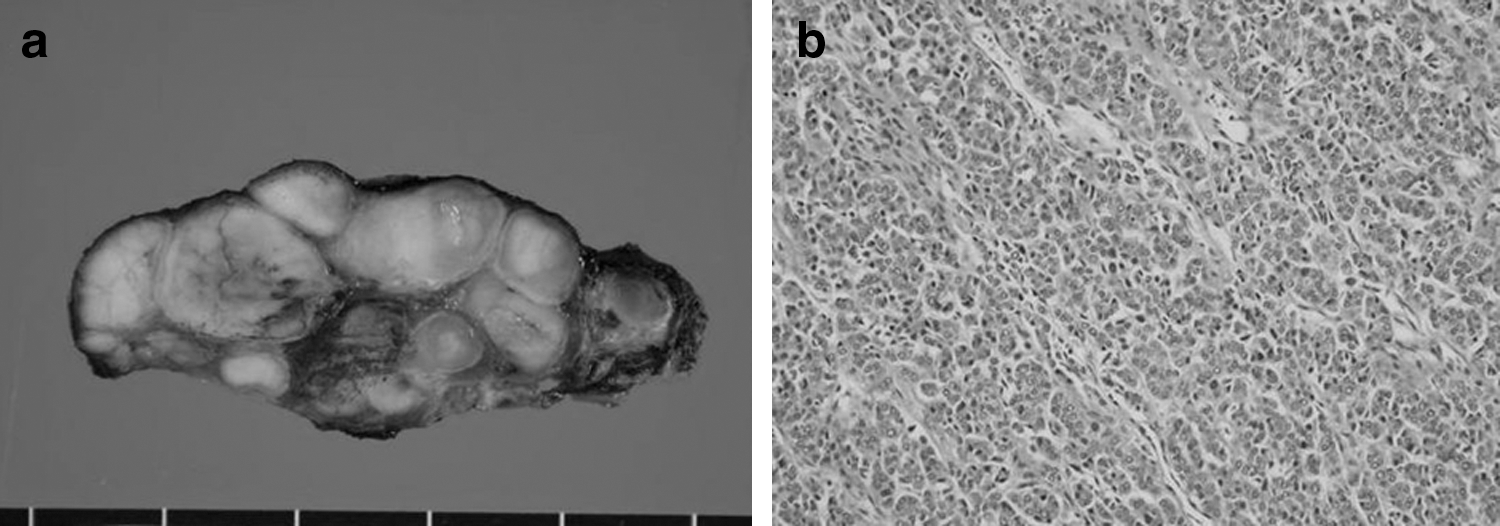
A 23-month-old girl presented with a mass shadow on chest X-ray that was incidentally found during the treatment of pneumonia. The initial chest CT scan revealed a mass with solid and cystic components in her left lung. The mass then grew rapidly, and within one month, occupied the entire hemithorax and caused respiratory difficulty (Fig. 1a). The mass was surgically removed with lingular segmentectomy and near-total pleurectomy. The pathological diagnosis was PPB (Fig. 2a). In January 2003, she was referred to our hospital and received four courses of the Children's Cancer Group (CCG) 6921 regimen (vincristine, actinomycin-D, cyclophosphamide, etoposide, ifosfamide, cisplatin, and adriamycin) over 6 months. Two years later, a 6.6 cm × 3.3 cm-sized mass was found on her left back muscle (Fig. 1b). The mass was completely excised and identified as relapsed PPB (Fig. 2b). The patient underwent five courses of the CCG ICE regimen (ifosfamide, carboplatin, and etoposide) over 5 months, followed by HDC and autologous PBSCT. Melphalan [60 mg/(m2·day) for 3 days], etoposide [200 mg/(m2·day) for 5 days], and carboplatin [350 mg/(m2·day) for 5 days] were used as a conditioning regimen. Two years later, when she was 7 years old, she was found to have a goiter. An ultrasonographic exam revealed multiple heterogeneous iso- and hypoechoic nodules in both thyroid lobes, with the largest one (2.5 cm × 1.2 cm × 3.8 cm) being in the left lobe. Her serum thyroid hormone, thyroglobulin, and microsomal antibody concentrations were within the normal range (triiodothyronine, 156 ng/dL [normal, 90–240 ng/dL]; free thyroxine, 0.98 ng/dL [normal, 0.8–2.2 ng/dL]; thyrotropin, 1.99 μIU/mL [normal, 0.7–6.4 μIU/mL]; thyroglobulin, <20 U/mL [normal, 5.6–41.9 U/mL]; and microsomal antibody, 43.4 U/mL [normal, <100 U/mL], respectively). Fine-needle aspirates showed no evidence of malignancy. Over the next 7 months, however, the mass steadily grew. Serum thyroid hormone, thyroglobulin, and microsomal antibody levels remained within the normal range. Needle aspirates at that time also revealed no evidence of malignancy. One year later, at the age of 9 years, she underwent total thyroidectomy, because thyroid cancer was suspected when the thyroid mass continued to grow (Fig. 1c). Pathology revealed invasive follicular carcinoma (Fig. 3a, b). No lymph node involvement was noted. Radiation therapy was not given because of concerns that it would cause a second malignancy. Tests for P53 and K-RAS aberrations using the PPB specimen did not reveal mutations (data not shown). Eventually, 12 months after her thyroidectomy, the patient was tumor free.
Discussion
Thyroid carcinoma is not uncommon as a secondary malignancy (11 –13). In European countries, 7.5% of second malignant neoplasms in childhood cancer survivors are thyroid carcinomas; most of the primary cancers are lymphoma and leukemia (12). Chemotherapeutic agents and radiation as well as genetic aberrations of primary cancers might play a role in the development of secondary thyroid carcinomas (12 –16). Two cases of thyroid carcinoma have been reported in patients with PPB (8,10). Interestingly, they had several features in common with the present case. All of them were girls below 10 years of age, and none had received radiotherapy. Pathological diagnosis was the follicular type, and most interestingly, all of them had received HDC followed by hematopoietic stem cell transplantation (HSCT) (Table 1).
PPB, pleuropulmonary blastoma; HSCT, hematopoietic stem cell transplantation; RT, radiotherapy; TC, thyroid cancer; auto-BMT, autologous bone marrow transplantation; auto-PBSCT, autologous peripheral blood stem cell transplantation; NA, not available; ND, not done.
There are seven children with PPB in the literature who were treated with HDC and autologous HSCT. Three of them had a relapse culminating in death (4,5,17). Of the remaining four survivors, two later developed thyroid carcinoma (8,10). The other two survived without any reported event up to the time of reports on them, but information on their recent course is not available. Thus, with the present case included, three of the five survivors of PPB who had been treated with HDC and autologous HSCT developed follicular thyroid carcinoma (Table 1). To the best of our knowledge, thyroid cancer in patients with PPB who did not undergo HDC and HSCT has not been reported.
Radiotherapy is a well-known risk factor for the development of thyroid cancer (12). However, all three patients including ours never received radiotherapy. In fact, HDC and HSCT could have played a role in them with regard to the development of thyroid cancer. The EBMT Late Effect Working Party Study reported that the prevalence of thyroid cancer in patients who received HSCT without radiotherapy was increased by 25% compared with the general population, and that young children below 10 years at the time of transplantation were particularly vulnerable to developing thyroid cancer (14). Additionally, they reported that thyroid carcinoma as a secondary tumor was more common in females, and that the follicular type was more frequent after HSCT, whereas papillary thyroid carcinoma was predominant in childhood cancer survivors who received radiotherapy (12,13). Consistent with these findings the present case, and two previous cases, had all of these risk factors (Table 1).
The prevalence rate (3 of 5, 60%) of thyroid carcinoma in patients with PPB who had HDC and HSCT is surprisingly high when compared with the prevalence of thyroid carcinoma in patients with other primary cancers, such as leukemia, lymphoma, and various solid tumors (11,12). The EBMT Late Effect Working Group found only 32 instances of secondary thyroid carcinoma within the EBMT cohort of 68,936 patients who received transplants (14). Thus, it is not plausible that the exceptionally high prevalence of thyroid carcinoma in patients with PPB could be solely explained by the fact that they were treated with HDC and HSCT. A large series published in 1996 reported that 25% of patients with PPB or their young relatives had other dysplasias, benign neoplasias, or malignancies (7). This suggests that PPB itself predisposes to the development of neoplastic disease; furthermore, it seems likely that HDC and/or HSCT act synergistically in patients with PPB to promote the development of follicular thyroid carcinoma. Several mutations have been reported in patients with PPB, including P53 and novel DICER1 mutations (18,19). We did not find mutations of P53 or K-RAS, which are often encountered in patients with thyroid carcinoma (16,20), in our patient. However, there is limited knowledge on the gene abnormalities in patients with PPB, so we have not ruled out gene mutations predisposing to thyroid carcinoma. We do not have any insight into why patients such as ours seem predisposed to follicular thyroid carcinoma, in contrast to the occurrence of papillary thyroid carcinoma as a secondary neoplasm in patients with primary cancers other than PPB.
Conclusions
We report a 9-year-old girl with follicular thyroid carcinoma who had previously had PPB and had been treated for this with HDC and HSCT. In the limited number of reports to date, including this one, there is a surprisingly high prevalence (60%) of follicular thyroid carcinoma in patients with PPB who were treated with HDC and HSCT, suggesting that the latter two treatments predispose patients with PPB to follicular thyroid carcinoma. Clinicians should be aware of this relationship as they consider the best management and follow-up of children with PPB.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.