
Abstract
Background:
Well-differentiated thyroid cancer arising in struma ovarii is rare. The optimal management of this entity remains undefined. Unilateral cystectomy, unilateral salpingo-oophorectomy (USO), or total abdominal hysterectomy with bilateral salpingo-oophorectomy (TAH/BSO), in addition to total thyroidectomy and radioactive iodine (RAI) ablation, have been employed by various groups. We hypothesized that in patients with thyroid cancer arising within struma ovarii, pelvic surgery alone would be sufficient, provided there is no evidence of gross extra-ovarian extension.
Methods:
We review a series of four patients from a single institution and 53 cases from the literature, comparing the extent of treatment and outcomes. Our literature review focused on low-risk patients with struma ovarii confined to the ovary, without evidence of gross extra-ovarian spread or distant metastases. Cumulative recurrence rate was determined by using the Kaplan-Meier method.
Results:
We report the treatment of four patients with well-differentiated thyroid cancer arising within struma ovarii. Patients underwent USO, BSO, or TAH/BSO. One patient underwent prophylactic total thyroidectomy in anticipation of RAI treatment, and was found to have a synchronous papillary thyroid carcinoma. All patients clinically remain without evidence of disease at a median follow-up of 9 (range 0.8–13) years. Treatment strategies in 53 cases from a review of the literature varied. The pooled cumulative recurrence rate of 57 cases with struma ovarii confined to the ovary was 7.5% at 25 years.
Conclusions:
Thyroid cancer arising in struma ovarii is rare. Controversy exists regarding the extent of pelvic resection and management of the thyroid gland. In our series of four patients, all patients are alive without evidence of disease, and the 25-year recurrence rate of 57 cases was low (7.5%), despite a variety of approaches to surgical resection and adjuvant treatment. Extensive pelvic surgery and prophylactic total thyroidectomy to facilitate RAI therapy may be reserved for patients with gross extra-ovarian extension or distant metastases.
Introduction
Well-differentiated thyroid cancer arising in struma ovarii has been reported in fewer than 5% of cases (9,10). Criteria for malignancy are similar to those for thyroid tumors. Features indicative of malignancy include cytologic atypia, nuclear grooves, ground-glass overlapping nuclei, increased mitotic activity, and vascular invasion. Capsular invasion is not diagnostic for malignancy in struma ovarii due to the irregularity of teratomatous tissue (2,3). If no teratomatous or strumal elements are present, then a diagnosis of ovarian metastasis from a primary thyroid cancer should be considered. The two largest series of struma ovarii published to date have reported that papillary thyroid cancer (PTC) is more common than follicular thyroid cancer (3,11). One series found that four of six patients with PTC arising within struma ovarii tested positive for the BRAF V600E mutation (12). Thyroid cancer arising within struma ovarii is a subset within the wider category of “malignant struma,” which also includes cases of benign struma ovarii with evidence of local invasion or distant metastases.
Due to the rarity of thyroid cancer arising within struma ovarii, optimal management has not yet been defined. Surgical management of the primary tumor and the thyroid gland, as well as the potential indications for adjuvant treatment, have not been standardized. Pelvic management may include unilateral cystectomy, unilateral salpingo-oophorectomy (USO), or total abdominal hysterectomy with bilateral salpingo-oophorectomy (TAH/BSO). When extra-ovarian extension or distant metastases are present, total thyroidectomy may be performed to facilitate radioactive iodine (RAI) therapy. The role of thyroidectomy and RAI in localized, nonmetastatic struma ovarii thyroid cancer is not well-defined.
In this article, we present case histories of four patients with localized thyroid cancer arising within struma ovarii, and perform a comprehensive review of 53 reported cases in the English-language literature. This study included patients with struma ovarii confined to the ovary, and excluded patients with gross extra-ovarian disease or distant metastases. The extent of treatment and resultant outcomes were analyzed. We hypothesized that pelvic surgery alone is sufficient in patients without evidence of gross extra-ovarian extension or distant metastases.
Methods
After institutional review board approval, we performed a retrospective analysis of patients with thyroid cancer arising within struma ovarii. Cases were identified in a comprehensive pathology database maintained at a single academic institution between 1998 and 2010. Laboratory, imaging, inpatient, and clinic records were retrospectively analyzed for pertinent clinical and pathologic characteristics. A review of the English-language literature was then performed, thereby narrowing our search to identify cases of thyroid cancer arising within struma ovarii, without gross extra-ovarian extension or evidence of distant metastases. Queries within the National Library of Medicine PubMed resource were performed, using headings “struma ovarii” and “malignant struma ovarii.” Data were individually reviewed for appropriateness of inclusion. Patients with benign struma were excluded. Patients with <6 months of follow-up were excluded. To account for variable time-to-event and loss to follow-up, the cumulative rate of recurrence among cases was calculated by using the Kaplan-Meier method (SPSS version 14, SPSS, Chicago, IL).
Results
Demographic characteristics
Review of pathologic data identified 4 women with well-differentiated thyroid cancer arising within struma ovarii. Clinical details are outlined in Table 1. Median age was 44 (range, 43–57) years. Two women were nulliparous, and three were postmenopausal. Adnexal masses were palpable in all four women.
BSO, bilateral salpingo-oophorectomy; CT, computed tomography; FTC, follicular thyroid cancer; GXPX, gravida/para; HRT, hormone replacement therapy; NED, no evidence of disease; POM, postmenopausal; PTC, papillary thyroid cancer; U/S, ultrasound; RAI, radioactive iodine 131-I; Rx, adjuvant therapy (radioactive iodine or thyrotropin suppression with thyroxine); TAH, total abdominal hysterectomy; TT, total thyroidectomy; USO, unilateral salpingo-oophorectomy; y, year(s).
Pelvic imaging, surgery, and pathology
Ultrasound revealed ovarian cysts in all four women. Two patients underwent TAH/BSO, one patient had a previous history of TAH for endometrial sarcoma and underwent BSO alone, and one patient underwent left USO and right ovarian cystectomy. Final pathology revealed papillary (n=3) and follicular thyroid cancer (n=1) arising within struma ovarii, none of which demonstrated extra-ovarian extension (Figs. 1 –3). Testing for the BRAF V600E mutation was performed on the surgical specimens of two patients, and was found to be negative in all cases (patients 2 and 4, Table 1).
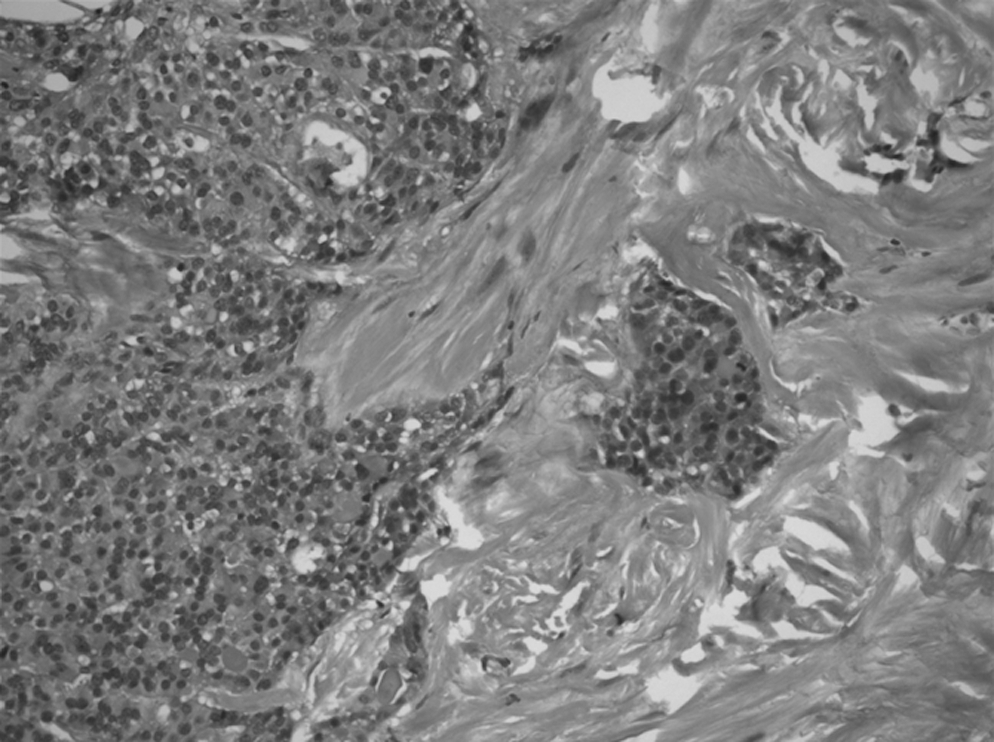
Follicular thyroid cancer arising within struma ovarii. Neoplastic cells arranged in irregularly shaped follicles and small cell clusters infiltrating through dense fibrous stroma (hematoxylin and eosin stain, original magnification 200×, patient 1).
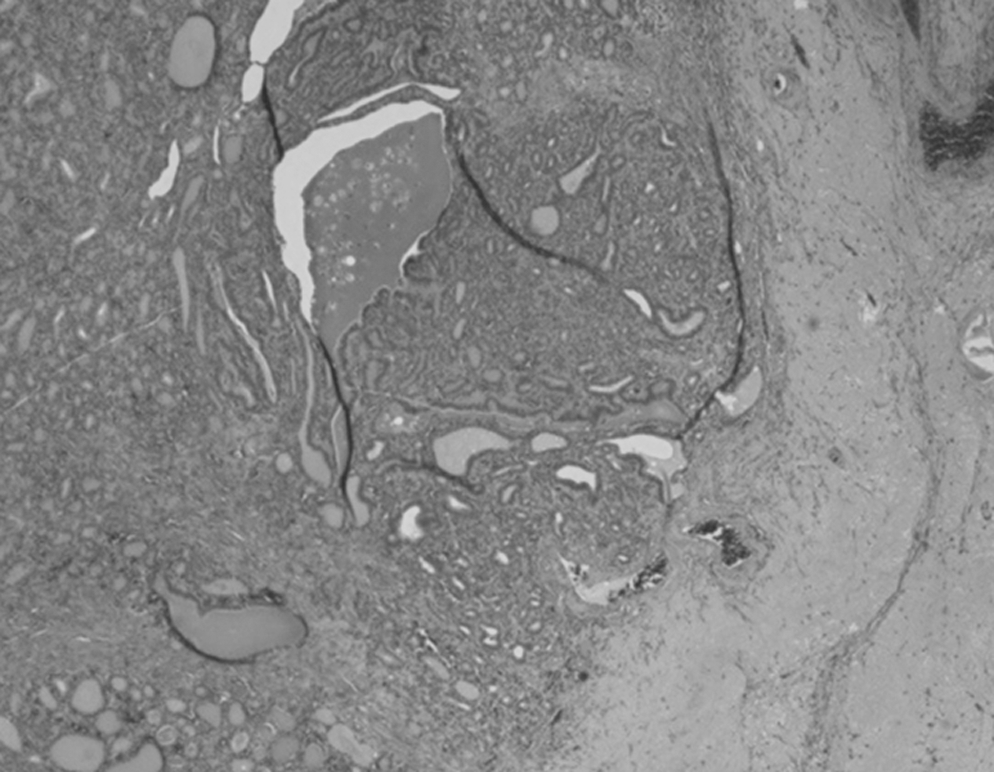
Papillary thyroid carcinoma arising within struma ovarii adjacent to corpus albicans (right, hematoxylin, and eosin stain, original magnification 40×, patient 2).
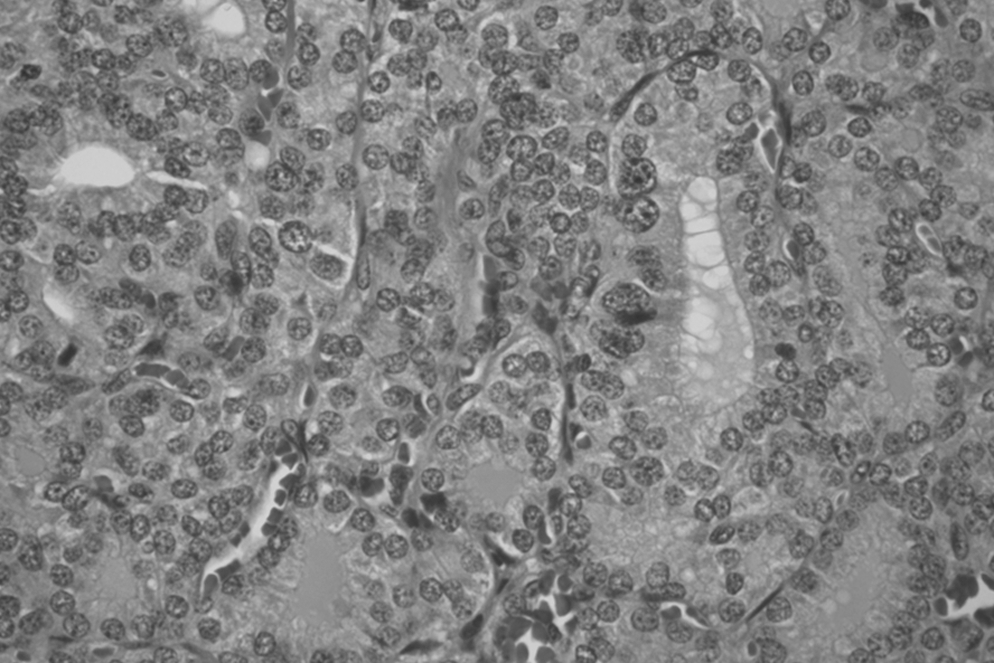
Papillary thyroid cancer arising within struma ovarii. Irregularly shaped follicles lined by cells with enlarged, crowded nuclei with powdery chromatin and grooves (hematoxylin and eosin stain, original magnification 400×, patient 2).
Thyroid imaging, surgery and pathology, and RAI
One patient had a previous history of left thyroid lobectomy for benign disease. Neck ultrasound revealed a stable 1.1 cm right thyroid nodule, and fine-needle aspiration cytology was benign, consistent with Hashimoto's thyroiditis. No further thyroid surgery was performed. One patient underwent total thyroidectomy and adjuvant RAI therapy. Final pathology revealed an incidental synchronous 5 mm PTC of the thyroid gland, with extrathyroidal extension and central lymph node metastasis (AJCC 7th edition stage pT3N1a, negative for the BRAF V600E mutation, Fig. 4). She received 29 and 150 milliCuries (mCi) of 131I, and was subsequently maintained on thyroid hormone suppression with levothyroxine. Two patients had a normal thyroid on physical examination, and further evaluation was either not recorded or not pursued.
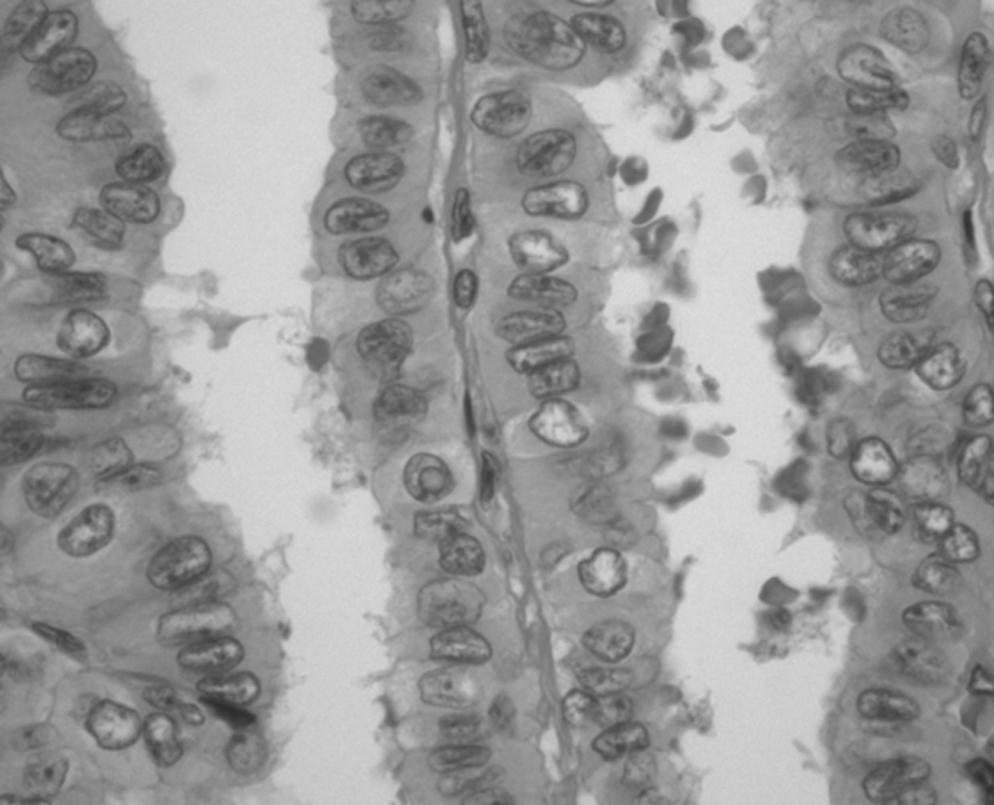
Synchronous papillary thyroid cancer of the thyroid gland. Neoplastic cells with enlarged nuclei lining papillae with fibrovascular cores. The nuclei are crowded and irregular with powdery chromatin, grooves, and pseudoinclusions (center of field, hematoxylin, and eosin stain; original magnification 600×, patient 4).
Clinical outcomes
No patients have been lost to follow-up. All four patients are currently free of disease, at a median follow-up of 9 years (range 0.8–13).
Literature review of 53 cases
We identified 53 reported cases of patients with well-differentiated thyroid cancer arising within struma ovarii, without distant metastases or gross extra-ovarian spread, in the literature. Details are provided in Table 2. Papillary thyroid cancer was the most common histology (74%), followed by follicular variant of papillary (21%), and follicular thyroid cancer (5%). All patients (n=53) underwent USO,±TAH/BSO. Specific details of pelvic surgery were available in 22 patients: 55% (n=12) underwent TAH/BSO, 9% underwent BSO (n=2), and 36% (n=8) underwent USO. Three patients (6%) underwent total thyroidectomy, and two of these patients also received RAI. The remaining 50 patients did not undergo thyroid surgery. Median follow-up was 7.0 years (range 0.5–25).
f/u, follow-up; FVPTC, follicular variant of papillary thyroid cancer; mo, month(s); mets, metastases; TSH, thyrotropin.
Three (6%) patients developed distant metastases at 1, 3, and 7 years, none of whom initially underwent total thyroidectomy with RAI (11,30). One patient developed liver metastases at 3 years (30). Thyroidectomy was subsequently performed, followed by three doses of 131I over 18 months (150, 30, and 150 mCi) (30). This patient had sustained stable disease since RAI for 4 years (30). Two other patients with PTC arising within struma ovarii recurred at 1 and 7 years, with reported recurrence in the abdomen in one patient and pulmonary metastasis in the other (11).
Including our four cases, recurrence data were available for a total of 57 patients. The extent of disease evaluation at last follow-up was variable among published reports, including computed tomography (CT), whole body scan, and/or clinical examination. The actuarial cumulative rate of recurrence at 25 years of follow-up was 7.5% (Fig. 5).
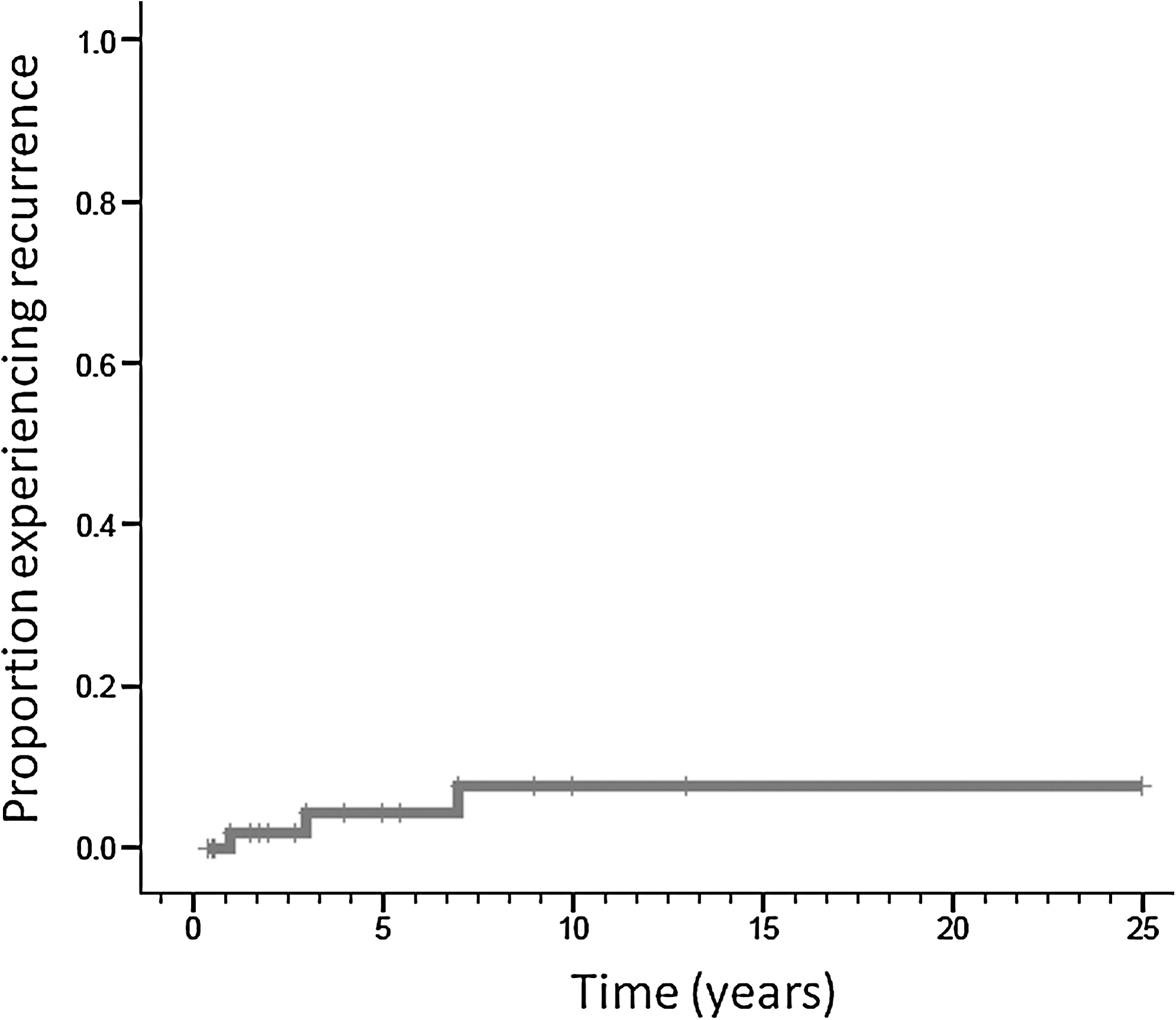
Cumulative 25-year recurrence rate of 7.5% as determined by the Kaplan-Meier method. n=57 patients, median follow-up 7 years (range 0.5–25).
Discussion
Malignant struma ovarii
In the literature, the term “malignant” has been inconsistently applied to struma ovarii, referring to cases demonstrating local invasion, distant metastases, or morphologic features of thyroid carcinoma on histologic analysis. Even “benign struma ovarii” has been reported to metastasize years after initial presentation (9,31,32). McGill et al. have reported intervals ranging from 5 months to 26 years from initial diagnosis to the development of metastases in patients with histologically benign or malignant struma ovarii (33).
The patients in this series and those identified in the literature demonstrated malignancy in the form of well-differentiated thyroid cancer arising within struma ovarii, without evidence of gross extra-ovarian extension or distant metastases at presentation. The choice of optimal treatment is challenging, because the natural history of this disease is not clear (34). The need for subsequent total thyroidectomy to facilitate adjuvant RAI therapy is controversial.
Presentation
Most patients with struma ovarii present with abdominal pain or a mass (3,11). Occasionally, patients may present with symptoms of hyperthyroidism. Uncommonly, struma ovarii has been diagnosed on RAI uptake scans after total thyroidectomy (7,35,36). Rarely, patients may present with ascites or an elevated ovarian cancer tumor marker, CA-125 (37). An ovarian adenocarcinoma is often initially suspected, prompting extensive primary surgery consisting of TAH/BSO, omentectomy, peritoneal washings, and lymph node sampling (8). Once the diagnosis of well-differentiated thyroid cancer arising within struma ovarii has been determined, then thyroid evaluation should be performed to exclude a synchronous thyroid malignancy.
Extent of surgery and therapy
In cases of malignant struma ovarii with distant metastases, aggressive treatment is warranted, including TAH/BSO and total thyroidectomy to facilitate adjuvant RAI therapy (8,9,33,38 –42). The goal of RAI treatment is to ablate metastatic thyroid cancer and to facilitate reliable surveillance for recurrence with whole body iodine scans and serum thyroglobulin levels.
However, in patients without metastases, the indications for thyroidectomy and RAI are unknown, as surgery of the primary tumor in the pelvis may be sufficient. In our series of four patients, all are currently without disease, and the majority (3 of 4) underwent pelvic surgery alone. Our review of 53 reported cases (Table 2) identified only 3 patients who developed recurrence. The cumulative rate of recurrence at 25 years among all 57 patients was only 7.5% (Fig. 5). However, as in patients with thyroid cancer, long-term follow-up (10–20 years) with a large patient cohort is required to definitively conclude that additional therapy is of no benefit. In premenopausal patients, the presumed benefits of RAI treatment in reducing the risk of recurrence should be weighed against the possible risk of temporary or permanent ovarian failure (8,33,43).
McGill et al. also have suggested that pelvic surgery alone may be sufficient for patients with well-differentiated thyroid cancer arising within struma ovarii, without metastases (16). They reserve total thyroidectomy and RAI for patients with metastases or recurrent disease.
Risk stratification
Yassa et al. support stratifying patients with well-differentiated thyroid cancer arising within struma ovarii into low- or high-risk groups to guide therapy (8). They suggest USO and thyroid stimulating hormone suppression with thyroxine for low-risk patients, defined as those with primary tumors <2 cm in size, confined to the ovary, and without aggressive histologic features (8). They reserve additional treatment (i.e., total thyroidectomy and RAI) for high-risk patients, those with cancers >2 cm, or with extra-ovarian extension (8).
Risk stratification has emerged as a critical component of thyroid cancer management. Tuttle et al. have reported that low-risk patients with thyroid cancer do not benefit from adjuvant RAI (27). Low-risk patients should have no local or distant metastases; have complete macroscopic tumor resection; no invasion of locoregional tissues; nonaggressive histology; no lymphovascular invasion; and no uptake outside the thyroid bed if an 131I uptake scan is performed (44). Janszen et al. support additional treatment with total thyroidectomy and RAI in patients with well-differentiated thyroid cancer arising within struma ovarii for tumors ≥1 cm; this recommendation uses extrapolated data from well-differentiated thyroid cancers arising in the thyroid gland, where RAI treatment provides minimal or no benefit in patients with subcentimeter cancers (30).
The present series and data from the literature, concerning patients with struma ovarii confined to the ovary at presentation, do not allow the determination of a tumor-size threshold for risk stratification. Assessing tumor size is particularly difficult, given that the cancer is often intermingled in teratomatous components. Thyroidectomy to facilitate RAI therapy is reasonable when extra-ovarian spread or metastases are present, or if synchronous primary thyroid gland cancer is diagnosed. In localized cases of struma ovarii, existing evidence drawn from reported cases in the literature reveals that the majority of patients will experience excellent disease control with surgery of the primary tumor in the pelvis alone, without adjunctive thyroidectomy and RAI treatment. Unlike cancer arising in the thyroid gland, where there is a risk of locoregional recurrence in the thyroid bed or lymph nodes, treatment failures in patients with thyroid cancer arising within struma ovarii appear to be limited to a low incidence of delayed distant metastases. These may impact patient survival differently than primary thyroid cancer neck recurrences.
A limitation of this study is the heterogeneity of reporting among case reports. Intraoperative findings and pathologic analyses were not always described in detail. Although we excluded cases with obvious extra-ovarian spread or distant metastases at the time of initial laparotomy, these findings may have been missed or under-reported, which would potentially lead to inclusion of patients at a higher risk and potential over-estimation of the rate of recurrence. Furthermore, the method of evaluating the extent of disease at the last follow-up varied among studies, some of which included surveillance CT, whole body radioiodine scan, or clinical examination. Heterogeneity in the level of scrutiny for recurrent disease could potentially lead to underestimation of the true recurrence rate.
In conclusion, based on this retrospective analysis, in patients with well-differentiated thyroid cancer confined to the ovary, pelvic surgery alone may be sufficient initial therapy. Prophylactic total thyroidectomy with RAI may be reserved for patients with gross extra-ovarian spread or distant metastases. However, our retrospective analysis has inherent limitations as just described, and definitive recommendations can only be made in the setting of a prospective trial. Unfortunately, a prospective trial is not likely feasible due to the rarity of the disease.
Footnotes
Acknowledgment
The authors would like to thank Ms. Monica Talmor, manager of the Molecular Diagnostics Lab of Yale University, for performing BRAF mutation testing on available specimens.
Author Disclosure Statement
The authors report no disclosures and have no competing financial interests.