
Abstract
Background:
Galectin-3 (G3) immunostaining of fine-needle aspiration (FNA) samples from thyroid nodules is very useful for the diagnosis of malignancy. The objective of the present study was to determine whether the absence of G3 immunostaining in preoperative FNA samples is associated with favorable clinicopathological parameters, including lymph node (LN) metastasis, in papillary thyroid carcinoma (PTC).
Methods:
The records of 868 patients with PTC who had prethyroidectomy ultrasonography-guided FNA with G3 immunostaining between January 2006 and December 2009 were retrospectively reviewed. G3 immunostaining was considered positive if the percentage of tumor cells showing definite cytoplasmic immunostaining exceeded 5%. Patients who had negative G3 immunostaining of FNA samples were assigned to the G3-negative (G3N) group; whereas those who had positive G3 immunostaining were assigned to the G3-positive (G3P) group.
Results:
There were 92 patients who were assigned to the G3N group (10.6%) because of the negative staining for G3 in the preoperative FNA samples from their thyroid nodules. The proportion of PTC subtypes in the G3N and G3P groups was similar (p=0.376). There was less frequent thyroid capsular invasion (46.7% vs. 66.5%, p<0.001), extrathyroidal extension (28.3% vs. 48.5%, p<0.001), and LN metastasis (22.2% vs. 48.7%, p<0.001) in the G3N group than the G3P group. In multivariate regression analysis, G3N expression predicted a lower risk of LN metastasis (odds ratio=0.37, 95% confidence interval 0.18–0.78) after adjustment for other clinicopathological parameters. Over a median follow-up of 33 months, no association was observed between G3N and disease-free survival.
Conclusion:
The absence of G3 expression in FNA samples from PTC is associated with pathological parameters considered less aggressive than is the case for PTCs with G3 expression, including being a negative predictor of negative LN involvement. Long-term follow-up studies, however, are needed to verify whether G3N patients have lower recurrence and mortality rates.
Introduction
Determining what thyroid surgery is optimum is difficult. Total thyroidectomy with wide lymph node (LN) resection can reduce the rate of recurrence, but may also cause permanent complications such as hypoparathyroidism and recurrent laryngeal nerve injury. Clinical parameters and ultrasonography findings provide an imprecise estimation of risk of tumor aggressiveness and metastases.
Galectin-3 (G3) belongs to a family of β-galactoside-binding lectins that can bind to the cell surface or matrix (8). G3 has attracted research interest, because G3-positive (G3P) immunostaining of fine-needle aspiration (FNA) samples reveals potent predictive value in the diagnosis of thyroid cancer, from 78% to 100% in sensitivity and from 81% to 94% in specificity (9 –11). Several studies suggested that increased G3 expression is associated with malignant transformation, tumor progression, and metastasis (12,13), and its expression in surgical specimens is significantly related to the aggressive characteristics of thyroid cancer (14 –16).
The present study was undertaken to evaluate whether preoperative evaluation of G3 expression in FNA cytology (FNAC) is associated with the invasiveness of thyroid cancer and LN involvement as noted by a histologic examination.
Methods
Subjects and study designs
A retrospective review was conducted on patients who received preoperative FNAC with G3 staining and who between January 2006 and December 2009 underwent thyroidectomy. FNAC was performed on the primary tumor in the outpatient clinic using a 23-G needle with ultrasound guidance. FNAC was categorized as inadequate, benign, indeterminate, and malignant.
After excluding 64 patients who had 46 inadequate cytologies and 18 G3-staining sections without available follicular cells, there were 1070 patients who were available for further analysis. After surgery, 141 patients were diagnosed as having benign lesions and 929 as having malignant tumors by histopathology. Of these patients, there were 917 with PTC who were eligible for further study. Three patients with follicular thyroid carcinoma, two patients with medullary thyroid carcinoma, and seven patients in whom there were discordant results in which there was a benign preoperative FNAC reading, but malignant histology, were not studied. Of the 917 patients, a total of 868 were included in the final analysis after further excluding those with aggressive subtypes (poorly differentiated carcinoma, PTC with squaumous cell carcinoma) and those who had limited surgery (subtotal thyroidectomy or lobectomy), reoperation, or loss to follow-up. Postoperative pathologic specimens were interpreted by two pathologists (K.L. and C.K.J.) according to the World Health Organization classification(17), independently of cytology and G3 immunostaining results.
Central lymph node dissection (CLND) was routinely performed in 625 patients regardless of clinical suspicion of metastatic LN. In addition, lateral LN biopsy or dissection was done in 117 patients if suspicious lesions were found in preoperative imaging or surgical field to assess LN involvement. The clinical and histopathologic data were retrospectively reviewed. The histopathologic parameters that were evaluated included primary tumor size, multifocality, tumor encapsulation, thyroid capsular invasion, extension, vascular invasion, and LN metastasis. TNM classification and staging were performed according to the criteria of the American Joint Committee on Cancer (AJCC) (18). The Institutional Review Board of the Clinical Research Coordinating Center in Seoul St. Mary's Hospital approved the study protocol.
G3 immunohistochemical staining
Material from FNAs was used to prepare slides for thyroid cytology from needle aspiration, and the remaining material was immediately fixed in 95% ethyl alcohol, and then processed to obtain paraffin-embedded cell blocks. Immunostaining was conducted on 4-μm-thick sections of cell blocks. Slides were deparaffinized in xylene and rehydrated with distilled water. Endogenous peroxidase activity was blocked by incubating the slides in 0.5% hydrogen peroxide in methanol for 10 minutes. After blockage of nonspecific binding sites with diluted normal serum for 10 minutes, the slides were incubated with 1:800 dilution of a specific monoclonal antibody against G3 (Novocastra Lab., Newcastle Upon Tyne, United Kingdom) for 30 minutes at room temperature. Then, specimens were detected using the EnVision Plus System (Dako, Carpinteria, CA) as recommended by the manufacturer, after which they were counterstained with hematoxylin. G3 immunostaining was considered positive if the percentage of tumor cells showing definite cytoplasmic immunostaining exceeded 5%. Otherwise, G3 was interpreted as being negative (10).
DNA isolation and detection of the BRAFV600E mutation from tumor tissue
Genomic DNA was extracted from two 10-mm-thick paraffin sections containing a representative portion of each tumor block using the QIAamp DNA Mini kit (Qiagen, Hilden, Germany). Neoplastic areas were manually microdissected from the tissue sections. A 224-bp fragment of exon 15 of the BRAF gene was amplified by polymerase chain reaction (PCR) using the forward primer (5′-TCATAATGCTTGCTCTGATAGG-3′) and reverse primer (5′-GGCCAAAAATTTAATCAGTGGA-3′). The PCR conditions were as follows: 35 cycles of 30 seconds at 94°C, 30 seconds at 55°C, and 30 seconds at 72°C. Water was used instead of template DNA for a negative control. The PCR products were then evaluated by 2% agarose gel electrophoresis, after which they were extracted from the gels and purified using a HiYieldTMGel/PCR DNA Extraction Kit (RBC Bioscience, Taipei, Taiwan). The purified PCR products were processed for the DNA sequencing reaction using the ABI-PRISM BigDye Terminator version 3.1 (Applied Biosystems, Foster, CA) according to the manufacturers' protocol. Sequencing was performed in both directions using the same primers used for PCR. Sequencing reactions were performed with 25 cycles for 10 seconds at 96°C, 5 seconds at 50°C, and 4 minutes at 60°C. Sequence data were generated using the ABI PRISM 3100 DNA Analyzer (Applied Biosystems), and the sequences were then analyzed and compared using the Sequencer 3.1.1. software (Applied Biosystems).
Postoperative management and follow-up
Subjects had a clinical examination every 3–6 months while taking doses of thyroxine (T4) designed to suppress serum thyrotropin (TSH), referred to here as T4 suppression therapy. At these visits, the patients had measurements of serum-free T4, TSH, and thyroglobulin (Tg) level. Serum Tg levels were measured using an immunoradiometric assay (IRMA) kit (CIS Bio International, Cedex, France) with a functional sensitivity of 0.7 ng/mL. Serum TSH levels were measured by IRMA (TSH IRMA kit; Beckman Coulter, Prague, Czech Republic), with a detection limit of 0.025 mIU/L. Among the 868 patients, 131I (30–250 mCi) was administered to 758, and whole-body scans (WBSs) were obtained after 5–7 days. Serum Tg levels were considered elevated when higher than 2.0 ng/mL on TSH stimulation (>30 mIU/L) or 1.0 ng/mL on TSH suppression. Recurrence of PTC was defined by cytological or pathological data or by elevated serum Tg levels with any evidence of radiological imaging, including 131I-WBS, chest computed tomography, or fluorodeoxyglucose (18F-FDG)-positron emission tomography studies were read as showing suspected recurrent disease.
Statistical analyses
Discrete data are summarized as numbers (percentages), and continuous data are expressed as means and standard deviations. The comparison of two continuous variables was done by Student's t-test and of categorized ones was done by χ2 test or Fisher's exact test. Univariate and multivariate logistic regression analysis were performed to estimate the odds ratio (OR) of LN metastasis for G3-negative (G3N) expression with adjustment for other clinicopathologic characteristics. Survival curves were generated with the Kaplan–Meier analysis, comparing survival with the log-rank test. Univariate and multivariate Cox proportional hazards analysis was used to assess the independent effects of G3N expression and other variables on recurrence and to adjust for confounders. A p-value<0.05 was considered statistically significant. All analyses were performed using SAS version 8.2 (SAS Institute, Cary, NC).
Results
Clinicopathologic characteristics of G3 expression in FNAC samples
Among the 868 patients with PTC, 776 patients (89.4%) had G3P cytology, and 92 patients (10.6%) did not express G3 (G3N). The G3N and G3P groups were similar in terms of age at diagnosis and sex distribution (Table 1). The G3N group had smaller-sized tumors (7.6±4.1 mm vs. 10.4±7.5 mm, p<0.001), less frequent capsular invasion (46.7% vs. 66.5%, p<0.001), and less extrathyroidal extension (28.3% vs. 48.5%, p<0.001) than the G3P group. In addition, the G3N group had less LN involvement than the G3P group (22.2% vs. 48.7%, p<0.001), both as far as the central compartment (23.1% vs. 48.5%, p<0.001) and the lateral compartment (14.3% vs. 69.1%, p=0.003) were concerned. The G3P group had more advanced clinical stages than the G3N group (AJCC stage III/IV; 35.6% vs. 21.7%, p=0.008).
One value is missing.
Assessment of central and lateral LN involvement only in patients who performed CLND with LND or biopsy.
Assessment of central LN only in patients who performed CLND.
Assessment of lateral LN only in patients who performed lateral neck evaluation.
G3, galectin-3; G3P, G3 positive; G3N, G3 negative; LN, lymph node; CLND, central lymph node dissection.
Among the 92 PTCs in the G3N group, 76 (82.6%) were of the classic variant. The percentage of classic variant PTC in the G3P group (86.7%) was not significantly different. Similarly, the frequency of follicular variant and other variants was similar in the G3N and G3P groups (Table 2).
One specimen (G3P) was not discriminated into the subtype.
Clinicopathologic characteristics according to the BRAF mutation status in 297 patients with PTC
Out of a total of 868 study subjects, 279 patients with PTC were tested for a 1799T>A (V600E) BRAF mutation using postoperative tumor tissue. Of these, 224 patients had PTCs that were positive for a BRAF mutation. The presence of a BRAF mutation was neither associated with G3 expression (p=0.366) nor associated with clinicopathologic features such as tumor size, capsular invasion, extrathyroidal extension, LN involvement, and tumor stages (Table 3).
Relationship between LN involvement with G3N and clinicopathologic parameters
In the 625 patients who had routine CLND, the frequency of LN metastasis was lower in the G3N group compared with the G3P group (OR=0.30 [95% confidence interval (CI) 0.16–0.58], p<0.001; Table 4). By univariate analysis, younger age, male sex, increased tumor size, multifocality, thyroid capsular invasion, vascular invasion, and extrathyroidal extension were also positively associated with LN metastasis. After adjustment of the clinicopathologic parameters just referred to, negative G3 immunostaining independently predicted a lower risk of LN metastasis in PTC (OR=0.37 [CI 0.18–0.78], p=0.009).
OR, odds ratio; CI, 95% confidence interval.
Predictive value of G3N for disease-free survival
To evaluate prognosis as it related to PTC recurrence, survival curves were generated using Kaplan–Meier analysis. These did not indicate an association between G3N immunostaining results and disease-free survival rate over a median follow-up of 33 months (p=0.245; Fig. 1). In Cox regression analysis, G3N immunostaining was not a significant predictor of disease recurrence or persistence by either a univariate or a multivariate model after adjusting for age, male sex, size, multifocality, extrathyroidal extension, LN metastasis, central neck dissection, and radioactive iodine treatment (p=0.735; Table 5).
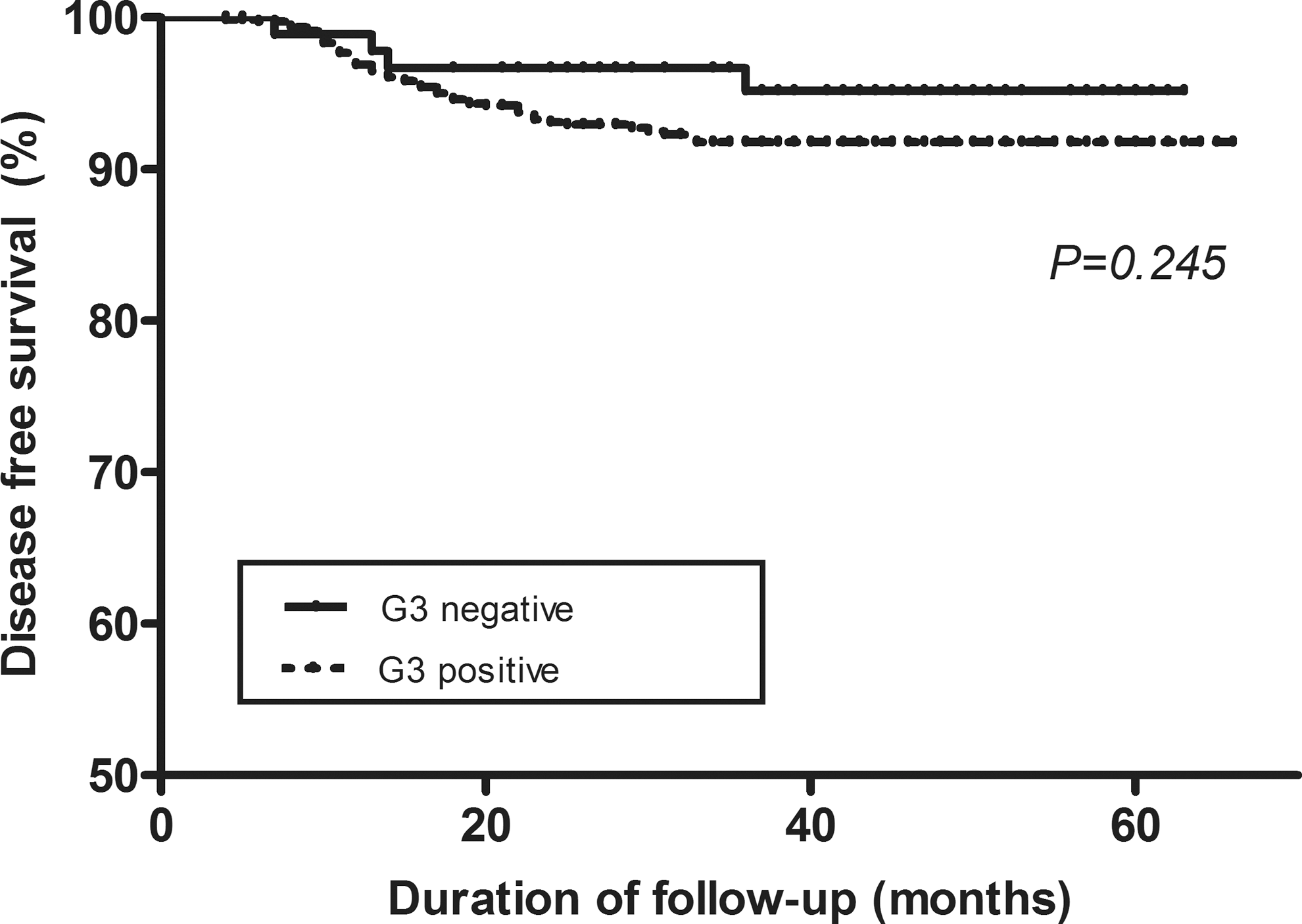
Kaplan–Meier survival curve according to galectin-3 staining.
Adjusted for age, male sex, size, multifocality, extrathyroidal extension, LN metastasis, central neck dissection, and radioactive iodine treatment.
HR, hazard ratio.
Discussion
With the progressive increase in the incidence of PTC, its proper treatment and management have become important issues. Current recommendations for management may lead to overtreatment in some patients whose PTC may be inherently indolent with a favorable outcome. Optimal preoperative risk assessment is crucial to stratify treatment. Among the recently recognized molecular markers of thyroid cancer, the T1799A BRAF mutation noted in patients with PTC is associated with higher tumor stages and its attendant earlier recurrence and greater mortality (19). It has been suggested that a BRAF mutation, when recognized in FNAC samples from PTC, is a useful presurgical indicator of less favorable tumor behavior. In our data, however, the presence of a BRAF mutation was not associated with unfavorable clinicopathologic features such as tumor size, capsular invasion, extrathyroidal extension, LN involvement, or tumor stage. In contrast, the absence of G3 expression in preoperative FNAC samples was indicative of more favorable clinicopathologic findings and the absence of LN involvement. Notably, we did not find an association between G3 expression and the BRAF mutation, as had been reported by Sapio et al. (20). In this study, due to differences in sample size, we could not compare the relative merits of G3 expression and a BRAF mutation in predicting the behavior of PTC. However, consistent with our data, several studies from Japan and Korea also did not find an association between the presence of a BRAF mutation and the aggressive characteristics of PTC (21,22). Therefore, at least for certain populations, the lack of G3 expression in preoperative FNAC samples may be better for the risk stratification of PTC than assessing whether a BRAF mutation is present.
G3 has been highlighted as a diagnostic tumor marker, because it is strongly expressed in some FNAC samples (10,23,24) or histology samples (23,25) from epithelial thyroid carcinomas but not normal thyroid tissues (25).
There are contradictory reports regarding the relationship between G3 expression and the invasive characteristics of PTC, some suggesting inverse relationship (26,27) and others reporting that G3 expression is associated with more tumor invasion and metastases (14 –16). In a study of 110 patients, Kawachi et al. (15) suggested that G3 expression in primary tumors was associated with LN metastases. Torregrossa et al. (16) reported that G3 was linked with the development of LN metastasis in the follicular variant of PTC, the proportion of G3P expression in tumors with metastasis being 96.1% as compared with 78.2% in tumors without this expression. In 147 patients with PTC, Savin et al. (14) also demonstrrated an association between strong G3 immunostaining and aggressive tumor characteristics, including LN metastases, size, extrathyroidal invasion, and a more advanced stage. Similar correlations have also been reported for medullary thyroid cancer (28,29).
The mechanism for the association between tumor G3 expression and a propensity to metastases is considered to be that G3 promotes the cellular interactions between tumors and adjacent tissue, formatting tumor emboli through cancer cell aggregation, extravasation, and implantation to other organs or tissues (13,30). G3 has roles in proliferation, antiapoptosis, and angiogenesis (31) that could foster tumor invasiveness. In an in vitro study, the overexpression of G3 increased cell motility and invasiveness (32) and promoted angiogenesis (31). In other studies, the suppression of G3 by RNA interference reduced the tumor metastases and tumor invasive properties (33) and had a pro-apoptotic effect (34). All of these data indicate that targeting G3 has potential for the therapy of PTC.
In the current study, the proportion of G3N expression was 10.6%. This is compatible to other studies in which negative expression of G3 was observed in 0%–25% of thyroid malignancies (10,23,24,35). Therefore, since G3 staining is not always found in malignancy, it is not always a reliable guide in the management of PTC. If CLND were performed only in the G3P group, 6.7% PTC (42/625) without central LN metastasis could escape unnecessary dissection compared with the routine performance of CLND. However, 1.9% PTC with LN metastasis (12/625) could be missed for evaluation (Table 1). Thus, other findings should be considered in planning management, and further research to identify prognostic markers is needed.
Perhaps unexpectedly, our data did not demonstrate that G3N expression was a prognostic marker of disease-free survival despite the fact that it was associated with favorable tumor characteristics. Such a relationship might exist but would not be evident considering the relatively short-term surveillance period of our study, which is one of its limitations. This study employed dichotomous categorization of G3 expression rather than a semiquantitative scoring method. The strength of our study was the relatively large number of patients and the fact that G3 expression was established before surgery rather than after the results of histopathology were available.
In conclusion, a negative expression of G3 in prethyroidectomy FNAC samples was associated with less aggressive and early stages of PTC and less LN involvement, independent of classic clinicopathologic parameters of tumor behavior. Long-term studies are needed to validate the prognostic significance of presurgical G3 immunocytostaining; these could help in determining the proper management of patients with PTC.
Footnotes
Acknowledgments
This research was supported by Seoul St. Mary's Clinical Medicine Research Program year of 2009 through the Catholic University of Korea. A part of these results was presented in abstract form at the 14th International Thyroid Congress, Paris, France, 2010.
Disclosure Statement
The authors have no conflicts of interest to declare.