
Abstract
Background:
French Polynesia has one of the world's highest thyroid cancer incidence rates. Iodine is suspected to play a role in this high incidence. The objective of this study was to assess whether low dietary iodine is related to a higher risk of thyroid cancer in the French Polynesian population.
Methods:
A case–control study was performed among native residents of French Polynesia. It included 229 cases of differentiated thyroid cancer diagnosed between 1979 and 2004 (203 women, 26 men) matched with 371 population controls (324 women, 47 men) on the date of birth. The current study is focused on dietary iodine intake and fish consumption (food rich in iodine) and analyzed by conditional logistic regression.
Results:
Daily dietary iodine intake was insufficient (<150 μg/day) in 60% of both cases and controls. A decreased risk of thyroid cancer was observed with a higher consumption of fish (p trend=0.008) and shellfish (p trend=0.002), and also with a higher dietary iodine intake (p trend=0.03). There was no significant interaction between the effects of the thyroid radiation dose and the dietary iodine intake (p=0.2).
Conclusion:
French Polynesia is a mild iodine deficiency area in which a higher consumption of food from the sea and a higher dietary iodine intake are significantly associated with a decreased risk of thyroid cancer. The quantification of this reduction requires specific investigation of iodine intake in traditional Polynesian food.
Introduction
The highest thyroid cancer incidence rates are observed among the populations of the Pacific, attaining 24.6/100,000 among French Polynesian women between 1985 and 1995, which is twice that observed among the Hawaiians of Hawaii and Maoris of New Zealand (4), and threefold higher than that observed among immigrants living in French Polynesia (5). French Polynesia comprises 118 main islands (76 inhabited) with a total area equivalent to that of Western Europe. It is composed of five archipelagos: the Windward Islands (Tahiti and Moorea) and the Leeward Islands (which make up the Society Islands), the Tuamotu-Gambier archipelago, the Austral Islands, and the Marquesas Islands. After the airport was built on Tahiti in 1961, changes in lifestyle led to a nutritional transition from the traditional diet of starchy roots, fish, and fruits to the addition of imported foods that are high in fat and low in fiber (6). We performed a case–control study to investigate the potential role of French atmospheric nuclear testing, which took place between 1966 and 1974 on Mururoa (7), on the high incidence of thyroid cancer in French Polynesia and to study other risk factors for differentiated thyroid cancer risk among the natives in this Pacific islander population.
A recent epidemiological review focused on nutritional factors (8) concluded that iodine intake might affect thyroid cancer risk and that fish consumption (a major source of iodine in food) was not consistently associated with this risk. In the current study, we focused on the role of iodine in French Polynesia in order to clarify the association with the risk of thyroid cancer.
Materials and Methods
The study population and methods have previously been reported (7,9 –12). The study was approved by the French Polynesian Ethics Committee. Written informed consent was obtained from all participants so that we could contact their physician.
Case selection
All patients diagnosed with a differentiated thyroid cancer before the age of 56, born and living in French Polynesia, were eligible for the study. This cutoff age was chosen in order to include mainly subjects who were younger than 15 at the time of the atmospheric nuclear tests (between 1966 and 1974). Four patients aged from 56 to 62 years at the time of the diagnosis, one case diagnosed in 1979, and two cases diagnosed in 2004 were included erroneously and were kept in the analysis because their characteristics were close to the inclusion criteria and results were unchanged when these cases and their controls were excluded. The cases were identified from the cancer registry of French Polynesia and medical insurance files and by the four endocrinologists in Tahiti. Histological information was obtained from the two histopathology laboratories (one public and one private) in Tahiti and from the medical files of endocrinologists. Follicular variants of papillary carcinomas were considered papillary lesions. The histological slides of 68 patients who had received 131I treatment at the Institute of Oncology Gustave Roussy were reviewed in the institute's pathology department, and the diagnoses were in agreement with those established in French Polynesia for 64 patients (94%). Of the 255 eligible differentiated thyroid cancer cases, 26 (10%) individuals were not interviewed because they had died (n=14), could not be located (n=6), or refused to participate (n=5), or the person was too ill to be interviewed (n=1). Finally, the study population consisted of 229 cases.
Matching process
For each eligible case, two potential controls closest in terms of the date of birth and matched on sex were randomly selected from the registry of births, which records all inhabitants born in French Polynesia. An SAS random number generator (SAS Institute, Inc., Cary, NC) was used for random selection. At the end of the interviews, a few cases had no interviewed controls. Each of those cases was matched with a control initially selected for another case of the same gender and with the same date of birth. Matching on the date of birth was then extended if necessary. Finally, of the 229 interviewed cases, 87 were matched with one control (38%) and 142 with two controls (62%).
Contacting controls and conducting interviews
Of the 458 randomly selected controls, 85 (19%) were not interviewed because the subjects had died (n=9), could not be located (n=29), refused to participate (n=29), were too ill to be interviewed (n=2), or had left French Polynesia (n=16). Among interviewed controls, we had no information on dietary consumption for two controls: overall, 371 controls were considered in the present analysis.
Data collection
The addresses of cases and controls were obtained from the territorial medical insurance plan, which covers all inhabitants, whatever their professional status. Interviews were conducted face-to-face by trained Polynesian interviewers and medical staff using a structured questionnaire. Cases diagnosed between 1979 and 2004 and matched controls answered the questionnaire between 2002 and 2004. Most interviews were conducted in French; very few were conducted in the Polynesian language and this mainly concerned the oldest participants. Some cases were interviewed at the hospital on the day of their usual follow-up consultation. Data collection included their ethnicity, education, smoking habits, lifetime weight changes, personal and family history of thyroid disease and cancer, places of residence, gynecologic and reproductive factors, medical X-ray exposure, and diet. For each subject, the total thyroid dose was calculated by summing the thyroid doses reconstructed for each nuclear test, taking into account age, source of drinking water, and data collected in the diet questionnaire (13).
Food frequency questionnaire
The dietary questionnaire was composed of two parts with a booklet of photographs to facilitate the estimation of portion sizes. The two parts included questions on the consumption (frequency and quantity) of seven food groups: the first part concerned consumption at the time of the interview and the second part concerned consumption during childhood. Overall, the questionnaire provided an estimate for daily consumption of 66 food items, 5 of which were food from the sea including pelagic fish, lagoon fish, fafaru, and shellfish (giant clams, other shellfish). Portion sizes were estimated with a photo booklet validated by the EPIC (European Prospective Investigation into Cancer) study (14).
We used the Pacific Islands food composition tables (15) to convert foods into nutrients. For each person, we calculated the average daily dietary energy intakes. We used the CIQUAL, a validated French food composition table (16) for the calculation of iodine intake because data were lacking in the Pacific Islands food composition tables. The food items that were richest in iodine were shellfish and fish (Fig. 1). The overall iodine intake took into account all the foods of the questionnaire, except iodized salt, because we had no precise information on the amount of iodized salt consumption.

Food richest in iodine (more than 7 μg per 100 g of food), based on the CIQUAL (Centre d'Information sur la Qualité des Aliments) food composition table.
Statistical analysis
Data were analyzed using conditional logistic regression (17) with the SAS software, version 9.1 (SAS Institute). Food item consumption and dietary iodine intake were categorized into tertiles based on the distribution among controls. If more than 33% of the controls declared that they never consumed a given food item, we used nonconsumers as the reference category, and we divided consumers into two categories using the median of the distribution among controls. We also used the WHO/ICCIDD/UNICEF classification of iodine nutrition status (1): <30 μg/day (severe deficiency), 30–74 μg/day (moderate deficiency), 75–149 μg/day (mild deficiency), 150–299 μg/day (optimal—reference), 300–449 μg/day (more than adequate), and ≥450 μg/day (possible excess). Another variable related to iodine was also analyzed: the use of iodized salt (never, occasionally, always). Analyses were stratified by age and sex. All odds ratios (ORs) were adjusted for smoking status (ever, never), family history of thyroid cancer (yes, no), head or neck exposure to medical X-ray irradiation before the age of 15 (yes, no), body surface area (tertiles), and the number of births following full-term pregnancies (continuous) for women, which were identified as risk factors in previous analyses (9,11,12). ORs were also adjusted for ethnicity (Polynesian, Poly-European or Poly-Asian, other), education level (no diploma, middle school, high school, or university), dietary energy intake (tertiles), and interviewers. Because each interviewer did not always interview cases and controls belonging to the same strata, we adjusted on “interviewer” because some answers may have been influenced by differences in the interviewee's confidence in female and male interviewers when intimate questions were asked. All p values presented are two-sided and a p value of <0.05 was considered statistically significant. Tests for trend were performed by assigning the median value to each quartile and then, modeling this as a continuous variable using the Wald chi-square statistic.
Analyses were conducted for the consumption of food from the sea and dietary iodine intake during childhood and at the time of the interview. Separate analyses were performed according to ethnicity, smoking status, the archipelago of birth and of residence, the histology of differentiated thyroid cancer, the thyroid radiation dose, and in subjects who did not consume iodized salt.
Results
Characteristics of participants
Papillary carcinoma was the histological type in 77% of cases (Table 1). Half of the cases and controls had parents who were both Polynesian and just over 30% had one Polynesian parent while the other parent was either European or Asian (Table 2). About 90% of cases and controls born in the Windward Islands (Tahiti and Moorea) were living in the Windward Islands at the time of the interview, while only 35% of cases and controls born in another archipelago were living there at the time of the interview (i.e., 65% of subjects had gone to live in Windward Islands).
For two cases and two controls, we had no information about the archipelago of birth.
ICCIDD, International Council for the Control of Iodine Deficiency Disorders.
Nutritional characteristics at the time of the interview
In our French Polynesian study, the mean daily energy intake among controls was 2800 kcal in women and 3600 kcal in men, while in the French population with intense physical activity, the recommended daily energy intake is 2600 kcal for women and 3400 kcal for men (18). We observed that 41% of the male and female controls consumed more than the recommended daily energy intake and 20% consumed more than 4000 kcal per day whatever the gender.
Among controls, food from the sea was consumed more frequently in the Tuamotu-Gambier archipelago (Fig. 2): 70% of controls living in the Tuamotu-Gambier archipelago ate more than 90 g of fish and shellfish per day, versus only 30% of controls living in other archipelagos. The inhabitants of the Tuamotu-Gambier archipelago ate chiefly local food, while those of the Windward Islands ate rather processed foods. On average, cases of thyroid cancer consumed 71 g of fish and shellfish per day, while controls consumed 83 g/day.
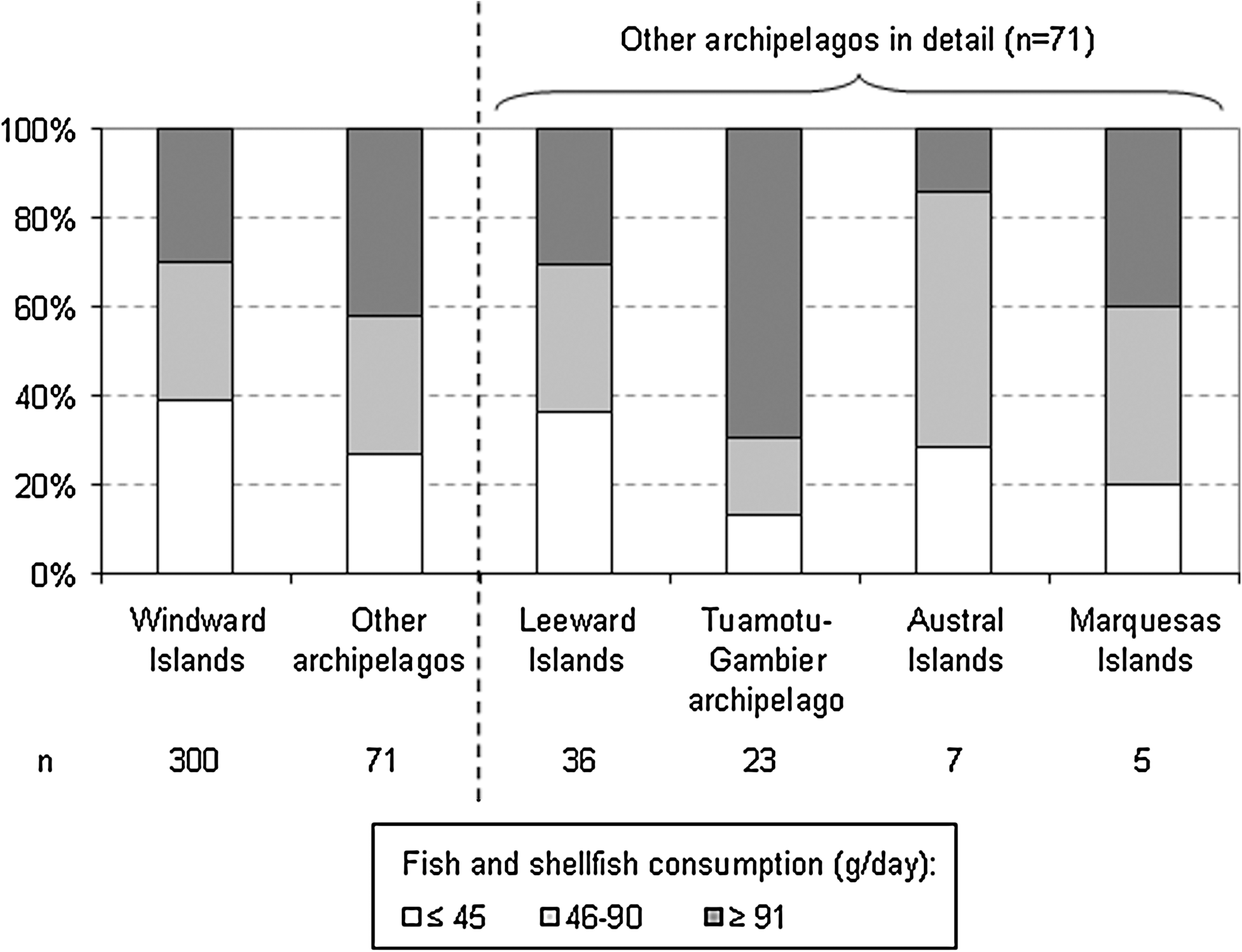
Consumption of food from the sea according to archipelagos of residence, among controls, French Polynesia, 1979–2004.
Iodine nutrition deficiency (<150 μg/day) was observed in 60% of cases and controls and only 30% had optimal iodine nutrition (150–299 μg/day). Among subjects with iodine nutrition deficiency, two-thirds had mild deficiency (75–149 μg/day) (Table 2).
Association between dietary iodine and risk of thyroid cancer
The risk of thyroid cancer decreased significantly with the increasing consumption of fish and shellfish at the time of the interview (Table 3). Among shellfish, increased giant clam consumption was particularly associated with a decreased risk of thyroid cancer: the risk for consumers compared with nonconsumers was 0.42 (95% confidence interval [CI]: 0.25, 0.69).
ORs were adjusted for smoking, family history of thyroid cancer, radiation to the head or neck for the diagnosis before 15 years old, body surface area, number of full-term pregnancies among women, ethnicity, education level, dietary energy intake, and interviewers.
Includes foods, except iodized salt.
For eight cases and three controls, we had no information about the consumption of iodized salt.
OR, odds ratio; CI, confidence interval.
At the time of the interview, a high dietary iodine intake was significantly associated with a decreased risk of thyroid cancer (p trend=0.03). Subjects with severe or moderate iodine nutrition deficiency (<75 μg/day) had a 2.6-fold increased risk of thyroid cancer (95% CI: 1.12, 5.93) compared with subjects with optimal iodine nutrition (150–299 μg/day).
Overall, daily iodized salt consumption at the time of the interview was associated with a 5.8-fold increased risk of thyroid cancer (Table 3).
The results on fish and shellfish, dietary iodine intake, and iodized salt consumption remained unchanged after additional adjustment with thyroid dose from exposure to radioactive fallout before 15 years of age. A sensitivity analysis in subjects who never consumed iodized salt (120 cases and 260 controls) showed that results were quite similar, but they were not significant, probably due to lack of power (results not shown).
The association between the risk of thyroid cancer and both dietary iodine intake and iodized salt consumption was not significantly different according to the histology of cancer (Table 4), smoking status (Table 5), ethnicity, and the archipelago of birth, and of residence (results not shown). It would seem that the increased risk of thyroid cancer associated with low dietary iodine is higher in follicular type than in papillary type (Table 4) and also higher in smokers than nonsmokers (Table 5), but the interactions were not significant.
ORs were adjusted for smoking, family history of thyroid cancer, radiation to the head or neck for the diagnosis before 15 years old, body surface area, number of full-term pregnancies among women, ethnicity, education level, dietary energy intake, and interviewers.
Includes foods, except iodized salt.
For eight cases and three controls, we had no information about the consumption of iodized salt.
Ca, number of cases; Co, number of controls.
ORs were adjusted for family history of thyroid cancer, radiation to the head or neck for the diagnosis before 15 years old, body surface area, number of full-term pregnancies among women, ethnicity, education level, dietary energy intake, and interviewers.
Includes foods, except iodized salt.
For eight cases and three controls, we had no information about the consumption of iodized salt.
The thyroid radiation dose received before the age of 15 years was not correlated with dietary iodine intake (r=0.1, p=0.06) and we did not find any significant interaction (p=0.2) between the effects of the thyroid radiation dose and the ones of dietary iodine intake.
Neither the reported fish and shellfish consumption, nor the iodized salt use during childhood was significantly linked to the risk of thyroid cancer. A high dietary iodine intake in childhood was significantly associated with a decreased risk of thyroid cancer (p trend=0.03) (results not shown).
Discussion
In this case–control study conducted in French Polynesia, which included 229 cases of thyroid cancer and 371 controls, we observed that cases reported a lower consumption of food from the sea, in particular shellfish consumption, than controls. As a consequence, we estimated a lower dietary iodine intake for cases than for controls because fish and shellfish are the richest food sources of iodine. In contrast, a greater percentage of heavier consumers of iodized salt was observed among cases than among controls.
This study aimed to include almost all the cases of thyroid cancer diagnosed from 1981 to 2003 in French Polynesia and among natives from this territory. Given the geographic isolation of French Polynesia and the high standard of the local public health system, only a few recent cases may have been missed by the cancer registry, the medical insurance system, and the endocrinologists in Tahiti. As thyroid cancer is rarely lethal, the restriction of the study to individuals alive at the time of the interview is not likely to have been a major source of bias.
Controls were selected randomly from the Polynesian registry of birth, which includes all persons born in French Polynesia. Among the 458 potential controls, 85 did not qualify for interviewing. These noninterviewed potential controls were born earlier than the interviewed controls (1955 in average, vs. 1957, p=0.09), but were of similar gender and place of birth distribution. An analysis was performed using conditional logistic regression matched on the date of birth; therefore, this potential source of bias was controlled.
For a number of reasons, including fewer uncertainties and fewer possible biases when reporting, cohort studies are far more appropriate for the investigation of dietary habits than case–control studies. Our study results are nevertheless interesting because no cohort study exists in French Polynesia. Furthermore, despite Westernization, food is less varied and some dietary habits continue to persist, especially on islands other than Tahiti, and the reporting is easier. In our opinion, at the time of the interview, Polynesians were unaware of the hypothesis linking cancer to higher overall or specific food consumption, but they had a priori knowledge of the role attributed to the nuclear tests performed by France in Mururoa and Fangataufa. In 1995, a study was conducted on food consumption in French Polynesia (19): the mean daily consumption of food from the sea was similar to that of controls in our study.
A limitation of our study is that the dietary iodine intake, which was estimated by the amount and composition of the food intake of the participants, employed a composition table established in metropolitan France (16). This table is probably not well adapted to French Polynesia: for example, fish (from the lagoon and the Pacific Ocean) consumed in French Polynesia is different from fish consumed in metropolitan France. But data on iodine intake were lacking in the Pacific Islands food composition tables. Moreover, both food composition tables did not give iodine intake according to cooking methods that may affect iodine content of the final product. A 24-hour measurement of urinary iodine in addition to the food questionnaire would have been more appropriate, unfortunately it would have been very difficult to apply this method during our epidemiological study.
We cannot evaluate the amount of iodized salt consumed in our study, because we only knew whether subjects “never, occasionally, or always” used iodized salt. Moreover, iodine concentration in iodized salt decreases over time and depends on the level of humidity (20,21). According to the literature, iodine content in iodized salt varies from 5 to 205 ppm (21 –23).
To date no study has established the iodine status in this French overseas territory. Based on the controls in our study, who are supposed to be representative of French Polynesian natives of the same age, our study shows that French Polynesia may be considered as an area of low iodine deficiency (Table 2): 60% of controls have iodine nutrition deficiency according to the International Council for the Control of Iodine Deficiency Disorders (ICCIDD) classification (1).
In our case–control study, we observed that high fish consumption decreased the risk of differentiated thyroid cancer, in particular shellfish consumption. These findings are in agreement with most of the other studies. In the pooled analysis of 13 case–control studies (24) conducted in the United States, Japan, China, and Europe, fish consumption was not significantly associated with thyroid cancer risk, but a protective effect was suggested in the six studies conducted in endemic goiter areas and a decreased risk was found in Los Angeles (24,25), which is an iodine-rich area. In three more recent studies, a protective effect was found with high fish and shellfish consumption in California (26) and Kuwait (27), and a study in New Caledonia (28) evidenced that a high consumption of brackish water fish decreased the risk of thyroid cancer.
In this French Polynesian study, we found that a high dietary iodine intake decreased the risk of thyroid cancer. This result is consistent with both the high incidence of thyroid cancer and the mild iodine deficiency in French Polynesia. An estimation of dietary iodine intake was performed only in three studies. In the multiethnic case–control study in California (26), a high dietary iodine intake also lowered the risk of thyroid cancer. In contrast, a study conducted in Hawaii (29) found a nonsignificantly increased risk of thyroid cancer with a high dietary iodine intake. It is difficult to compare our results with those results because Westernization of the way of life in this U.S. overseas state occurred earlier and to a greater extent than in French Polynesia, and therefore it is difficult to compare our results. In the recent study in New Caledonia (28), no association was found between dietary iodine intake and the risk of thyroid cancer.
We found that individuals who had developed thyroid cancer consumed iodized salt more frequently than healthy controls, which is not in agreement with previous findings: no association was found in the Swedish study (30) and a decreased risk was found in Norway (30) with iodized salt (yes, no). We also found that iodized salt use increased the risk of thyroid cancer in both papillary and follicular histology, with a higher risk in follicular than in papillary thyroid cancer, but the latter interaction was not significant. However, we must be cautious with our results on iodized salt use because endocrinologists in Tahiti had advised patients who had a goiter or thyroid cancer to consume iodized salt.
We did not find significant interaction between iodine nutrition status and the radiation exposure in childhood on thyroid cancer risk, but this could be explained by a lack of power. Two studies on thyroid cancer following the Chernobyl accident (31,32) found that the risk of radiation-related thyroid cancer was higher in iodine deficiency areas. Nevertheless, the radiation doses were about 100 times higher in these two studies than in ours (7) (mean dose: 2 mGy in French Polynesia, more than 200 mGy in Chernobyl areas). Another difference between Chernobyl areas and French Polynesia was the dietary habits. Indeed, the main source of contamination by radioiodine in Chernobyl areas was the milk (33), which was consumed very little in French Polynesia. Whereas, the thyroid radiation dose during the nuclear tests in French Polynesia was almost exclusively due to the contamination of leafy vegetables (7), which counts for very little in the dietary intake of stable iodine, contrary to fish and shellfish, not significantly contaminated.
We did not obtain evidence for a relationship between reported fish or shellfish consumption during childhood and the risk of thyroid cancer. We do not think that this is due to a greater recall bias or uncertainties in the reporting of dietary behavior during childhood rather than the reporting of recent dietary behavior. Indeed, during childhood, the dietary behavior of cases and controls in our study was much simpler than their current dietary behavior: there were very few imported foods in French Polynesia during the sixties and seventies and half of the Polynesians lived on islands or atolls without an airport where their diet was almost exclusively limited to local products. We rather believe that if low dietary iodine intake plays a role in the risk of thyroid cancer, it is mainly by promoting precancerous lesions, rather than by inducing new ones and this is therefore a short-term effect.
In conclusion, French Polynesia is a mild iodine deficiency area in which a higher consumption of food from the sea and a higher dietary iodine intake are significantly associated with a lower risk of thyroid cancer. The quantification of this reduction requires a specific investigation on iodine intake in traditional Polynesian food.
Footnotes
Acknowledgments
This study was supported by the Association pour la Recherche Contre le Cancer, the Ligue Nationale Contre le Cancer, the Direction Générale de la Santé, the Comité de Radioprotection de Electricité de France, Agence Française de Sécurité Sanitaire et Environnementale et du Travail, CHILD-THYR EEC programme, and the Fondation de France.
The authors thank Lorna Saint Ange for editing. They wish to thank John Paoaafaite and Joseph Teuri who contacted and interviewed cases and controls in the study. They are also grateful to Barbara Burlingame, leader of group “Nutrient requirements and assessment” of the Food and Agriculture Organization, for the validation of the estimates of French Polynesian nutrients (in particular, energy) from the Pacific Islands food composition tables.
Disclosure Statement
The authors declare that no competing financial interests exist.