
Abstract
Background:
Fine-needle aspiration biopsy (FNAB) is a simple technique for the investigation of suspicious thyroid nodules. However, low success rates are reported in the literature. The aim of this prospective study was to compare the clinical performance and impact of an automatic aspirator, referred to here as Aspirator 3, to those of the manual technique for the FNAB of clinically suspicious thyroid nodules.
Methods:
One hundred nine consecutive patients with 121 clinically suspicious thyroid nodules underwent a biopsy twice of the same site with the clinically approved Aspirator 3 and with the manual technique. The number of follicular cell formations and the total number of follicular cells in the aspirate were counted using the ThinPrep® method.
Results:
With the Aspirator 3, the total number and the mean number of extracted cell formations were significantly higher than the values achieved with the manual technique (total: 3222 vs. 1951, p=0.02; mean: 27 vs. 16). The total number of cells that were biopsied was also higher when the Aspirator 3 was utilized (47,480 vs. 23,080, p=0.005). Overall, the Aspirator 3 was superior in 65 biopsies, and the manual technique was superior in 39 biopsies.
Conclusions:
In terms of cell formations and the total number of cells aspirated, the Aspirator 3 was superior to the manual technique. Further, the Aspirator 3 was more convenient to use and had a greater precision in needle guidance.
Introduction
In a pilot study using a prototype of an automatic aspirator, we evaluated a novel aspiration technique in vitro and reported the first clinical results obtained with this new tool (12,13). These results demonstrated that an automatic aspirator was more effective than the manual technique for the aspiration of cells from thyroid nodules. Moreover, compared with aspirating the nodules manually with Cameco-syringe pistol (Precision Dynamics Corporation, Burbank, CA) the new device was significantly more convenient to handle. In the present study, we evaluated an improved automatic aspirator that is approved for the biopsy of follicles, the Aspirator 3.
Methods
Study design
One hundred nine consecutive patients with one or more nonautonomous nodules were included. Each nodule was biopsied twice, once with the Aspirator 3 and once with the manual technique. The total cytologic material from both biopsies was stored in polypropylene tubes and sent to the Institute of Pathology and Neuropathology, University Hospital of Essen, Germany, to assess the number of thyrocytes and thyrocyte clusters as well as for routine cytological evaluation using the ThinPrep® (Hologic Deutschland GmbH, Frankfurt am Main, Germany) method.
Aspirator 3
The standard configuration of the Aspirator 3 (Labotect Labor-Technik-Göttingen GmbH, Göttingen, Germany, approved according to Council Directive 93/42EEC [European Economic Community] concerning medical devices as Class IIa medical devices for the biopsy of ovarian follicle) includes a foot pedal to create a customized vacuum (Fig. 1). The needle was connected to this system via plastic tubing. A microfilter was fitted between the device and the syringe to avoid fluid aspiration into the instrument. After the tip of the needle is sonographically located in a node, the operation of the foot pedal generates a vacuum to aspirate thyrocytes. Because the needle-guiding hand has not build the vacuum simultaneously, the aspiration can be performed with greater accuracy (Fig. 2).
Original photo of the Aspirator 3 used in this study.
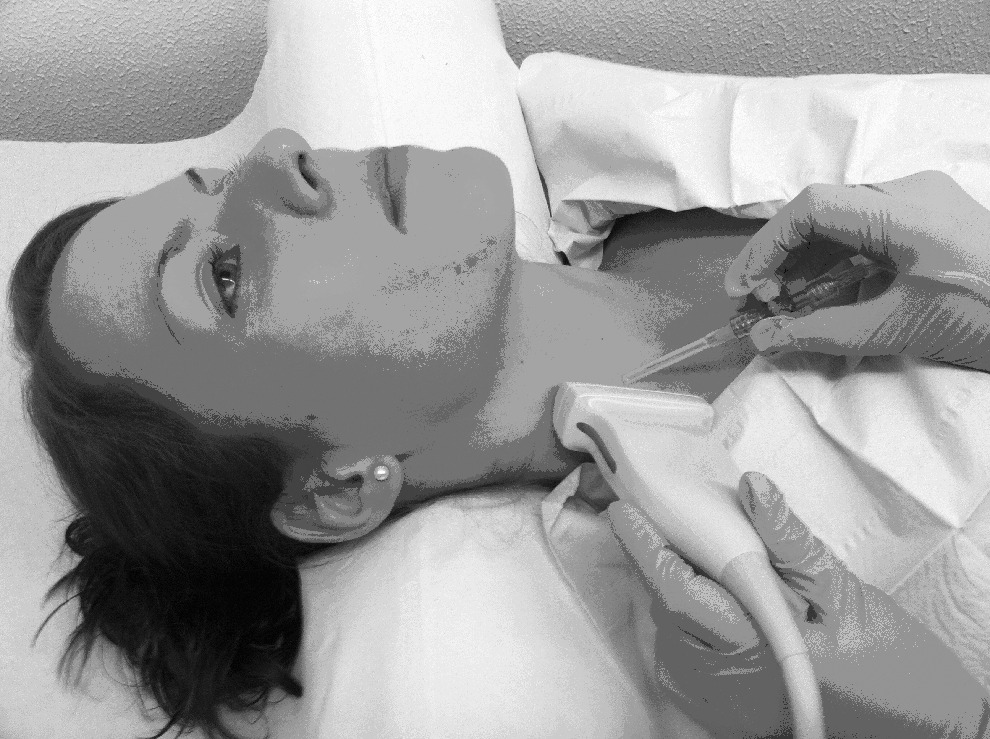
Handling of the sonographic device and the biopsy needle using the Aspirator 3.
Patients
One hundred nine consecutive patients at the Thyroid Center of Bottrop and Dorsten, Germany (F: 72, M: 37; mean age 56.2±13.7), with at least one nonautonomous nodule were included in this study. Each individual nodule was biopsied twice applying the Aspirator 3 and subsequently the manual technique. In 12 patients, two clinically suspicious nodules were biopsied, accounting for a total of 121 biopsied thyroid nodules.
Fine-needle aspiration biopsy
The FNAB was performed by only one experienced physician (J.F.) conducting annually several hundred FNABs. The aspiration biopsy was performed first by the Aspirator 3 followed by the manual technique. Similar to the manual technique, the evacuation process through the Aspirator 3 for the same site was started after the tip of the needle was sonographically visualized in the nodule, followed by 5–10 fan-shaped oscillations of the needle in the nodule for ∼10 seconds. Before removing the needle, the negative pressure was relieved. The needle was then disconnected from the syringe, and the aspirate was washed out with 1 mL 0.9% NaCl solution in a polypropylene tube (containing 30 mL of Cytolyt® fluid). The conserved aspirate was sent to the Institute of Pathology and Neuropathology, University Hospital of Essen, within 24 hours to analyze the sample using the ThinPrep (Hologic Deutschland GmbH) method. Because of the significantly better results achieved with a 21-gauge needle, compared with those achieved with the 27-gauge needles used in our pilot study (12,13), the FNABs were performed with 21-gauge needles in the present study. To evaluate the aspiration powers of the two techniques, the number of cell formations and the total number of cells (only one ThinPrep slide per aspiration was used) in each cell formation were counted by a pathologist (S.Y.S.) experienced in the cytologic diagnosis of thyroid cells. If the number of cell clusters was lower than 5 and there were fewer than 10 cells, then the aspirate was classified as nondiagnostic. To compare the two aspiration techniques, the total number of cells and cell clusters, as well as the number of FNABs without any results, were counted (16).
Results
The Aspirator 3 aspirated a total of 47,480 cells and 3222 cell clusters for the entire cohort, with an average of 27 (mean 10, range 0–142) cell formations per case (Table 1). In 23 cases no thyrocytes could be identified in the aspirate, and in 2 cases, the results from the manual technique were identical to the results from the Aspirator 3. Overall the Aspirator 3 provided 81% diagnostically evaluable biopsies, whereas the manual technique provided 76% (p=0.06; McNemar test).
p=0.02; b p=0.005: Wilcoxon rank sum test; c p=0.06: McNemar test.
The manual technique aspirated a total of 1951 cell formations and an average of 16 cell formations per biopsy (median: 6, range 0–132), with a total of 23,080 cells (Table 1). Twenty-nine cases had no thyrocytes in the aspirate.
Based on the number of cell formations and the total number of cells, the difference between the two techniques was significant (p=0.02 for cell formations and p=0.005 for the total number of cells, respectively; Wilcoxon rank sum test) (Figs. 3 and 4).
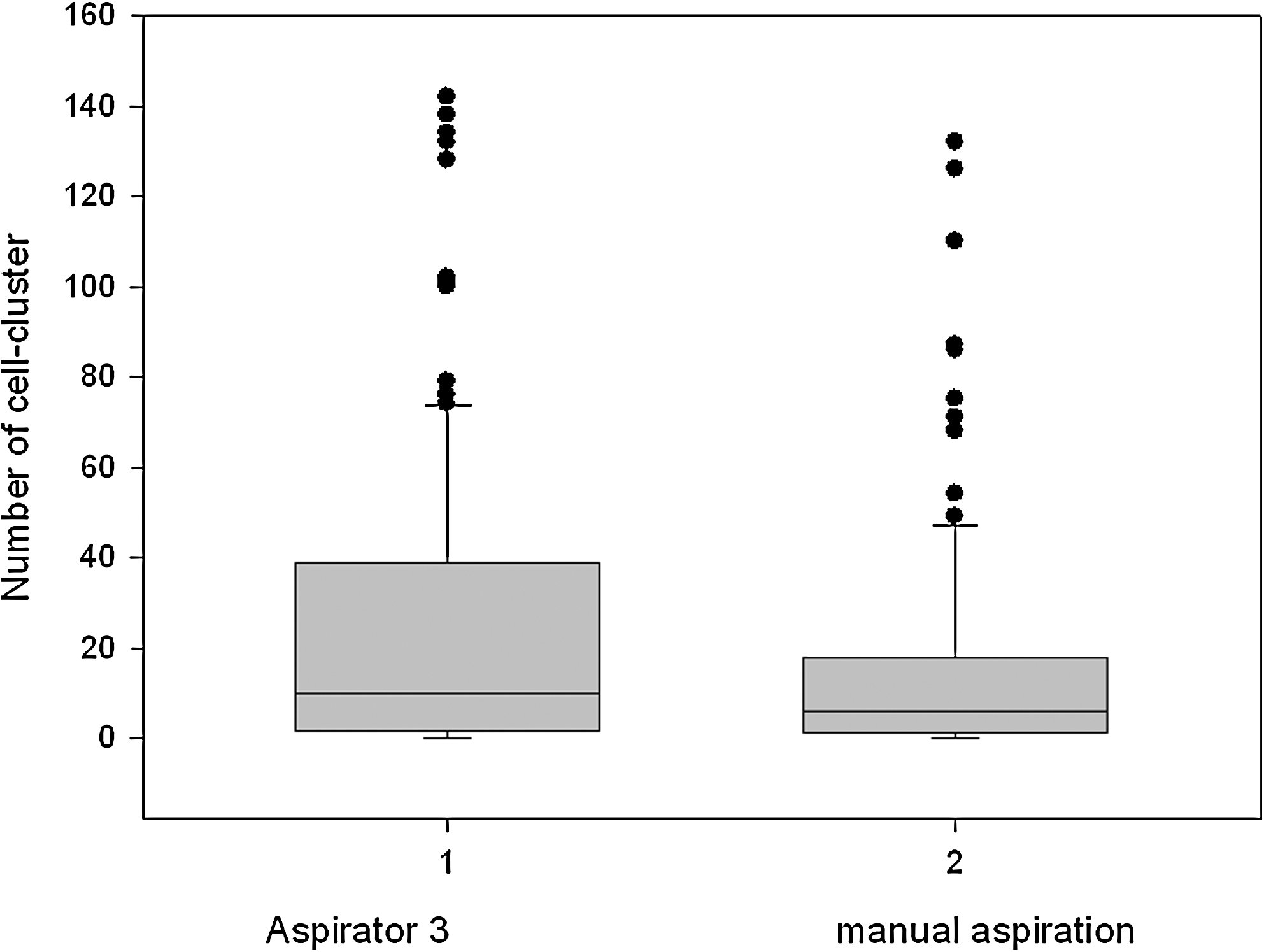
Comparison of aspiration power of the Aspirator 3 versus manual technique (Cameco® gun) in case of the number of cell cluster per patient. The median difference was statistically significant (p=0.02; Wilcoxon rank sum test).
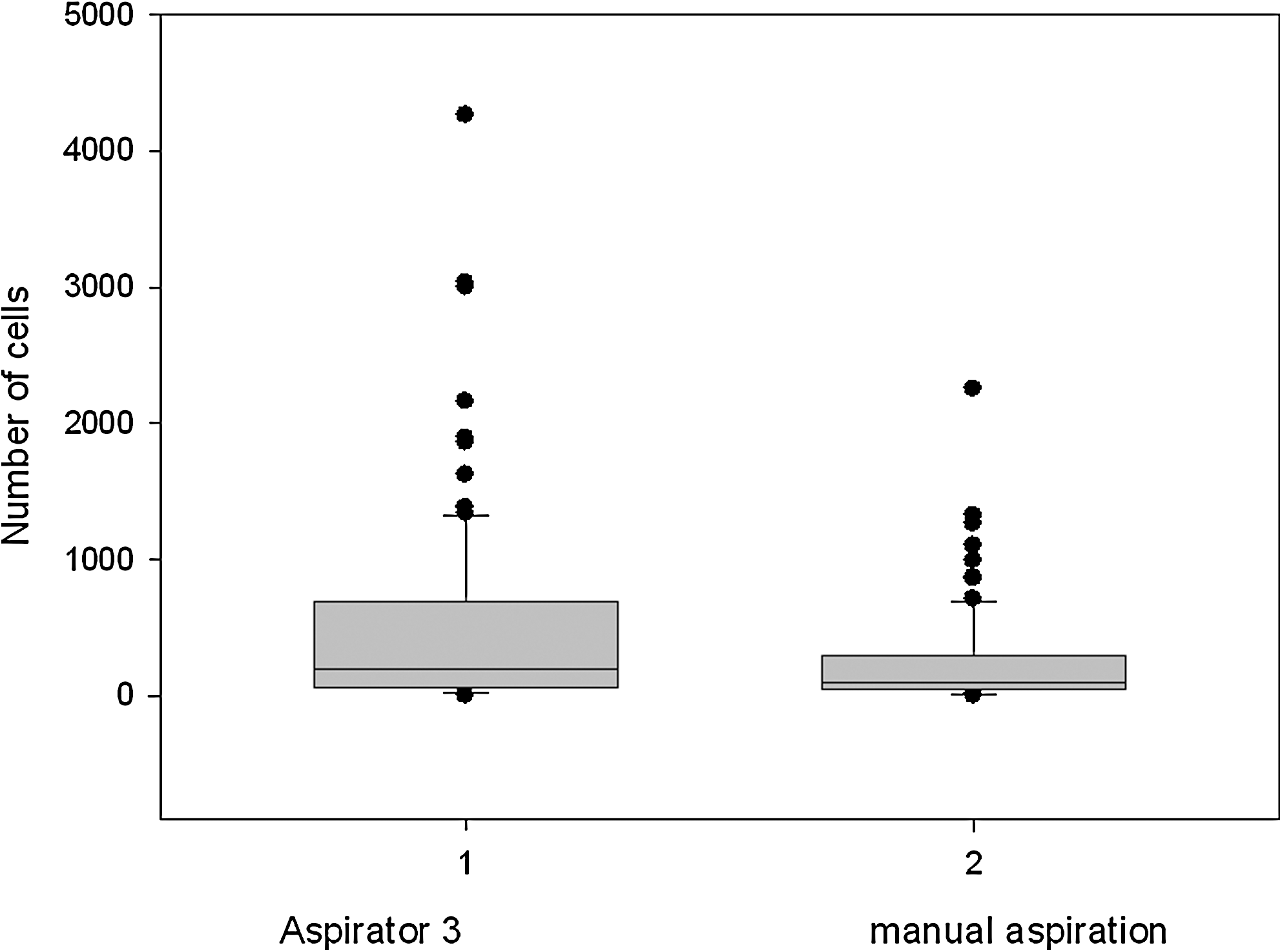
Comparison of the aspiration power of the Aspirator 3 versus manual technique in case of the total number of cells per patient. The median difference was statistically significant (p=0.005; Wilcoxon rank sum test).
In head-on-head comparison the Aspirator 3 aspirated more cell formations in 65 cases, whereas the manual technique aspirated more cell formations in 39 cases (Table 1). And the combination of these both biopsies lead to an increase of evaluable biopsies to 89% and 11% of all nodules that remained without evaluable results.
Moreover, the handling of the Aspirator 3 was convenient and easy to learn. As such, FNAB could be performed for even extremely small lesions (<4 mm in diameter).
Discussion
FNAB is a powerful technique in the diagnostic work-up of suspicious thyroid nodules (17). It is an easy technique to learn and has a low rate of complications. Many authors have already demonstrated the benefit of this technique in clarifying the nature of suspicious thyroid nodules (6,7,18 –20). Ultrasound guidance improves its specificity, and the use of the ThinPrep method especially improves the sensitivity of FNAB (6,7). The usual method is to aspirate the nodule, followed by fan-shaped movements of the needle and simultaneous evacuation of the syringe while disabling the negative pressure before the needle is removed. Some problems may arise, especially if the FNAB must be completed under sonographic control. First of all, it is not easy to biopsy accurately and to evacuate the syringe simultaneously. Despite the size of the lesions, the risk of dislocation from the nodule was quite high. Another problem was the number of cell formations in the aspirate. There have been several approaches to solving this problem, but no meaningful successes (4,5). To manage this problem, we evaluated a prototype of an automatic microaspirator (12,13). The results obtained with that device were promising, so we decided to further evaluate this new approach in a prospective clinical study. In the present study, we used a clinically approved aspirator (Aspirator 3) and compared it with the manual technique under highly standardized conditions. Each clinically suspicious thyroid nodule was biopsied twice by one experienced physician, first with the Aspirator 3 followed with the manual technique. The Aspirator 3 had, in total and on average, more cell formations and a higher total number of cells in the aspirate, compared with the manual technique. This difference was statistically significant. Approximately 19% of the FNABs with the Aspirator 3 and 24% with the manual technique had no material in the aspirate, this difference was not significant. It might be expected that because of hypervascularization of thyroid nodules a previous biopsy would cause bleeding leading to a lower sensitivity. This may be one reason for a lower sensitivity of the second biopsy. Additionally, the Aspirator 3 had more convenient handling. Through the automatic production of negative pressure by activating the foot pedal, it was able to biopsy several nodules in rapid succession. Because of the precise handling of the needle, it was possible to biopsy even small nodules (as small as 4 mm in diameter in our study) or small solid parts of cystic nodules or nodules in difficult surroundings, such as vessels. Therefore, the Aspirator 3 is a promising tool for biopsy of even extremely small lesions under special circumstances, as recently proposed (14,15).
The combination of these both techniques provided 89% evaluable biopsies. Even after double biopsies, there were no evaluable results for 13 nodules. This fact indicates that for some nodules the FNAB is not useful.
In conclusion, the Aspirator 3 is a promising tool for FNAB of thyroid nodules. In comparison with the manual technique, this tool aspirated more thyroid cells and cell formations. Moreover, the handling of the Aspirator 3 was convenient and easy to learn. As such, FNAB could be performed for even extremely small lesions.
Footnotes
Acknowledgment
Company selling the Aspirator 3: Labotect Labor-Technik-Göttingen GmbH, Rosdorf, Germany (
Disclosure Statement
The authors declare no potential conflicts of interest with respect to the authorship and/or publication of this article. None of the authors have ownership in the company that produces or markets the Aspirator 3, or consult or receive funding from these companies. The Aspirator 3 used in this study was not donated by the company that produces or markets the Aspirator 3.