
Abstract
Background:
Iodine deficiency (ID) remains common in Europe, and may be especially detrimental during pregnancy. The aim of our study was to assess iodine status and thyroid function in healthy pregnant women in the Lyon metropolitan area.
Methods:
In a cross-sectional study, healthy pregnant women (n=228) with no history of thyroid disease were consecutively recruited from an obstetric clinic during all trimesters. Thyrotropin (TSH), free thyroxine (FT4), anti-thyroid peroxidase (anti-TPO) antibodies, thyroglobulin (Tg), and urinary iodine concentration (UIC) (n=100) were measured. Thyroid functions were compared with those in a control group of nonpregnant adults.
Results:
The median (range) UIC was 81 (8–832) μg/L, and 77% of pregnant women had a UIC <150 μg/L, indicating inadequate iodine intake. Overall, 11% of women had abnormal TSH or anti-TPO. The median FT4 (pmol/L) was 14.9, 12.6, and 11.5 in the first, second, and third trimesters, respectively. The median Tg in pregnant women was 16.2 μg/L, did not differ across trimesters, and was significantly higher than in the control group of nonpregnant adults (11.7 μg/L) (p=0.02). Controlling for maternal age and week of gestation, UIC was not a significant predictor of any of the thyroid function tests.
Conclusions:
Pregnant women in the Lyon area are iodine deficient and have increased serum Tg concentrations compared with nonpregnant controls, likely due to physiological thyroid hyperstimulation during gestation exacerbated by ID.
Introduction
Thyroid disorders are the most common endocrine disorders in women of childbearing age and complicate ∼1%–2% of pregnancies (10). Consensus statements on clinical guidelines for the management of thyroid abnormalities during pregnancy and the postpartum period recommend targeted case finding either at the first prenatal visit or at the diagnosis of pregnancy (11,12). Hormonal changes and increased metabolic demands during pregnancy produce complex alterations in thyroid hormone concentrations (13). The changes include increased renal iodine losses, an estrogen-induced increase in thyroxin-binding globulin concentration, an increase in the tissue volume of T4 distribution, and increasing placental T4 degradation and transport. Those changes are dependent on the stage of gestation (10). Human chorionic gonadotrophin (hCG) also modulates TSH concentrations, and a decline in serum TSH occurs at the end of the first trimester at the time of the hCG peak. Thus, the interpretation of thyroid tests during pregnancy is challenging, and gestational age-specific reference intervals for most thyroid tests are likely necessary, as recommended by the US National Academy of Clinical Biochemistry (14). With regard to FT4, these reference intervals need to be method specific (15), because FT4 immunoassays are known to be sensitive to alterations in binding proteins (16 –18).
Several small regional studies have suggested that many French women may be iodine deficient during pregnancy (19 –21). However, more data on the iodine status in French women during pregnancy and the potential effects on thyroid function would be valuable, in order to make recommendations for improving iodine intakes in this important target group. Therefore, the aim of this cross-sectional study was to assess iodine status and thyroid function in healthy pregnant women in the Lyon metropolitan area.
Materials and Methods
Patients
Two hundred and twenty eight consecutive pregnant women attending the Groupement Hospitalier Est from Hospices Civils de Lyon either for first-semester termination of pregnancy (n=53) or for routine antenatal care (n=175) were enrolled between October 2008 and June 2009. The exclusion criteria as determined by a questionnaire were as follows: presence of chronic disease; iodine supplementation, including ingestion of iodine-containing multivitamin/mineral supplements; current or past thyroid disease; and/or multiple pregnancies. Approximately 25% of women declined participation in the study, ∼10% of women were excluded because of a personal history of thyroid disease and ∼5% due to a history of iodine supplementation. The study design was cross-sectional, and a single blood sample was taken from each woman at routine venepuncture. The sample was taken during the first trimester for women attending for termination, and at each of the three trimesters for women attending for antenatal care. A spot urine sample was collected for measurement of urinary iodine concentration (UIC) in a subset of 100 consecutive women for technical reasons. Written informed consent was obtained from all the enrolled subjects.
Controls
Reference intervals of thyroid tests were determined using blood from healthy local blood donors (men and nonpregnant women, age range: 18–50 years), for TSH (n=202), for FT4 (n=110), and for Tg (n=86). The healthy donors had no familial or personal history of thyroid disease or use of chronic medications or medication known to alter thyroid function (amiodarone, corticoids, propranolol, lithium, and/or neuroleptics). The number of control samples for the thyroid function tests varied, because the tests were performed at a different time when the new methodologies were adopted in the laboratory.
Methods
Each blood sample was analyzed for TSH, FT4, anti-thyroid peroxidase (anti-TPO), and Tg. The TSH was measured by chemiluminescence (Architect system; Abbott Laboratories). The FT4 was measured by electrochemiluminescence (Roche Diagnostics 2010 Elecsys). Anti-TPO antibodies were measured by radiometric assays (Dynotest anti-TPO, Brahms). Tg was measured by immunoradiometric assays (Cisbio International). The coefficient of variation for FT4 at 8.4 pmol/L was 4.6% and at 15.9 pmol/L, was 4.7%; at the level of 0.68 mUI/L it was 2.5% for TSH, and at 5 mUI/L, it was 2.5%; at the level of 0.6 μg/L it was 20% for Tg, and at the level of 8.3 μg/L, it was 10.7%. With these methods, the reference intervals for TSH and FT4 were 0.4 to 3.1 mIU/L and 11.1 to 18.8 pmol/L, respectively. The reference ranges from the control subjects were as follows: for TSH, 0.4 to 3.1 mIU/L; for FT4, 11.1 to 18.8 pmol/L; and for Tg, <45 μg/L. The UIC was measured at the Human Nutrition Laboratory in Zürich by using a modification of the Sandell–Kolthoff reaction (22). By this method, the CV for the UIC concentration is 10.0% at 47.7±0.6 μg/L and 12.7% at 79.5±0.8 μg/L.
Statistical analysis was performed by using Prism software. Normally distributed data were expressed as means±standard deviations (SDs); non-normally distributed data were expressed as medians (ranges). Comparisons among different groups were performed using Kruskall–Wallis followed by Dunn's test. Spearman and Pearson correlations were done to identify univariate relationships, and multiple regressions were done to examine predictors of thyroid function. The range of gestational ages for the first, second, and third trimester was 6–13 weeks, 14–27 weeks, and 28–38 weeks, respectively. The TSH concentrations were compared with the reference values from the controls as well as expert guidelines that suggest an upper recommended value for the first trimester of 2.5 and 3 mIU/L in the second and third trimesters (12). The UIC were compared with the WHO recommendations. According to WHO, the median UIC that indicates adequate iodine status in a population of pregnant women is 150 to 249 μg/L (7). p-values <0.05 were considered significant.
Results
Age and gestational age of the pregnant women are summarized in Table 1. Mean age was 29.6±5.6 years (min 15.3, max 45.7 years). There were fifty-three women in the first trimester, 107 in the second trimester, and 68 in the third. There was no difference between age at the second and third trimester (30.2 years, 30.2 years), while women in the first trimester were younger (27.4 years; p=0.0032).
Data are means±standard deviations with ranges in parentheses.
The overall median UIC during pregnancy was 81.1 μg/L (min 7.5, max 832.4 μg/L) (Table 2). Values in the first trimester were significantly lower than those in the second or third trimesters (p<0.05). Seventy-seven percent of our study population had a UIC below 150 μg/L, 58% below 100 μg/L, and 27% below 50 μg/L.
Data are medians with ranges in parentheses.
Comparison of UIC: I versus II, p<0.05; I versus III, p<0.05; II versus III, p>0.05.
UIC, urinary iodine concentration
Median TSH was 1.015 mIU/L for the whole group (Table 3). The TSH values in the first trimester were significantly lower compared with the second and the third trimesters (p<0.0001). The lowest values were observed between the tenth and twelfth weeks. The values rose during the second and third trimesters. There were no significant differences between the TSH values in the second and third trimesters, and they were in the normal range for the nonpregnant women. Log TSH and gestational age were positively correlated (p<0.001). During the first trimester, 3 women had a TSH below 0.1 mIU/L, 12 were below 0.3 mIU/L, and one was greater than 2.5 mIU/L. In the second trimester, all tested women had TSH values within the reference interval for nonpregnant women. The TSH values were between 2.5 and 3 mIU/L in five women, and during the third trimester, one woman had a TSH below 0.3 mIU/L, five were higher than 2.5 mIU/L and one was greater than 3 mIU/L (5.7 mIU/L). In total, eleven values were above 2.5 mIU/L.
Data are medians with ranges in parentheses.
Comparison of TSH: I versus II, p<0.001; I versus III, p<0.001; II versus III, p>0.05.
Comparison of FT4: I versus II, p<0.001; I versus III, p<0.001; II versus III, p<0.05; controls versus I, p>0.05; controls versus II, p<0.001; controls versus III, p<0.001.
Comparison of thyroglobulin: I versus II, p>0.05; I versus III, p>0.05; II versus III, p>0.05; controls versus I, p>0.05; controls versus II, p<0.001; controls versus III, p<0.05.
TSH, thyrotropin.
Anti-TPO antibodies were detected in 16 sera (7%) with 3 values just above the threshold of positivity (60 IU/mL) and three values greater than 1000 IU/mL. All women who had anti-TPO antibodies had TSH values in the normal range; those with the higher anti-TPO values (1490; 1530, and 2650 IU/mL) had TSH values 1.9, 1.4, and 1.1 mIU/L, respectively. The woman who had the highest TSH (5.7 mIU/L) was anti-TPO negative. Women with anti-TPO antibodies tend to be older than women without anti-TPO (31.5±1.3 years compared to 29.4±0.4), a nonsignificant difference. Thus, as a whole, 11% of women showed a biological abnormality in TSH or anti-TPO (25/228).
Free T4 decreased from the first to the third trimester (Table 3). The median free T4 was 14.9 pmol/L in the first trimester, 12.6 pmol/L in the second trimester, and 11.5 pmol/L in the third trimester. As shown in Figure 1, the values in the first trimester were not different from those of the nonpregnant controls but were higher as compared with those of the second and third trimesters. The values of FT4 in the second trimester were lower compared with the nonpregnant controls, and the values in the third trimester were lower compared with the nonpregnant controls and with the values in the second trimester (p<0.05). Moreover, log FT4 and stage of pregnancy were inversely correlated (p<0.001).
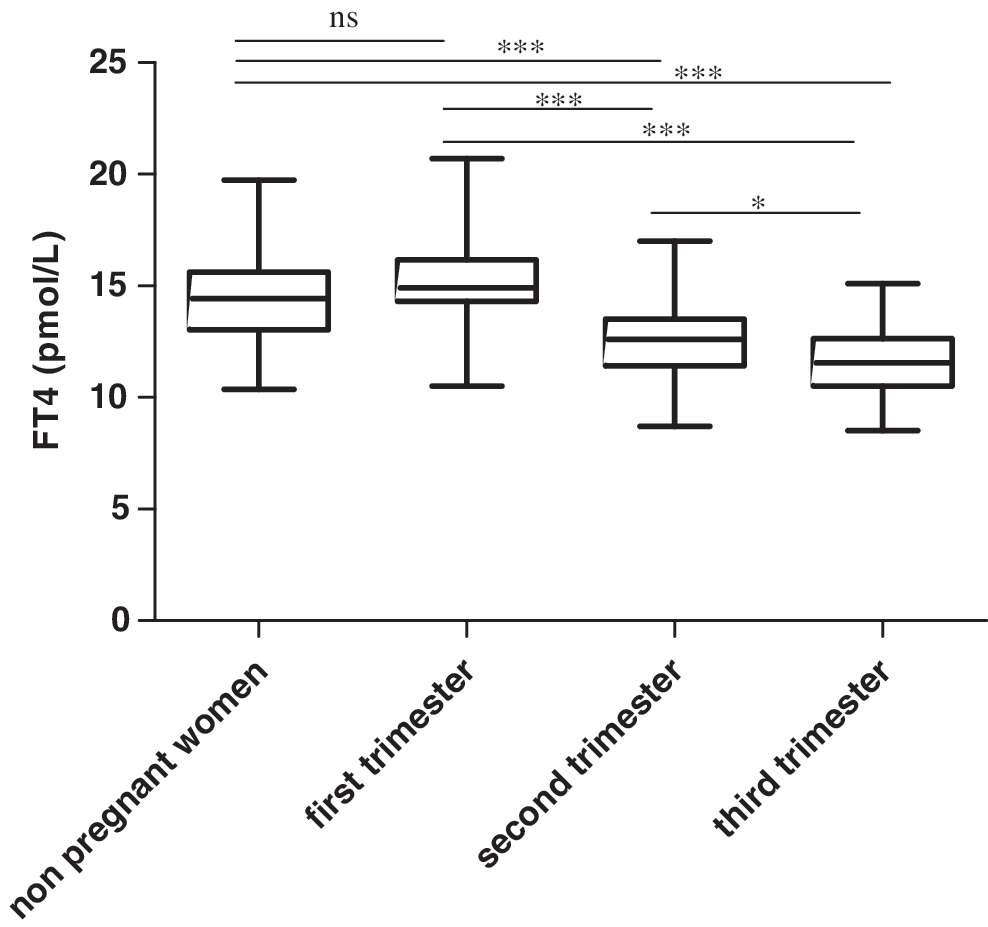
Comparison between FT4 levels and controls in each trimester. Distributions of FT4 are graphically summarized by boxes in which the central box represents the value from the lower to upper quartile (25th and 75th percentile, and the middle line represents the median). *p<0.05, ***p<0.001. ns, nonsignificant; FT4, free thyroxine.
The median Tg concentration in the population of pregnant women was 16.2 μg/L, and there were no significant differences in Tg values among the trimesters. The median value during pregnancy was significantly higher than in the nonpregnant controls (n=86, 11.7 μg/L) (p=0.02).
In univariate correlations, TSH was significantly inversely correlated with FT4 (r=−0.499; p<0.001) and TT4 (r=−0.177; p=0.020) but not significantly correlated with Tg (r=−0.017; p=0.802) or anti-TPO antibodies (r=0.054; p=0.417). In multiple regressions with TSH, FT4, and Tg as independent variables, and while controlling for maternal age and week of gestation, UIC was not a significant predictor of any of the four thyroid function tests (for TSH: β=−0.032, p=0.773; for FT4: β=−0.124, p=0.345; for Tg: β=−0.013, p=0.897).
Discussion
This cross-sectional study suggests that pregnant women in the Lyon area are iodine deficient: their median UIC was 81 μg/L, and 77% had a UIC <150 μg/L, indicating inadequate iodine intake. Although UIC was determined in a subset of only 100 subjects, they were a nested subgroup of consecutively recruited women who are likely to be representative of the total group. In addition, although the UIC were determined from a single spot-urine sample, spot sampling is recommended by the WHO for assessing iodine nutrition in populations of pregnant women, and the low UIC values are in accordance with the national French data estimating that iodine intake in the general population is <100 μg/day (23), below the recommended iodine intake of 150 μg/day for adults and 250 μg/day for pregnant women (7,24 –26). However, there are other factors that, in addition to iodine intake, may influence UIC during pregnancy (27,28). Thus, additional biomarkers of iodine nutrition during pregnancy would be valuable. Moreover, it is known that the negative regulatory effect of intra-thyroidal iodine on the goitrogenic effect of TSH is decreased in the case of ID (29). Whether this is the case also with hCG and in pregnancy has not been studied.
Tg is recommended by the WHO as an indicator of population iodine status in children, as elevated values reflect increased TSH stimulation due to ID (7). Tg may also be a useful marker of iodine nutrition in adults (30). Whether Tg may be a useful indicator of iodine status during pregnancy remains uncertain. In two small randomized controlled intervention studies that provided iodine supplements to pregnant women, ID increased Tg concentrations during pregnancy and the postpartum (31,32). In a cross-sectional study conducted on Italian pregnant women in the first trimester, mean±SD Tg (μg/L) was 10.2±9.2 in women with long-term iodized salt intake and a median UIC of 115 μg/L compared with 24.1±19.3 in women with short-term iodized salt intake and a median UIC of 63 μg/L (33). In a prospective study conducted on Spanish women (n=140) in a reportedly iodine-deficient area, median Tg (μg/L) in the first, second, and third trimesters, and one-year postpartum were 11.0, 11.0, 12.6, and 9.7, respectively; the levels were not significantly different between the semesters but were higher than in the postpartum (34). Similarly, in the present study, the Tg concentrations were significantly higher in pregnant women at each trimester than in nonpregnant controls, but did not significantly differ between the trimesters.
Laurberg et al. have suggested that pregnant woman have higher serum Tg concentrations than nonpregnant control women even in areas of iodine sufficiency due to increased thyroid stimulation to maintain euthyroidism (35). By contrast, Mandel et al. have argued that during gestation in women with no ID and no autoimmune thyroid disease, serum Tg across the trimesters and compared with postpartum remains essentially unchanged (15). Indeed, two studies conducted on iodine-deficient populations have suggested that there are no significant differences in Tg concentrations between pregnant and nonpregnant women. In a large study conducted in Sweden (36), mean±SD Tg (μg/L) was measured at gestational week 12 (15.48±1.96), week 22 (14.92±2.05), week 32 (18.55±2.8), and one-year postpartum (13.95±1.6); Tg concentrations were not significantly different among the timepoints. In iodine-sufficient women in the United States (37), the mean Tg concentrations did not differ between nonpregnant controls (n=104) and euthyroid pregnant women in the second trimester (n=49); mean±SD Tg was 14±10 and 16±10 μg/L, respectively. Overall, these studies and others (32,33) suggest, in iodine-deficient areas, that Tg increases during pregnancy and remains elevated across trimesters at a fairly consistent level, while in iodine sufficient areas, there is no or little increase in Tg during gestation. Thus, Tg shows promise as an indicator of ID in pregnancy, and would be complementary to UIC measurement. Future studies comparing Tg values in pregnant women and nonpregnant controls with different underlying iodine intakes would be useful to clarify this issue.
Our findings confirm those of others in that changes in thyroid hormone levels during pregnancy differ between the stages of gestation and between gestation and nonpregnant controls. The TSH values are comparable with those described in the literature (33,38 –41), with the lowest values found at about 10–12 weeks of gestation, at the time when the peak of hCG is maximal. In the second and third trimesters, TSH values tend to increase up to the reference range for nonpregnant women. The prevalence of anti-TPO antibodies was only 7% in our population, which corresponds to what is commonly described in women (42). The profile of the results of FT4 is also comparable with the literature (33,38 –40), with the T4 values negatively correlated with the stage of pregnancy, which stresses the limitations, during pregnancy, of applying the reference range for the nonpregnant population. Indeed, in our study, 18% (19/107) of the FT4 values obtained in the second trimester and 40% (27/68) in the third trimester are below what is considered normal in a nonpregnant population. Pregnancy reference ranges have been reported, but some from areas with different iodine status or ethnic populations (China, India, Canada) (39,43,44), and those ranges differed from ours. This is especially the case for the report from India, in which the FT4 ranges are much higher (12–19.45, 9.48–19.58, and 11.32–17.7 pmol/L) than ours, despite the same methodology. Indeed, Glinoer and Spencer recommended that thyroid function ranges should not only be trimester specific but also geography specific to account for differences in ethnicity and iodine intake (45).
Although the pregnant women in our sample were iodine deficient, variations in individual iodine intake, as reflected in UIC, did not appear to strongly influence the parameters of thyroid function. As expected, serum TSH increased and FT4 decreased over gestation, but there was no correlation of maternal serum thyroid hormones, TSH, or Tg with maternal UIC. These findings are consistent with those of other recent studies, including a population in northern France (20). Possible reasons for the lack of correlation include the small sample size and the well-recognized wide inter-day variability in UIC from spot collections, precluding the assessment from spot urine samples of the individual iodine status (46). However, it is also possible that, although their iodine intakes were low, these pregnant women are able to maintain the euthyroid state by drawing on thyroidal iodine stores and thyroidal adaptation (as reflected by increased Tg, suggesting thyroid hyperstimulation).
However, iodine status estimated from a single spot sample is a weak measure of individual iodine intake, which is probably not sufficient to provide an accurate estimation of iodine intake (46). A sequential measurement of UIC during pregnancy in a larger sample would provide a more accurate evaluation of the iodine status in pregnant French women. Improved monitoring may be important while considering the results of a recent French survey indicating a median UI of 127 μg/L in nonpregnant women (47).
It is important to maintain adequate FT4 values during pregnancy in light of several studies linking subclinical hypothyroidism or hypothyroxinemia with neurodevelopmental delay (8,14,48,49). The question of thyroid screening during pregnancy is currently debated; in our sample, given the very low frequency of thyroid abnormalities, case finding and targeted screening would likely be more appropriate. However, larger epidemiological studies in our populations are warranted.
In Europe, several randomized controlled trials of iodine supplementation of mild-to-moderate iodine-deficient pregnant women have been performed. Iodine reduced maternal and newborn thyroid size, and, in some, decreased maternal TSH. However, none of the trials showed an effect on maternal and newborn total or free thyroid hormone concentrations, which is the most important outcome (2,50). However, since no controlled trial in mild-to-moderate iodine-deficient pregnant women has measured long-term clinical outcomes or infant development, whether this degree of maternal ID has detrimental effects remains uncertain. Until more data on this issue become available, it may be prudent to ensure adequate iodine intakes during pregnancy by iodine supplementation, as recommended by expert organizations (American Thyroid Association recommendation). Iodine supplementation should, thus, be considered for pregnant women in the Lyon area and other European countries, who are mild-to-moderately iodine deficient and show signs of thyroid hyperstimulation.
Footnotes
Disclosure Statement
No competing financial interests exist.