
Abstract
Background:
Thyroid nodules with fine-needle aspiration (FNA) readings of nondiagnostic or atypia of undetermined significance (AUS), also referred to as follicular lesion of undetermined significance (FLUS) are problematic for their optimal management. The usefulness of performing a core-needle biopsy (CNB) to clarify whether these nodules are benign or malignant has not been established. The purpose of the present study was to determine whether CNB provides better diagnostic information than repeat FNA (rFNA) in thyroid nodules having nondiagnostic or AUS/FLUS readings.
Materials and Methods:
The Bethesda System for Reporting Thyroid Cytopathology was used for FNA readings and for CNB readings. The study included 225 thyroid nodules from 220 consecutive patients who previously had nondiagnostic (Group N-DIAG, n=64) or AUS/FLUS (Group AF, n=161) FNA readings. All patients simultaneously underwent rFNA and CNB of each nodule. The nondiagnostic and AUS/FLUS readings by rFNA and by CNB were compared. The diagnostic sensitivities of rFNA and CNB for malignancy in thyroid nodules were also assessed. Statistical analysis was performed using a McNemar's test.
Results:
In N-DIAG Group, the nondiagnostic readings for the CNBs were lower than that those for rFNAs (1.6% vs. 28.1%, p<0.001). In the AF Group, the AUS/FLUS readings for the CNBs were lower than those for the rFNAs (23.6% vs. 39.8%, p<0.001). The inconclusive diagnoses (nondiagnostic or AUS/FLUS) for the CNBs were lower than those for the rFNAs in Group N-DIAG (12.5% vs. 45.3%, p<0.001) and Group AF (26.7% vs. 49.1%, p<0.001). The sensitivity of CNB for thyroid malignancy was higher than that of rFNA in Group N-DIAG (100% vs. 71.4%, p=0.125) and Group AF (78.5% vs. 55.4%, p<0.001).
Conclusion:
After patients have had one FNA of a thyroid nodule yielding inconclusive diagnostic results (nondiagnostic or AUS/FLUS), CNB is more useful than rFNA for reducing the frequency of inconclusive diagnostic results. CNB will improve the diagnostic performance for malignancy more than rFNA in thyroid nodules that on the first FNA had nondiagnostic or AUS/FLUS readings.
Introduction
According to the recently proposed Bethesda System for Reporting Thyroid Cytopathology (7,8), the categories for indeterminate nodules are AUS/FLUS, follicular neoplasm or suspicious for follicular neoplasm (FN/SFN), and suspicious for malignancy. The Bethesda System recommends repeat FNA (rFNA) for the management of nodules with nondiagnostic and AUS/FLUS readings due to their low risk of malignancy (1–4% and 5–15%, respectively). Unfortunately, rFNA does not seem to be a satisfactory solution for these nodules because a nondiagnostic reading is again obtained in 17–47% in nodules with previous nondiagnostic readings (1,2,9,10) and nondiagnostic and AUS/FLUS readings occur in 1–7% and 19–31% of cases of nodules with previous AUS/FLUS FNA readings (1,3).
Core-needle biopsy (CNB) provides a larger tissue sample and may facilitate a more precise histological diagnosis (11). Unlike the old technique of nonimage guided large needle biopsy, US-guided CNB using a modern spring-activated biopsy needle is reported to be a safe and well tolerated procedure (12 –21). Although CNB may be advantageous in cases of thyroid nodules that were read as “nondiagnostic” by FNA, it is controversial as to whether CNB is better than FNA for sample adequacy and diagnostic accuracy (12,13,15,16,18 –23). A complementary role of CNB has been suggested for investigating thyroid nodules (7,23) but this has been minimally investigated (21) and the clinical indications for CNB have not been established.
The present study was performed to test the hypothesis that CNB provides better diagnostic information than a rFNA in thyroid nodules that initially had nondiagnostic or AUS/FLUS readings on their initial FNA. To test this hypothesis, we prospectively evaluated the frequency of nondiagnostic and AUS/FLUS readings for rFNAs and for CNBs in thyroid nodules whose initial FNA was read as nondiagnostic or AUS/FLUS.
Materials and Methods
Study design and enrollment criteria
Patients in this study were classified into two subgroups. Group N-DIAG consisted of patients who had thyroid nodules whose initial FNA reading was nondiagnostic. Group AF consisted of patients who had thyroid nodules whose initial FNA reading was AUS/FLUS FNA. The primary end point of the study was diagnostic efficacy; the rate of nondiagnostic readings in Group N-DIAG and the rate of the AUS/FLUS readings in Group AF. The secondary end point was diagnostic sensitivity for malignancy. The inclusion criteria for entering the study were as follows: (i) patients who had thyroid nodules with previous nondiagnostic FNA readings (except for thyroid cyst) (Group N-DIAG) or (ii) patients who had thyroid nodules with previous AUS/FLUS FNA readings (Group AF). Exclusion criteria were as follows: (i) patients with bleeding tendencies or patients receiving anticoagulation therapy, (ii) patients who had nodules with high risk for hemorrhage (abundant perinodular vessels or risk of perithyroidal vessel injury), and (iii) patients with nodules that were not technically feasible for performing a successful CNB procedure. Coagulation screening was not routinely performed. In patients receiving antiplatelet therapy, CNB was performed after discontinuing these medications for one week. Institutional review board approval was obtained for this prospective study and informed consent was obtained from all patients.
Patients
From February 2009 to January 2010, 236 patients from three institutions, having 241 thyroid nodules, were consecutively enrolled in this study. All study-eligible patients underwent simultaneous FNA and CNB of each thyroid nodule. Sixteen (6.4%) nodules were excluded from the study for several reasons: anticoagulation therapy (n=1), high risk for hemorrhage (n=3), technically infeasible location of the nodules (n=8), failed needle penetration due to dense severe calcifications of the nodules (n=2), hematoma after FNA (n=1), and difficulty in identifying the a target nodule among multiple thyroid nodules (n=1). In total, 225 thyroid nodules (Group N-DIAG, 64 nodules; Group AF, 161 nodules) in 220 patients (191 women, 29 men; mean age, 46±11.7 years) were included in this study. The final diagnoses were obtained in 149 nodules (Group N-DIAG, 45; Group AF, 104). For malignant nodules (n=79), this diagnosis was based on histopathological readings after surgical resection. For benign nodules (n=70), this diagnosis was based on histopathological readings after surgical resection in 21 (30%), or benign cytology readings of FNAs that had been repeated at least two times (n=7, 10%) or benign readings of FNA or CNB and a decrease in size (maximal diameter) by more than 50% at follow-up (n=2, 2.9%), or a concordant benign reading of FNA and CNB (n=40, 57.1%). We used “benign follicular nodule” as the term for benign nodules that were not diagnosed by surgical resection. All follicular adenomas were diagnosed by histopathology readings.
US-guided FNA and CNB procedures
High-resolution color Doppler US using a 10–12 MHz linear transducer (iU22, Philips Medical Systems, Bothell, WA; AplioXG, Toshiba, Otawara-shi, Japan) was employed for the guidance of FNA or CNB. FNA and CNB procedures were performed by three experienced thyroid radiologists (D.G.N., J.K., and J.Y.S.) with 13, 5, and 6 years of experience, respectively, in performing thyroid US. They had an experience of reading more than 4000 cases of FNA and 100 cases of CNB.
In all cases, a comprehensive US evaluation of the neck and thyroid gland was performed, and the size, location, composition, and vascularity of nodules were evaluated. In all cases the rFNA was performed before the CNB with 1% lidocaine being administrated as local anesthesia. For the rFNA, a combination of 25-, 23-, and 21-gauge needles and a combination of capillary and aspiration FNA techniques were used according to the characteristics of nodules. Direct smears were made in all cases, and all smears were immediately fixed with alcohol after rFNA and stained with Papanicolaou. Cell blocks were also made for some cystic nodules or bloody aspirates. The number of needle passes was determined by the operator during the rFNA procedure, and a maximum of four needle passes was permitted for each nodule.
After rFNA, CNB was performed using a disposable 18-gauge, double action spring-activated needle (1.1- or 1.6-cm excursion) (TSK Ace-cut; Create Medic, Yokohama, Japan). Using a freehand technique, the end of the biopsy needle was advanced into the edge or within the nodule, and the stylet and cutting cannula of the needle were sequentially fired. In some nodules, a prefired biopsy needle was introduced into the nodule and a final second firing for cutting the specimen was performed. A second or third CNB was performed when the lesion was considered inaccurately targeted in the case of small nodules or when an adequate tissue core was not obtained by visual inspection. Tissue cores were placed in 10% buffered formalin immediately after the procedure and conventionally processed. After biopsy, each patient was observed with a firm, local compression of biopsy site for 20–30 minutes.
Cytology and histology analysis
FNA cytology and CNB histology specimens were reviewed by staff histopathologists. FNA cytology diagnoses were categorized into six categories according to the Bethesda System for Reporting Thyroid Cytopathology (7,8): nondiagnostic, benign, AUS/FLUS, FN/SFN, suspicious for malignancy, and malignant. The diagnostic criteria of CNB have not been standardized for thyroid nodules. For this study, CNB histology diagnoses were categorized into the same six categories of the Bethesda System according to the histopathology result of CNB. A Nondiagnostic CNB reading included absence of any identifiable follicular thyroid tissue, presence of only normal thyroid gland, and tissue containing only few follicular cells insufficient for diagnosis. The AUS/FLUS reading for CNB included nodules in which some atypical cells were present but were not diagnostic of suspicious malignancy or malignant tumor, and included cellular follicular nodules in which a distinction between follicular neoplasm and hypercellular hyperplastic nodule was not possible. Nodules with histology features favoring follicular neoplasm were categorized as “suspicious for follicular neoplasm or follicular neoplasm”. Immunohistochemistry was not employed as a basis for these readings.
Data collection
According to protocol the size, location, and composition of nodules were recorded at the time of biopsy, along with details of the biopsy site, needle gauge for the rFNA, needle type for the CNB, number of needle pass or biopsy core, and nature of immediate complications. The medical records were reviewed by two of the authors (D.G.N. and J.Y.S.) one to two years after the thyroid biopsy to determine the final diagnosis and any delayed complications.
Statistics
Statistical analysis was performed with the software package (SPSS, version 16.0 for Windows; SPSS, Chicago, IL). We calculated the rates obtained for the diagnoses as obtained by rFNA and by CNB in the Groups N-DIAG and AF. We calculated the sensitivity, specificity, positive predictive value, negative predictive value, and accuracy of rFNA and CNB for diagnosis of thyroid malignancy in Group N-DIAG and in Group AF, and we calculated diagnostic values for a diagnosis of thyroid neoplasm in Group AF. The McNemar's test was used to compare the rates of for each diagnosis obtained by rFNA and CNB and to compare the diagnostic sensitivity of rFNA and CNB. The Mann-Whitney U test was used to compare the number of needle passes required for nodules with nondiagnostic and diagnostic FNA results. A statistically significant difference was defined as p<0.05.
Results
Demographic data
For all patients, the rFNA and CNB procedures were performed at an outpatient radiology thyroid clinic. The size of thyroid nodules ranged from 3 to 51 mm (median, 10 mm) in Group N-DIAG, and from 3 to 80 mm (median, 9 mm) in Group AF. The number of needle passes for FNA ranged from 1 to 4 (mean, 2.0) in both of these Groups. In Group N-DIAG, the mean number of needle passes that were performed was not significantly different between nondiagnostic and diagnostic readings (2.1 vs. 2.0, respectively, p=0.548). In Group AF, the mean number of needle passes was slightly higher in nodules with nondiagnostic results than that in nodules with diagnostic results (2.4 vs. 1.9, respectively, p=0.048). The number of tissue cores obtained by CNB ranged from 1 to 3 (mean, 1.6) in both groups. A 1.1-cm excursion needle was used for 222 biopsies (98.7%), and a 1.6-cm excursion needle for 3 biopsies (1.3%). In the Group N-DIAG there were 62 (96.9%) solid nodules, 1 (1.6%) predominantly solid nodule, and 1 (1.6%) predominantly cystic nodule. In the Group AF there were 148 (91.9%) solid nodules, 9 (5.6%) predominantly solid nodules, and 4 (2.5%) predominantly cystic nodules according to conventional criteria (24).
Final diagnoses were obtained in 45 (70.3%) of the 64 nodules in Group N-DIAG and in 104 (64.6%) of the 161 nodules in Group AF. The final diagnoses for Group N-DIAG nodules were 31 benign nodules (1 nodular hyperplasia, 25 benign follicular nodules, and 5 follicular adenomas) and 14 papillary carcinomas. The final diagnoses for Group AF nodules included 39 benign nodules (7 nodular hyperplasia, 25 benign follicular nodules, and 7 follicular adenomas) and 65 malignant nodules (56 papillary carcinomas, 8 follicular carcinomas, and 1 medullary carcinoma).
Diagnostic efficacy
Listed in Tables 1 and 2 are the diagnostic results of rFNA and CNB in the N-DIAG and AF groups. In the N-DIAG group, the nondiagnostic readings for rFNA was 28.1% and that for CNB was 1.6% (p<0.001) (Fig. 1). Inconclusive diagnoses, including nondiagnostic and AUS/FLUS readings, were found in 29 (45.3%) of 64 nodules by rFNA and in 8 (12.5%) nodules by CNB (p<0001). In one nodule, for which a nondiagnostic reading was obtained by CNB, the histopathology showed only fibrovascular tissue.
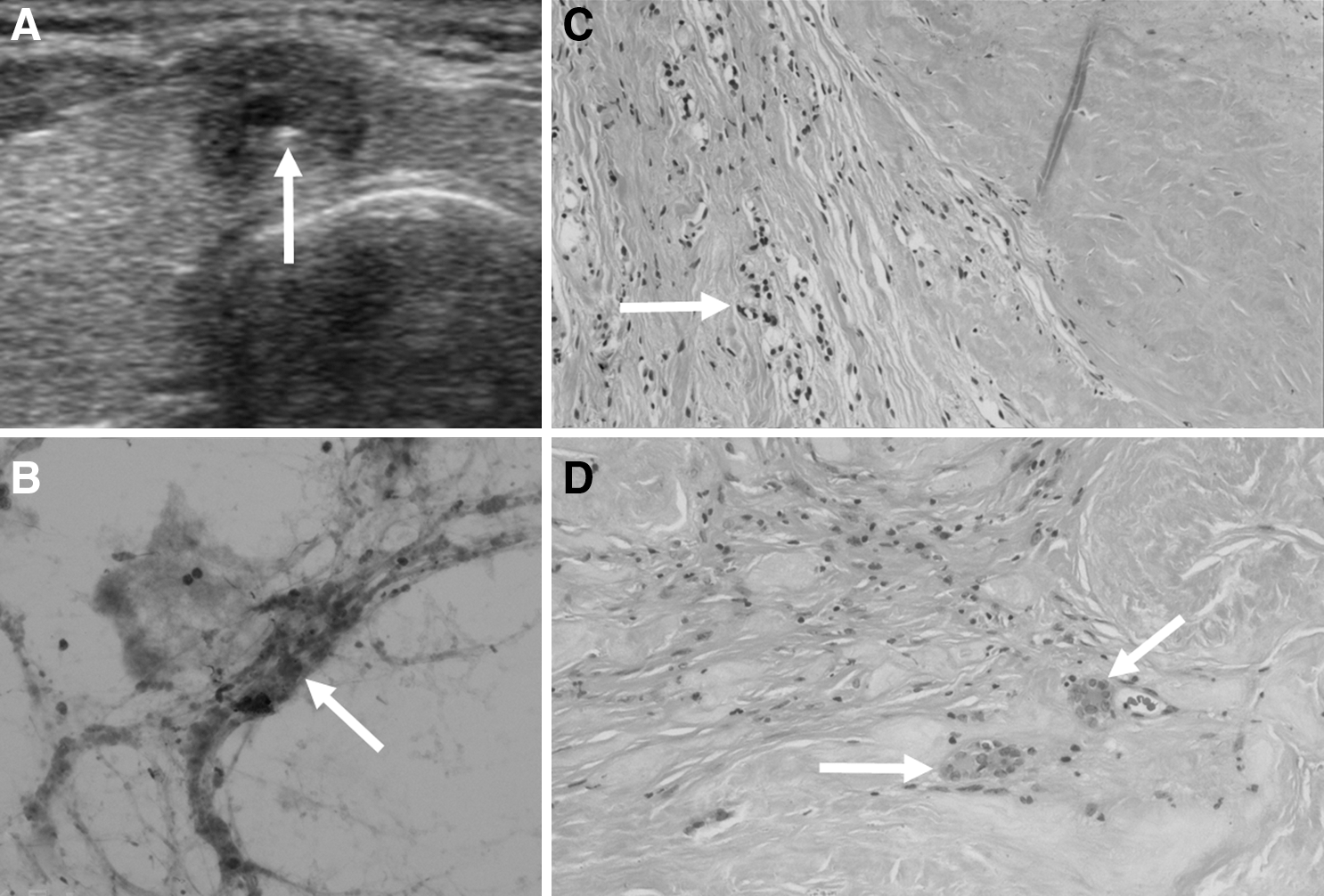
Ultrasound (US), fine-needle aspiration (FNA) cytology, core-needle biopsy (CNB) histology, and surgical pathology of a benign fibrotic nodule with previous nondiagnostic FNA reading.
Comparison of diagnosis of rFNA and CNB in nodules initially read as nondiagnostic.
AUS/FLUS, atypia of undetermined significance or follicular lesion of undetermined significance; CNB, core-needle biopsy; FN/SFN, follicular neoplasm or suspicious for follicular neoplasm; rFNA, repeat fine-needle aspiration.
Comparison of diagnosis between rFNA and CNB in nodules initially read as AUS/FLUS.
In the AF group 39.8% of the rFNA readings were AUS/FLUS and 23.6 % of the CNB readings were AUS/FLUS (p<0001) (Fig. 2). Inconclusive readings (including nondiagnostic and AUS/FLUS readings) were obtained in 79 (49.1%) of 161 nodules by rFNA and in 43 (26.7%) nodules by CNB (p<0001). The nondiagnostic rate for rFNA was 9.3% and that for CNB was 3.1% (p=0.041) in the AF group.
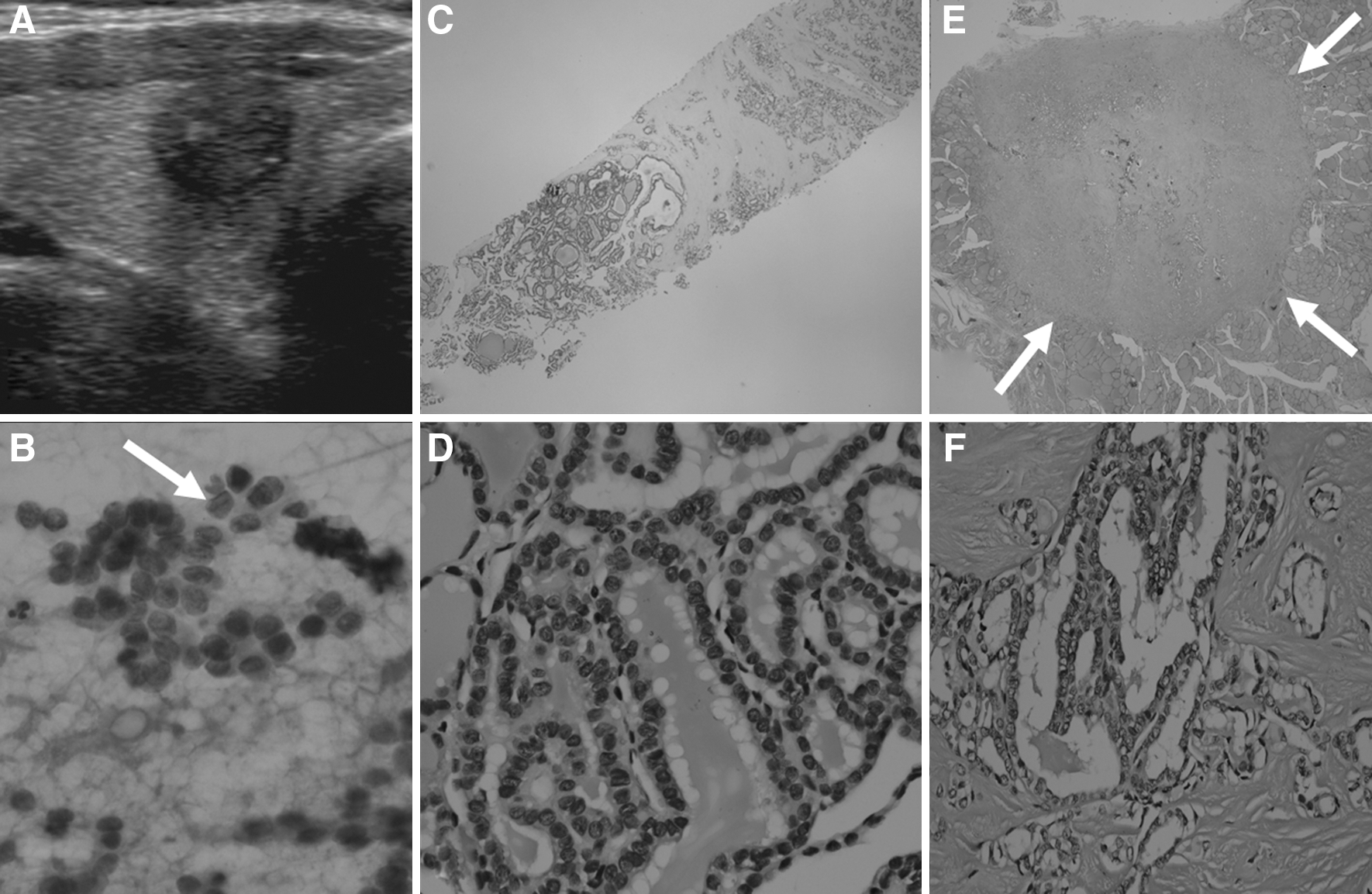
US, FNA cytology, CNB histology, and surgical pathology of papillary carcinoma with previous atypia of undetermined significance or follicular lesion of undetermined significance (AUS/FLUS) reading.
When FNA and CNB were combined there were no nondiagnostic readings in either the N-DIAG or AF groups. In five cases of a nondiagnostic reading by CNB alone, the histology specimens contained a few follicles with severe fibrosis (n=2), a few follicles with a normal gland (n=1), or normal thyroid gland only (n=2).
Diagnostic agreement between FNA and CNB
Supplementary Tables S1 and S2 (Supplementary Data are available online at
Diagnostic accuracy for malignancy
Using the criteria of Bethesda System category 5 (suspicious for malignancy) and 6 (malignancy), the diagnostic sensitivity of CNB for thyroid malignancy was higher than that for rFNA, but this was not statistically significant (p=0.125) in the N-DIAG group. In the AF group, the sensitivity of CNB for Bethesda System catagories 5 and 6 was significantly higher than that of rFNA (p=0.001) (Table 3).
Bethesda category 5 indicates suspicious malignancy and category 6 indicates malignancy.
In Group AF, the sensitivity of CNB was significantly higher than that of rFNA for the Bethesda System categories 4 (FN/SFN), 5, and 6 (malignancy, 80% vs. 55.4% and neoplasm, 76.4% vs. 50%, p<0.001, respectively). When final diagnosis of malignancy included only papillary carcinomas, the sensitivities of FNA and CNB for the Bethesda System categories 5 and 6 were 63% and 91.9%, respectively (p<0.001).
There were no cases of false positive diagnosis for the Bethesda System category 6 for both the combined results of rFNA and CNB. There was no false negative case by CNB, and one false negative case by rFNA for the Bethesda System category 2 (benign). In the AF group, the final CNB AUS/FLUS diagnoses were 5 (26.3%) for benign non-neoplastic nodules, 4 (21.1%) for follicular adenomas, and 10 (52.6%) for malignant tumors.
Complications
There were no major complications in either the N-DIAG or AF groups. In eight (3.6%) patients, small perithyroidal hematomas were demonstrated and in 5 (2.3%) patients, mild transient parenchymal edema occurred. None of these patients required hospital admission or intervention. There were no cases of needle track metastases at follow-up.
Discussion
Our study demonstrated the significantly lower rate of nondiagnostic readings obtained by CNB in the N-DIAG group and a lower rate of AUS/FLUS readings obtained by CNB in AF group compared with the results obtained by rFNA. In both groups, the rate of inconclusive diagnosis, including nondiagnostic and AUS/FLUS readings was significantly lower in readings obtained CNB compared with those obtained by rFNA.
Our data suggest that CNB can effectively reduce nondiagnostic readings compared with rFNA in nodules with previous nondiagnostic FNA readings. Our data also suggest that the combination of FNA and CNB can eliminate nondiagnostic readings in most cases. An unsatisfactory specimen obtained by FNA is the major cause of false-negative rate of FNA in the diagnosis of thyroid malignancy (25). The adequacy of FNA is highly dependent on the skill and experience of the operator; nondiagnostic readings of FNA are related to operator factor (skill and experience) and inherent nodule characteristics. These include a small amount of follicular cells due to severe fibrosis or calcification, nodules that easily bleed and result in bloody aspirate, and cystic nodules. Although the number of needle passes for FNA in our study was less than the four to six passes recommended as the optimal number (26), the number of needle passes of nodules with nondiagnostic FNA readings was similar or slightly higher than nodules with diagnostic readings. The diagnostic adequacy of FNA depends not only on the number of needle passes but also on many other factors. In our study, FNA procedures were performed by experienced operators who tried to get enough tissue sample at each FNA needle pass. The number of needle pass for each nodule was mostly determined by visual inspection of the aspirated specimen. Notably, our nondiagnostic rate of FNA in the N-DIAG group was slightly lower than the mean nondiagnostic rate (30%) in cumulative data from four previous studies of rFNA of thyroid nodules having initial nondiagnostic FNA results (1,2,9,10). The higher adequacy rate of CNB may be due to several factors. First, CNB depends less on operator skill if the needle successfully penetrates the nodule, and second, a tissue core contains a greater number of cells. Considering the operator factor relating to nondiagnostic FNA results, CNB will have a complementary role for some cases of thyroid nodules having nondiagnostic FNA results.
A recent retrospective study by Park et al. (21) reported that the rate of a nondiagnostic or indeterminate result was 48.6% for rFNA and that of for CNB was 1.8% in thyroid nodules that were indeterminate by previous FNA. Our data also shows that CNB significantly lowered the rate of inconclusive (nondiagnostic or AUS/FLUS) reading compared with rFNA. Although the reason for the lower AUS/FLUS rate of CNB than rFNA needs further investigation, it may be related to the larger tissue sample and additional histological information as obtained by CNB as compared with FNA cytology. Although it is difficult to separate a cellular hyperplastic nodule from a follicular neoplasm (23), our data showed a significantly higher diagnostic rate of follicular neoplasm by CNB compared with that by FNA in both of our groups. We usually obtained tissue cores containing a nodular margin and normal tissue in nodules with indeterminate US features, suggesting the possibility of a follicular neoplasm (24,27). Further investigations are needed to determine whether CNB might be helpful in separating a nodule with cellular hyperplasia from a follicular neoplasm (11,28 –30).
In addition to the higher adequacy rate of CNB, our data suggest that CNB is more sensitive for the prediction of malignancy, especially papillary carcinomas in thyroid nodules with previous AUS/FLUS readings. Because CNB had no false negative case within the benign category, nodules with nondiagnostic results or AUS/FLUS readings by rFNA and benign result by CNB may be managed as benign nodules. Therefore, theoretically, an additional biopsy procedure or surgery could have been avoided in the 16 nodules (25%) in the N-DIAG patients and in the 16 nodules (10%) in the AF patients. The high prevalence of malignancy in our study may be related to a bias in patient selection. Because many of benign nodules were not confirmed by surgery and the number of thyroid nodules with final diagnosis is limited in this study, diagnostic accuracy of CNB needs to be further investigated in a large series study.
Although CNB has a higher efficacy in the diagnosis of nondiagnostic or indeterminate nodules than rFNA, combining this with FNA will be more effective for accurate diagnosis in small nodules and nodules with severe fibrosis or calcifications or insufficient tissue core by visual inspection to reduce the problems of sampling error with CNB. Compared with FNA, CNB may be technically not feasible in some cases and CNB also has the disadvantages of possibly more patient discomfort, the necessity of local anesthesia, and the need for an adequate training period, a specific skill, and more experience in image-guided thyroid intervention for performing CNB. The lack of diagnostic category standardization in the histology diagnosis of CNB is another issue requiring further research and a limitation of this study.
In conclusion, CNB is more useful for reducing inconclusive diagnoses than rFNA and will have a useful complementary diagnostic role for an optimal management of thyroid nodules with previous nondiagnostic or AUS/FLUS FNA readings.
Footnotes
Acknowledgment
This study was supported by the research fund of Seoul R&BD Program (ST100011M0209721).
Disclosure Statement
No competing financial interests exist.