
Abstract
Background:
Graves' orbitopathy is an inflammatory orbital disease that represents the commonest extrathyroidal manifestation of Graves' disease. Autoimmune pancreatitis (AIP) is a rare inflammatory disease characterized by prominent lymphocytic infiltration and fibrosis of the pancreas causing organ dysfunction.
Summary:
This report provides the first clinical description of severe Graves'-like orbitopathy occurring in association with AIP. Although there was no clear evidence of autoimmune thyroid disease or dysfunction in our patient, the clinical course of his orbitopathy was related to that of AIP, the relapses of orbital inflammation being temporally coincident.
Conclusions:
Our data suggest that shared autoantigens between the pancreas and the orbit might be responsible for the unusual disorder observed in our patient.
Introduction
Autoimmune pancreatitis (AIP) is a rare inflammatory disease characterized by prominent lymphocytic infiltration and fibrosis of the pancreas leading to organ dysfunction (3,4).
We hereby report the case of a Caucasian male in whom an apparently typical Graves' orbitopathy was detected in association with AIP in the absence of any clear feature of autoimmune thyroid disease. This report constitutes the first clinical description of such an unusual disease entity.
Case Report
A 58-year-old male was referred to our unit in February 2007 for a prevalently monolateral orbitopathy. The eye disease had appeared nearly 2 years before (Table 1, March 2005). On magnetic resonance imaging (MRI) of the orbit (May 2005), swelling of the left extraocular muscles (medial, lateral, and superior recti) and a left eye proptosis were evident. Free thyroid hormones and thyrotropin (or) thyroid-stimulating hormone (TSH) were in the normal range; tests for antithyroglobulin (anti-TgAb), antithyroid peroxidase (anti-TPOAb), and anti-TSH receptor antibody (anti-TRAb) were negative. Three months after the eye disease had appeared, the patient developed an itching cholestatic jaundice with no abdominal pain. Laboratory tests revealed high total bilirubin, alanine transaminase and aspartate transaminase, lipase and carbohydrate antigen (CA) 19.9. Ultrasound (US) examination and computed tomography of the abdomen showed a dilated distal hepatocolic duct (17 mm). The pancreas had a hypoechogenic and dyshomogeneous structure and a head markedly increased in size. These findings were consistent with a diagnosis of chronic pancreatitis. An endoscopic echography-driven fine needle biopsy of the pancreatic head excluded the neoplastic nature of the disease. The pancreatic fine needle biopsy showed an inflammatory infiltrate containing granulocytes, lymphoid cells, and histiocytes associated with microaggregates of cylindrical epithelial cells deprived of neoplastic features.
As assessed by European Group on Graves' Orbitopathy recommendations. Activity measure is based on the classical features of inflammation, clinical activity score (CAS) is the sum of all items present. A CAS R3/7 indicates active Graves' ophthalmopathy. Negative findings are not shown, they include: spontaneous retrobulbar pain; optic nerve involvement; corneal involvement.
MRI, magnetic resonance imaging.
Autoimmune serology demonstrated negative tests for antiglucosaminidase, anti-tyrosin-phosphatase protein (IA2), antineutrophils (cANCA, pANCA), anti-smooth-muscle, antimitochondrial, anti-parietal-cells, anti-extractable-nuclear-antigen, antigliadin, antitransglutaminase, and antiendomysium antibodies. Antinuclear antibodies were weakly positive (1:80). The rheumatoid factor test was also negative and complement components (C3 and C4) were in the normal range.
The patient was treated with oral corticosteroid therapy: methylprednisolone 16 mg bid for about 8 months (from June 2005 to February 2006), achieving a significant decrease of CA 19.9, a normalization of liver transaminases and a resolution of cholestatic jaundice. A partial improvement of his eye signs and symptoms was also observed (Table 1, March 2006). In February 2007, 1 year after corticosteroid treatment had been withdrawn, the eye disease recurred and the patient was referred to our department. Ocular examination is reported in Table 1 (February 2007).
Laboratory parameters of thyroid function were in the normal range; tests for TPOAb, TgAb, and TRAb were all negative. At US evaluation, the thyroid was of normal size with a dyshomogeneous and slightly hypoechogenic pattern. An MRI of the orbit revealed similar findings as the previous one. Meanwhile, the patient suffered a relapse of cholestatic jaundice. Serum transaminases, amylase, and bilirubin were high. The serum concentration of total immunoglobulin G (IgG) was high (2.130 mg/dL, normal range 800–1.600). Subtype analysis of circulating IgG revealed high serum levels of IgG 4 (13.100 mg/L, normal range 80–1.400). At abdominal US a dilated coledoc (12 mm) and a markedly increased in size pancreatic head (3×4 cm) were also evident. According to the Mayo Clinic criteria (5), a diagnosis of a Type 1 AIP was rendered. The typical features of AIP and the differential diagnosis between Type 1 and Type 2 AIP are reported in Table 2.
Modified from Park et al. (4).
AIP, autoimmune pancreatitis.
Oral treatment with prednisone (40 mg) was initiated. When treated with steroids, the patient developed diabetes mellitus that required insulin therapy. Four weeks later an improvement of inflammatory eye manifestations was evident, together with a resolution of the liver disease. After 2 months, the dose of prednisone was progressively tapered. The eye signs underwent a partial remission 5 months after corticosteroid therapy was started. (Table 1, July 2007).
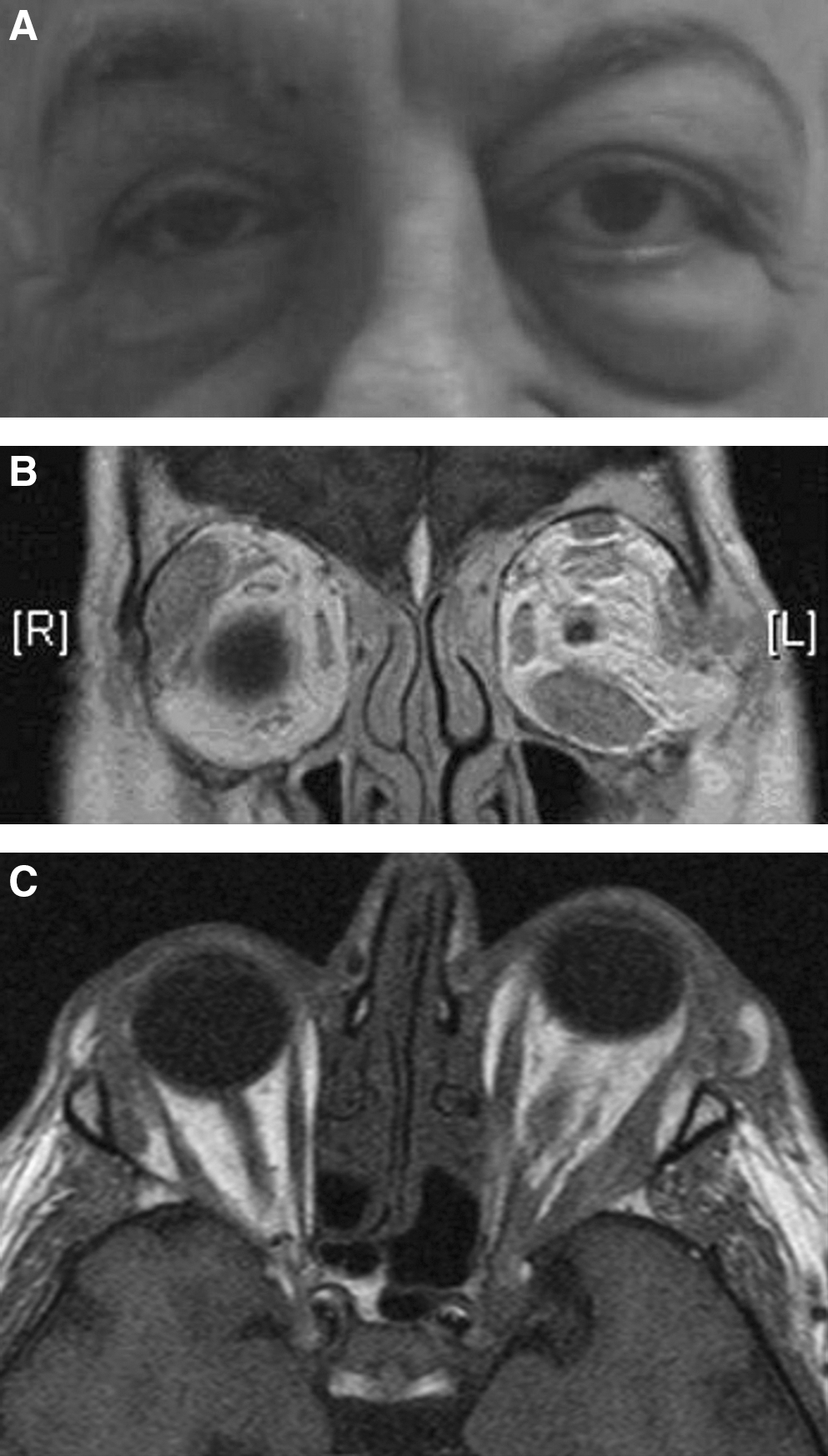
One year after starting corticosteroid therapy, when the patient was taking a low dose of the drug (prednisone 5 mg/day), he returned to our observation. A relapse of inflammatory orbitopathy was evident (Table 1, March 2008; Fig. 1A). On MRI of the orbit, a worsened picture was found (Fig. 1B, C). There were no cholestatic signs. Pulsed intravenous corticosteroid therapy was started, reaching a cumulative dose of 4g methylprednisolone. Orbital radiation with a cumulative dose of 20 Gy was also performed. A progressive amelioration of the eye signs and symptoms was observed. (Table 1, March 2009). Treatment with oral prednisone was continued for 5 months. At orbital MRI, reduction of the proptosis and shrinkage of enlarged extraocular muscles were evident. In the subsequent follow-up, the patient experienced two milder relapses of AIP. Orbitopathy did not recur after radiotheraphy.
Discussion
This report provides the first clinical description of severe Graves'-like orbitopathy occurring in association with AIP. In our patient, clinical features and MRI orbital imaging were consistent with a diagnosis of Graves' orbitopathy, including bilateral disease with a nonacute onset, multiple muscle enlargement without involvement of the tendon, increased orbital fat, forward displacement of the globe, lacrimal glands enlargement, absence of orbital masses, sinus involvement, and vascular engorgement (2). There was no clear evidence of autoimmune thyroid disease or dysfunction. Rather, the clinical course of this inflammatory orbitopathy was related to the course of AIP, as most of the relapses of the two diseases were coincident.
As discussed in a recent consensus guideline for the management of AIP (6), a variety of extrapancreatic complications are reported in this disease. In 2003, Kamisawa et al. (7) suggested that AIP is not simply a pancreatitis, but rather a pancreatic lesion within a syndrome termed IgG4–related systemic disease (ISD). ISD is a syndrome of multiorgan lymphoplasmacytic infiltration with fibrosis that often responds dramatically to corticosteroid therapy (8). Cholangitis, nephritis, Mikulicz disease, retroperitoneal fibrosis, pulmonary disease, hepatopathy, colitis, lymphoproliferative disease, and prostatitis are some of the typical manifestations of ISD. A subtype of autoimmune Hashimoto's thyroiditis, defined IgG4 thyroiditis, was also described, being characterized by a higher grade of parenchymal fibrosis, lymphoplasmacytic infiltration, and follicular cell degeneration, as compared with non-IgG4 thyroiditis (9). With specific regard to ocular involvement, orbital pseudolymphoma was reported in a few cases (10). Recently, Kubota et al. (11) reviewed the clinicopathological characteristics of 10 patients with infiltration of IgG4-positive plasma cells into the ocular adnexa. These patients showed swollen eyelids and/or proptosis; their ocular adnexal lesions consisted of different degrees of lymphoplasmacytic infiltration, reactive lymphoid follicles, and sclerosing lesions.
In our patient, the occurrence of a Graves'-like ophthalmopahty in association with AIP raises the question of which antigens might be involved in the autoimmune process and whether some of these antigens could be shared by the pancreas and the orbit. The autoantigens involved in the pathogenesis of AIP remain to be fully identified.
Two groups of autoantibodies have been described in the sera of patients with AIP: the non-pancreas-specific (antibodies reacting with carbonic anhydrase, with lactoferrin, and with alpha fodrin) and the pancreas-specific (autoantibodies directed to pancreatic secretory trypsin inhibitor, to trypsinogen PRRS 1 and 2, and to ubiquitin-protein ligase E3 component n-recognin 2-UBR2) ones (8). At least four isoforms of carbonic anhydrases (CA I, II, IV, and XIV) have been found in the human eye (12). Lactoferrin is present in tears and its expression is high in Graves' opthalmopathy (13). A recently described autoantibody of AIP is directed against a peptide that shows homology with an amino acid sequence of UBR2 (14). The gene codifying for UBR2 is not only expressed in the pancreas, but also in the eye, in the thyroid, and in muscles.
Fodrin is an intracellular cytoskeleton protein represented in eukaryotic cells (15,16). A fraction of this protein (120 KDa alpha fodrin) is a well known organ-specific autoantigen in Sjögren's syndrome (SS) (16). Patients with Graves' orbitopathy may show an involvement of the lacrimal gland by SS. Kahaly et al. reported the presence of autoantibodies reactive with alpha fodrin in sera of patients with Graves' orbitopathy (15). The presence of alpha fodrin and its expression in lacrimal and orbital target cells may explain the frequent involvement of the lacrimal gland in patients with Graves' orbitopathy (15). These data suggest that alpha fodrin may well be one of the autoantigens involved in cross-reacting autoimmunity between the pancreas and the orbit. Alpha fodrin and other autoantigens shared by the pancreas and the eye might be responsible for the unusual disorder observed in our patient.
Footnotes
Acknowledgment
We thank Dr. Riccardo Boeri for his technical support.
Disclosure Statement
The authors have no competing interests to disclose.