
Abstract
Background:
About 5% of nonmedullary thyroid cancers (NMTCs) are familial. Most patients with a family history of thyroid cancer do not meet the definition of familial NMTC (FNMTC; two or more affected family members). The aim of this study was to determine whether patients with a family history of NMTC, but who do not meet the definition of FNMTC, have more aggressive disease.
Methods:
A database of 1502 thyroidectomies was reviewed and 358 patients with NMTC who did not have a family history of benign thyroid disease and who underwent thyroidectomy from January 1994 to December 2008 were identified. These included 324 (90%) patients with papillary thyroid carcinoma (PTC), 24 (7%) with follicular thyroid cancer, and 10 (3%) with anaplastic or Hürthle cell carcinoma. Among them, those with and without a family history of NMTC in first-degree relatives were compared. Then patients with only one affected family member were compared with FNMTC patients.
Results:
Thirty-seven (10%) patients had a family history of thyroid cancer, all to of which had PTC. Patients with a family history of NMTC had a similar tumor size than those without (2±0 vs. 2.1±0 cm, p=0.72) but they were significantly younger (43±3 vs. 49±1 years, p=0.04), and more likely to have multicentricity (48% vs. 22%, p=0.01), malignant lymph nodes (22% vs. 11%, p=0.02), and local invasion to surrounding tissues (5.4% vs. 0.6%, p=0.007). They also had a higher recurrence rate (24% vs. 12%, p=0.03) than patients without a family history. Interestingly, patients with only one affected family member were similar to FNMTC patients with respect to age (44±4 vs. 40±3 years, p=0.4), tumor size (2±0 vs. 1.9±0 cm, p=0.65), rate of multicentricity (44% vs. 52%, p=0.57), malignant lymph nodes (22% vs. 21%, p=0.93), local invasiveness (5.5% vs. 11%, p=0.59), and disease recurrence (28% vs. 21%, p=0.56).
Conclusion:
Patients with NMTC having a family history of thyroid cancer have more aggressive disease, regardless of whether they meet the current definition of FNMTC regarding number of affected family members. Therefore, any positive family history should be considered a risk factor for more aggressive thyroid carcinoma.
Introduction
Robinson and Orr first reported a case of familial PTC in 1955 in 24-year-old identical twins (8). Population studies since then have shown that the risk of thyroid cancer increases ninefold in patients with a first-degree relative with thyroid cancer (9,10). A familial case of NMTC (FNMTC) is defined as a patient with two or more first-degree relatives diagnosed with thyroid cancer of follicular cell origin without another familial syndrome (3). When there are two people in a family with NMTC, there is a 31%–58% risk that the patient displays a familial syndrome. The risk of NMTC increases to >95% when there are three or more affected family members (10). However, given the stringent definition of FNMTC, most patients with a positive family history of thyroid cancer do not meet the definition.
Evidence suggests that FNMTC behaves in an autosomal dominant manner with incomplete penetrance and variable expressivity (6,11 –13). Several linkage studies have mapped out various chromosomal regions that may contain FNMTC susceptibility genes. These include TCO1, MNG1, fPTC/PRN or PRN1, and NMTC1 (14 –18). However, the responsible gene is yet to be identified. In the absence of a genetic marker, FNMTC cannot be easily differentiated from sporadic NMTC and families cannot be screened for a genetic condition.
Previous studies have shown that FNMTC is more aggressive than sporadic NMTC with an increased risk of recurrence, local invasion, multicentricity, and lymph node metastases (5). The aim of this study was to determine whether a positive family history is associated with more advanced disease and to determine what impact the extent of family history had on the aggressiveness of disease.
Materials and Methods
We conducted a retrospective review of 1502 patients who underwent a thyroidectomy between January 1994 and December 2008. Data were obtained from a prospectively maintained endocrine surgery database at the University of Wisconsin. Of the entire cohort, we identified 422 patients who underwent thyroidectomy for NMTC. We defined NMTC as any thyroid malignancy of follicular cell origin, which included papillary, follicular, Hürthle cell, or anaplastic carcinoma. A family history was obtained from all the patients and a family history was considered positive when patients had at least one first-degree relative with NMTC. These data were recorded in the database prospectively. When a family history was apparent and the affected family member had undergone thyroid surgery, the tumor histology was reinvestigated from the histologic records whenever possible. Family history and medical information (demographics, radiation exposure, additional cancer syndromes: familial adenomatous polyopsis) were confirmed by a careful review of the electronic health records and by reviewing endocrinology and endocrine surgery clinic notes. The presence of a positive or negative family history was documented, as was the number of affected family members.
We excluded patients with a family history of benign thyroid disease (multinodular goiter, follicular adenoma, Grave's disease, and Hashimoto's thyroiditis) and compared only those with a positive family history of NMTC to those without a positive family history of NMTC or benign thyroid disease. Patients with a family history of benign thyroid disease may or may not carry the genetic mutation seen in patients with FNMTC. Therefore, these patients were excluded from this study to ensure the cleanest comparison. Patients were then divided into two groups based upon their family history (Fig. 1).
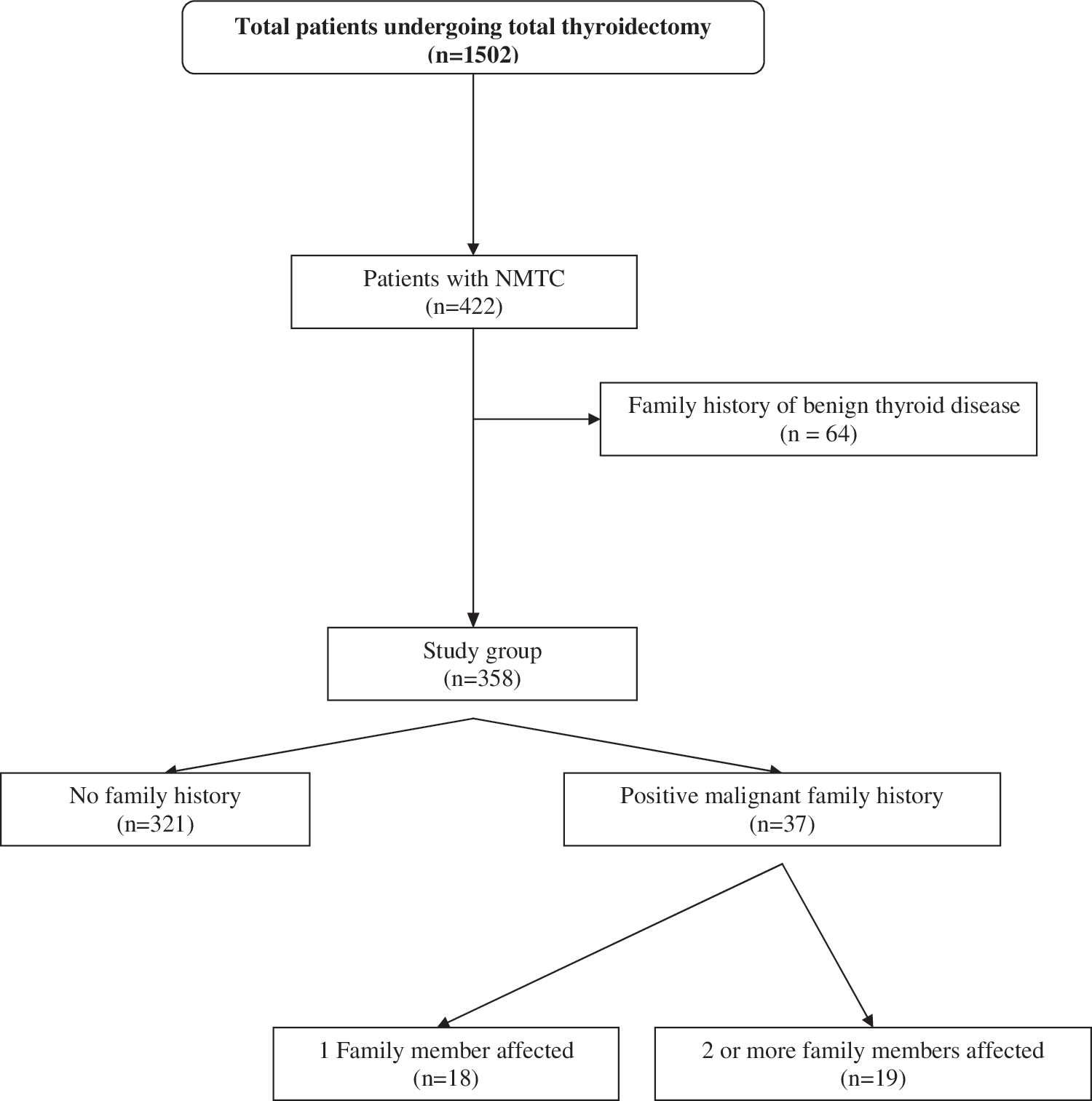
Study flow chart. NMTC, nonmedullary thyroid cancer.
We assessed baseline characteristics within our patient population in an attempt to determine whether a positive family history of NMTC was the key factor in predicting disease aggressiveness. Mean values of age at onset, nodule size, weight of thyroid gland, and the most recent thyroglobulin levels were obtained from probands with a positive family history of NMTC and analyzed against those without a family history.
We defined a positive family history as one or more first-degree relatives affected with NMTC. Aggressive features of the disease such as multicentricity, local invasion, positive lymph node metastasis, and disease recurrence were compared to those with no affected family members. We defined recurrence based on the need for reoperation or a positive whole-body scan showing metastatic disease.
Since many NMTC patients with a family history do not meet the definition of FNMTC (two or more affected first-degree relatives), we also performed a subset analysis to determine the aggressiveness of thyroid cancer in patients with just one affected family member versus those with two or more affected family members (who met the definition of FNMTC).
We performed all statistical analyses using SSPS (version 17). Comparison between the two groups was performed using the unpaired t-test and Chi-square. The difference between the two means was considered significant at a p<0.05.
Results
Of the entire cohort of 1502 thyroidectomies, 422 patients underwent surgery for NMTC. Patients with family history of benign thyroid disease were excluded (n=64). Study participants (n=358) included 321 (90%) patients without a family history of NMTC and 37 (10%) patients with a positive family history of NMTC (Fig. 1). Most of the patients had surgery for papillary thyroid cancer (n=324, 90%), but 7% had follicular thyroid cancer and 3% had anaplastic or Hürthle cell carcinoma. All patients with a positive family history of thyroid cancer were identified to have PTC on final pathology and all of their affected family members also had PTC. Of those with a positive family history, 49% (18/37) had only one affected family member, 27% (10/37) had two affected family members, and 24% (9/37) had three or more affected family members.
After comparing baseline characteristics between our positive family history and no family history cohorts, we found no significant difference in gender, nodule size, gland weight, or the most recent thyroglobulin levels (Table 1). However, compared with the patients with sporadic disease, patients with any positive family history were younger and more likely to demonstrate multicentricity (48% vs. 22%, p=0.01), malignant lymph nodes (22% vs. 11%, p=0.02), local invasion to surrounding tissues (5% vs. 0.6%, p=0.007), and disease recurrence (24% vs. 12%, p=0.03; Table 1).
FH, family history; Tg, thyroglobulin.
In the group with a positive family history, subset analysis revealed no significant difference between patients with only one affected first-degree relative versus those with two or more affected first-degree relatives (Table 2). Specifically, the comparison revealed similarly higher rates of multicentricity (44% vs. 52%, p=0.57), malignant lymph nodes (22% vs. 21%, p=0.93), local invasion to surrounding tissues (5.5% vs. 11%, p=0.59), and disease recurrence (28% vs. 21%, p=0.56) in those with only one affected family member versus those with two or more affected family members.
Discussion
Our analysis shows that FNMTC, namely PTC, is more aggressive than sporadic NMTC as portrayed by younger age at presentation and increased multicentricity, lymph node involvement, distant metastases, and recurrence. The presence of a positive family history was a significant predictor of aggressiveness. Interestingly, we found that the more aggressive pattern was seen not only in those patients who currently meet the definition of FNMTC (two or more affected family members) but also in those patients with only one affected family member. This suggests that implementation of the current definition of FNMTC may omit a significant number of patients with familial disease.
Most authors agree that FNMTC behaves more aggressively when compared with sporadic NMTC (19 –22) although not all (4,23). Ito et al. found the recurrence of thyroid cancer to be significant (p=0.04) in their FNMTC patients as well as a dramatically increased occurrence of multicentricity, yet lymph node metastases and invasion to surrounding tissues were not significant between sporadic and FNMTC patients (23). In the Ito study, 7% of FNMTC patients reported three or more affected family members, whereas our cohort consisted of 24% (9/37) FNMTC patients among the same category. This is a large difference in patient background and may account for the discrepancy between results especially since the risk for FNMTC increases to >95% when patients present with three or more affected members (10).
While FNMTC kindreds can include patients with follicular thyroid cancer or other follicular-derived malignancies, all patients with a positive family history in this study had PTC; therefore, our results reflect best on patients with a positive family history of PTC only.
The conflicting results in the literature maybe due to the inclusion of patients with a family history of two or less affected relatives into analyses, diluting the degree of aggressiveness (10,19). However, our study showed that patients with only one affected family member had a similar degree of aggressiveness as those who met the definition for FNMTC. A possible explanation for this finding is that these are really not two different groups. Triponez and colleagues showed that survival was significantly shorter in index cases who were diagnosed before the familial predisposition was recognized (22). Many of the patients with only one affected family member probably do have familial disease, but it may have not yet been recognized as such. In a similar regard, we also chose to eliminate patients with a family history of benign thyroid disease from our study. Most of the kindreds of FNMTC also have a high prevalence of benign nodular disease (18). Therefore, some patients with a family history of only benign thyroid disease may actually have the unrecognized putative genetic mutation(s) associated with FNMTC. Thus, it would be impossible to know whether to appropriately allocate these patients to the positive family history group or to the no family history group. Therefore, to have the cleanest comparison we excluded patients with a family history of benign thyroid disease.
It is not clearly understood why patients with a positive family history behave more aggressively. An inherited predisposition is assumed, supported by reports of vertical transmission in consecutive generations, horizontal transmission to siblings, an increased percentage of males with FNMTC compared with sporadic NMTC, and preponderance of multicentric and recurrent tumors (4,5,21,24,25). Cappezone et al. demonstrated that FNMTC exhibits “clinical anticipation,” with the second generation acquiring the disease at an earlier age and more advanced disease at presentation, also supporting genetic susceptibility (20). Other possible mechanisms explaining the familial association include an unidentified environmental factor or ascertainment bias—family members of a patient with NMTC maybe evaluated for thyroid disease more frequently than controls (12). Environmental exposure to low-dose radiation may also promote cancer development in thyroid glands that are already genetically predisposed to malignancy (26,27).
Linkage analyses and other genetic studies have had difficulty in identifying a genetic marker for FNMTC. A possible explanation is that FNMTC is not caused by a single gene, but is rather a heterogenous inherited syndrome with more than one susceptibility gene (12,28). Pal et al. showed that FNMTC patients were also at risk of developing other cancers (breast, kidney, colon, bladder, melanoma, and lymphoma), suggesting that these susceptibility genes may predispose to other cancers (6). Finding genes involved in FNMTC may provide information about other cancers as well (25,29).
It has been recommended that patients with FNMTC undergo more aggressive therapy with a total thyroidectomy, prophylactic central neck dissection, followed by postoperative radioactive iodine therapy (RAI) regardless of tumor size and lifelong thyroid suppression to reduce disease recurrence (5). A therapeutic lateral neck dissection should be performed if positive lymph nodes are identified. RAI remnant ablation and prophylactic central neck dissection are hotly debated areas in the treatment of thyroid cancer. We would ideally like to better identify patients with more aggressive disease up front who maybe more likely to benefit from these interventions. Since we currently have no means to genetically screen at-risk family members, neck ultrasound can play an important role in early recognition.
A positive family history should not be the only factor for using more aggressive therapy but it may tip the scales if the patient already presents with other high-risk features (presentation at young age, male gender, and lymph node metastasis). These patients should be thoroughly evaluated with an ultrasound and fine-needle aspiration of thyroid nodules. A negative fine needle aspiration (FNA) should not automatically exclude patients from surgery, since FNA is not as reliable in FNMTC due to the increased rate of multifocality, bilaterality, and multiple benign nodules seen in FNMTC patients (28,30,31). Musholt et al. proposed that the presence of multinodular goiter itself in at least three first- or second-degree relatives represents a primary criterion for FNMTC (32).
To some the results of this study may seem counter intuitive. As patients with a positive family history of thyroid cancer might be evaluated more frequently, or even potentially screened for their disease, it would be expected that their disease would be diagnosed at an earlier stage. This potential bias should only lessen the differences between our groups, suggesting that the true difference in aggressiveness maybe even greater than we have found.
We do not think that the definition of FNMTC should be changed, but we must acknowledge that the definition is so stringent that it may not capture all of the FNMTC patients. Modifying the definition may result in a dilution effect whereby patients with sporadic disease are erroneously included among the true FNMTC patients. Nevertheless, it is possible that bona fide FNMTC patients may only have one family member diagnosed at the time of presentation. Therefore, in the absence of a genetic marker, we think that any family history of thyroid cancer should be considered significant.
Conclusion
FNMTC is a separate clinical entity that warrants aggressive therapy due to its increased multicentricity, lymph node metastasis, local invasion, and frequent recurrence. We anticipate that characterizing the responsible gene(s) will clear the ambiguity surrounding FNMTC diagnosis and provide insights for optimal therapeutic approaches. Until genetic testing can clearly identify those with familial disease, we recommend a scrupulous evaluation of family history in order to identify NMTC patients with a positive family history. This information can then be used to identify patients who may have more aggressive disease, are at higher risk for recurrence, and therefore, may benefit from more aggressive initial treatment.
Footnotes
Acknowledgment
The authors have no acknowledgements to disclose.
Disclosure Statement
The authors declare that no competing financial interests exist.