
Abstract
Background:
There is a growing belief that a pretherapy scan yields little or no additional information that would impact on radioiodine ablation dosing. In addition, there is some concern regarding on the stunning effect of a pretherapy scan, especially when I-131 radioisotope is used for imaging. We hypothesized that a pretherapy scan provides invaluable information on the amount of thyroid remnant, sometimes indicating the need for two-step I-131 ablation. It may also detect unsuspected local lymph node involvement or distant metastases, indicating the requirement for a higher I-131 dose after thyroidectomy. The aim of this study was to evaluate how effective pretherapy scans are for guiding I-131 therapy planning and augmenting information provided in the pathology reports for thyroidectomy specimens.
Methods:
We reviewed 122 patients who underwent I-123 pretherapy scan and I-131 radioablation at Yale New Haven Hospital between January 2006 and August 2007. The percentage of neck uptake and whole-body images were acquired 24 hours following the administration of 51.8 MBq (1.4 mCi) of I-123 NaI. A 24-hour uptake of >3% was used as the cutoff to determine whether there was a greater than desired quantity of thyroid remnant, which would require a two-step treatment protocol. Furthermore, attention was paid to identifying cervical lymph nodes, which may not have presented themselves in the euthyroid state at the time of thyroidectomy. Additional clinical information provided by pretherapy scans was computed as percentages with 95% confidence intervals by using adjusted Wald intervals.
Results:
Overall, the pretherapy scans provided additional critical information in 25% of the cases (31/122; 95% CI: 18%–34%). For cases demonstrating >3% uptake with midline lymph nodes, the pretherapy scan provided additional information in 50% of the cases (8/16; 95% CI: 28%–72%).
Conclusions:
Our study demonstrated that I-123 pretherapy scans provide valuable information with regard to unsuspected lymph nodes or distant metastases, indicating the requirement for a significantly higher I-131 dose, and unexpected large thyroid remnants, suggesting the need for two-step ablation. We should take advantage of stimulated pretherapy scans and adjust the treatment dosing accordingly.
Introduction
There is a growing belief that a postoperative pre-ablation diagnostic scan or pretherapy scan yields little or no additional information that would affect radioiodine ablation dosing for patients with DTC (3,4). Due to the cost of the scan and a slightly prolonged hypothyroid period, pretherapy scans have fallen out of favor at many institutions. Some endocrinologists have questioned the usefulness of a pretherapy scan, because they believe it rarely changes the decision for the therapy (5). In addition, there is some concern about the stunning effect of a pretherapy scan, especially when I-131 radioiodine is used (6 –9). “Stunning” arises from administration of a diagnostic dose of I-131 or I-123 that may reduce the uptake of a subsequent therapeutic dose of I-131 and may potentially decrease the efficacy of the ablation dose. The American Thyroid Association recommends using a low-dose I-131 (1–3 mCi) or I-123 when the extent of the thyroid remnant cannot be accurately ascertained from the surgical report or neck ultrasonography or when the results would alter either the decision to treat or help in determining an appropriate dose to be administered (1,2). The Guidelines from European Association of Nuclear Medicine recommend avoiding pretherapeutic I-131 diagnostic scan or thyroid bed uptake for avoidance of stunning in cases in which radioiodine ablation therapy has been determined to be necessary (4).
At Yale New Haven Hospital (YNHH), we routinely perform an I-123 pretherapy scan on patients with thyroid cancer who have received total thyroidectomy with or without lymph node dissection. We believe the pretherapy scan provides useful information for determining 1) large thyroid remnants that may require a two-step ablation, and 2) unsuspected lymph nodes or distant metastases, which require a significantly higher dose.
The aim of this study was to determine whether a pretherapy scan has additional merit from clinical information guided by the pathology report alone in determining the radioablative dose. We sought to assess the extent of grossly apparent stunning by comparing I-123 pretherapy and I-131 posttherapy scans.
Methods
We retrospectively reviewed 150 consecutive patients who underwent I-131 radioiodine ablation at YNHH between January 2006 and August 2007 (see Table 1). Patients had total thyroidectomy either at YNHH or at outside hospitals. Exclusion criteria included incomplete thyroidectomy (two-step thyroidectomy, for instance, hemithyroidectomy followed by completion thyroidectomy) or substitution of I-131 for I-123 in pretherapy scans, Thyrogen® (Genzyme Corporation, Cambridge, MA) stimulation I-131 therapy without a pretherapy scan, and re-treatment for recurrence. A total of 122 patients were included in the final analysis. The retrospective study was approved by Yale University Human Investigation Committee.
The percentage of neck uptake and whole body images were acquired 24 hours following the administration of 51.8 MBq (1.4 mCi) of I-123 sodium iodine (NaI). The patients were imaged in a supine position using a Philips SKYLight dual-headed gamma camera (Philips) with 3/8-inch-thick NaI crystal and low-energy high-resolution collimator and 20% energy window centered at 159 keV. Anterior and posterior whole-body planar images as well as spot views in the neck region with I-123 (200 μCi) markers placed at the chin and sternal notch were obtained (see Fig. 1). Additional lateral projections were acquired as needed. We used I-123 NaI for all pretherapy uptakes and scans to have better image quality, reduce radiation exposure, and reduce the possibility of stunning of radioiodine naïve thyroid tissues, which could be assessed using the posttherapy scan.
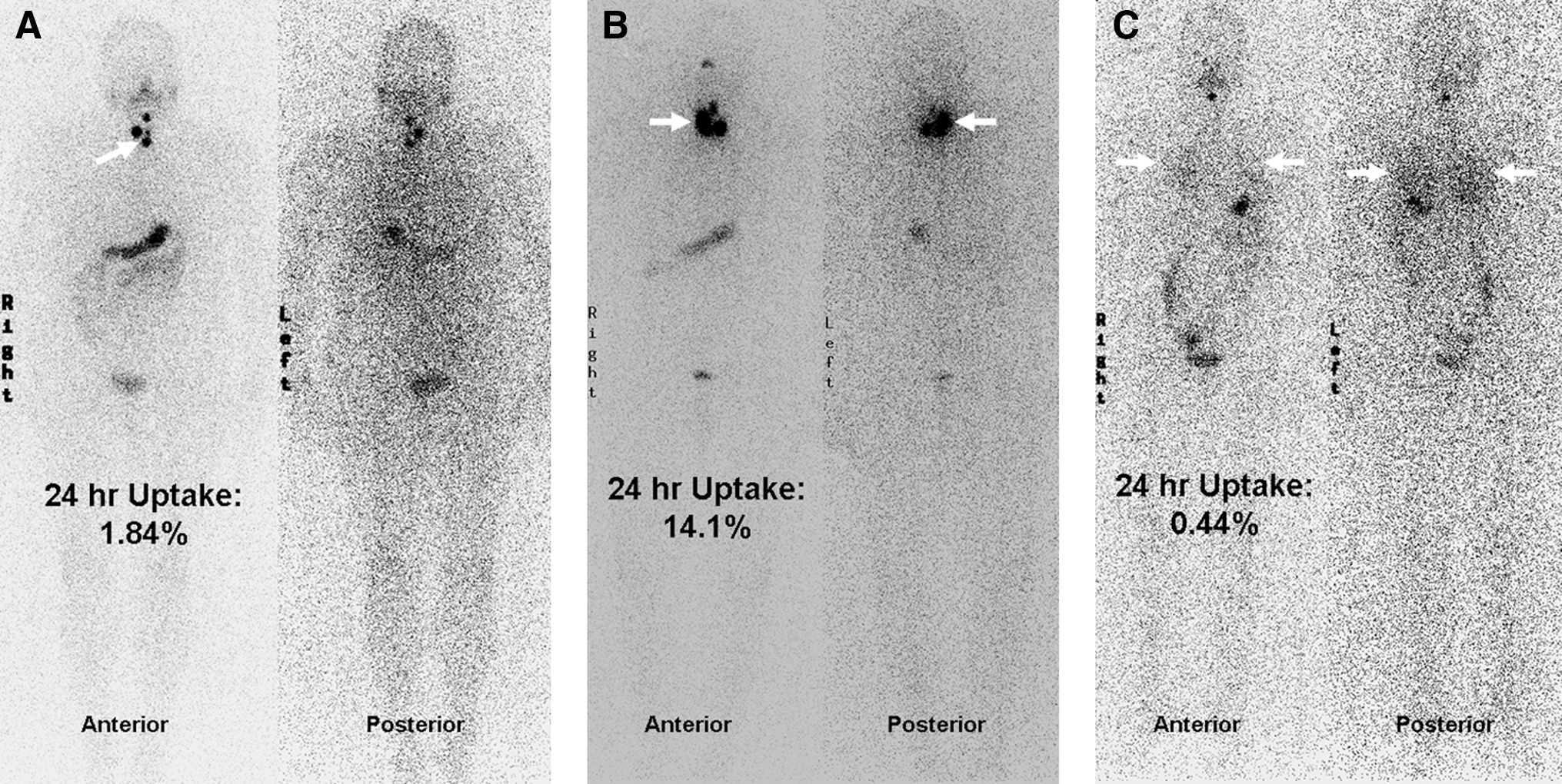
Examples of anterior and posterior projections of I-123 whole-body scan in thyroid cancer patients.
I-131 posttherapy scans were obtained between 7 and 10 days after treatment in order to optimize the target to background ratio. Patients were imaged in a supine position using a Philips SKYLight dual-headed gamma camera (Philips) with 5/8-inch-thick NaI crystal and high-energy collimator and 20% energy window centered at 364 keV. Anterior and posterior whole-body planar images as well as spot views of the neck region with I-131 markers placed at the chin and sternal notch were obtained. Additional lateral projections were acquired as needed. Stunning effects from I-123 were assessed by comparing the I-131 posttherapy to I-123 pretherapy scan. Additional uptake or quantification was not performed.
Two board-certified nuclear medicine physicians at YNHH independently reviewed all of the pretherapy scans and determined the location of the uptake. Furthermore, attention was paid to identify cervical lymph nodes, which may not have presented themselves in the euthyroid state at the time of thyroidectomy. The pretherapy images and reports were obtained from a Fuji Synapse system. The readers classified the I-123 uptake to 1) within the thyroid bed only, 2) outside the thyroid bed but within the neck, and 3) outside of the neck. The thyroid bed only was defined as uptake noted only in the lower part of the neck and extending laterally on either side of the midline. If the two readers disagreed on the interpretation of a scan, the final decision was made after they discussed it (20/122 patients). Physicians further characterized the location of uptake outside of the thyroid bed but within the neck. For instance, if the uptake was in the midline (between the chin and sternal notch markers), was more intense than usual, and could not be explained by thyroglossal duct remnant, then this uptake was considered to possibly be in the lymph node. However, if the uptake was not in the midline then it was considered to be in the lymph node but it was less certain than those at midline. The readers had no disagreements in this portion of the evaluation.
The percentage of thyroid uptake in the neck was obtained. This was measured by subtracting the background activity measured at the thigh from the total counts in the neck and then dividing the result by the counts from an I-123 standard in a neck phantom with decay correction. The percent uptake was calculated by the following formula:
A 24-hour uptake of >3% was used as the cutoff combined with biodistribution information from imaging to determine whether there was a greater than desired quantity of thyroid remnant, which would require a two-step treatment protocol. For instance, if the uptake in the thyroid remnant was greater than the presumed lymph node uptake, the patient might be treated with a low dose of I-131 first (<1.11 GBq) to ablate a significant amount of thyroid remnants followed by a higher dose (>3.70 GBq) within 3–6 months to cover the relatively less iodine avid lymph nodes or pathologic lesions. If the uptake in the presume lymph nodes was greater than in thyroid remnants, then a single high dose of I-131 (>3.70 GBq) would be administered.
The pathology reports of the YNHH patients were accessed via the Centricity/Logician system. The pathology reports of the outside patients were obtained through the referring endocrinologists' offices. We reviewed all pathology reports, including type of thyroid cancer, whether lymph nodes were sampled or neck dissection was performed, and whether there were other suspicious findings.
We compared the patients who had total thyroidectomy in the medical community against those at YNHH in terms of the size of thyroid remnants, which was assumed to be proportional to the measured neck uptake. The YNHH and outside patients were each categorized by the uptake in the neck using the conservative mark of 3% uptake and by visual location of the uptake within the neck, which was compared to the presence of metastatic lymph nodes on pathology reports.
Additional critical clinical information provided by I-123 pretherapy scan was computed as a percentage with 95% confidence intervals using adjusted Wald intervals (10,11).
Results
Overall, the pretherapy scan provided additional information in 25% of the cases (31/122; 95% CI 18%–34%) when compared with pathology reports only. For YNHH surgeries, the pretherapy scan provided additional critical clinical information in 23% of the cases (21/92; 95% CI 15%–32%); for surgeries outside YNHH, the pretherapy scan provided additional clinical information for up to 33% of the cases (10/30; 95% CI 19%–51%).
We further divided the subjects using 3% neck uptake as the cutoff for determining if the thyroid remnant was significant. Of the 32 patients with uptake ≥3%, only seven patients required a two-step radioiodine ablation. For YNHH patients, 3 out of 19 patients required a two-step treatment due to significant amount of thyroid remnants, while 16 patients received only a single high dose for treatment of local nodal metastases. For outside patients, 4 out of 13 patients required a two-step treatment for significant remnants, while nine patients received a single high dose for treatment of nodal metastases.
For cases with uptake ≥3% with iodine avid foci at the midline, the pretherapy scan provided additional clinical information up to 50% of the cases in differentiation between suspected lymph nodes and remnants (8/16; 95% CI 28%–72%). For cases with ≥3% uptake but iodine foci not at the midline, the pretherapy scan provided additional clinical information in 36% of the cases (5/14; 95% CI 16%–62%).
For cases with 24-hour neck uptake <3% and iodine avid foci at the midline, the pretherapy scan provided additional clinical information in 32% of the cases in differentiating between lymph nodes and remnants when compared with pathology reports only (14/44; 95% CI 20%–47%). For cases with uptake <3% but iodine avid foci not at the midline, the pretherapy scan provided additional clinical information in 19% of the cases (4/21; 95% CI 7%–41%). There was no grossly apparent stunning associated with the I-123 pretherapy scan based on a visual comparison of the I-131 posttherapy scan with the I-123 pretherapy scan.
Discussion
There has been a general belief in the endocrine and nuclear medicine societies that the postsurgery pre-ablation diagnostic thyroid scan has little or no impact on the I-131 ablation treatment for DTC. Part of the reason is that most physicians will routinely perform the posttreatment scan after the high dose of I-131 radioiodine ablation, which has been demonstrated to detect more lesions and to be more sensitive than the pretherapy diagnostic scan (12 –14). For this reason, some insurance companies do not reimburse the pretherapy diagnostic scan, which limits this option. There are two major drawbacks to not performing the pretherapy diagnostic scan. First, we will not have information regarding the amount of thyroid remnant, which is highly dependent on the skill of the surgeon. If there is a large amount of thyroid remnant with a high percentage of uptake (see Fig. 1B), it may compromise the biodistribution of I-131 to metastatic lymph nodes, which are less iodine avid. On the other hand, administering a high dose of I-131 (>3.7 GBq or 100 mCi) to the large remnants may be overkill and may potentially cause undesirable complications, such as radiation-induced thyroiditis (15,16). With the help of a pretherapy scan, we can identify patients with large remnants and recommend a two-step treatment, using a low dose (<1.11 GB) for remnant ablation followed by a high dose (>3.7 GB) for local or distant metastases. Some authors proposed using a pretherapy uptake measurement with only a very low dose of I-131 to determine the amount of thyroid remnants (3,17,18). Unfortunately the degree of I-131 uptake will not be likely to distinguish between thyroid remnants and local nodal metastases. In contrast, pretherapy images can identify local nodal or distal metastases (see Fig. 1C), which may not declare themselves while patients are euthyroid, either before or after thyroid surgery. Pretherapy ultrasound may be useful to determine remnant size or cervical nodal metastases, but it does not provide critical information for distant metastases. Even a routine chest X ray will miss almost half of the early lung metastases (19). A single pretherapy scan will provide invaluable information for localization of disease, which will complement the finding of a high serum Tg level. We have been surprised, in a small number of patients, by finding unsuspected metastases in the mediastinum, lungs, or skeleton. Hence, a pretherapy scan is essential to have the information required to prescribe an appropriate dose of I-131 for effective treatment.
It is noteworthy that I-123 pretherapy scans were performed when patients were hypothyroid; their thyrotropin (TSH) level was documented to be elevated (>30 μIU/mL) several weeks after thyroid hormone withdrawal. The elevated TSH stimulates iodine uptake in the thyroid remnant or residual thyroid cancer. This increases the sensitivity of the scan compared with the euthyroid state at the time of surgery. In some cases pathologic lymph nodes will be hidden from inspection at the time of surgery but declare themselves in the scan.
Salvatori et al. (5) retrospectively reviewed 875 patients who underwent I-131 radioiodine treatment without a pretherapy scan and found that the majority of the patients (94%) had thyroid remnants or metastases on posttherapy scans. In most cases (91.2%), the neck uptake and Tg level were sufficient for the detection of remnants. Only 14 patients (1.6%) with tiny metastatic lymph nodes seen on posttherapy scans showed undetectable Tg level when hypothyroid and another 30 patients (3.6%) with faintly positive findings for thyroid remnants posttherapy were classified as false-positive results. Salvatori et al. (5) concluded that neck uptake and measuring serum Tg alone are sufficient for I-131 pretreatment evaluation and that it is reasonable to omit routine diagnostic whole-body scans, thereby obtaining clinical, managerial, and economic advantages. However, the authors indicated that 6% of the patients did not have thyroid remnants or metastases; therefore, they probably received unnecessary I-131 treatment. This could have been avoided if a pretherapy scan had been performed.
de Klerk et al. (20) did not do pretherapy scans and gave fixed high empiric ablative doses (3.7–7.4 GBq) in 93 patients, based on pathology and age. They concluded that high-dose radioiodine ablation without a diagnostic scan resulted in a high rate of successful one-time ablation in most cases. However, 19 cases (20.4%) had residual thyroid remnants or metastasis and required retreatment, with some patients receiving greater than necessary dosing. With the help of a pretherapy scan, we can perform two-step treatment for patients with large thyroid remnants or prescribe an appropriate dose for low-risk patients to avoid unnecessary empiric high dosing.
There have been several studies that compared I-123 with I-131 for pretherapy diagnostic whole-body scan, the consensus from these being that I-123 is superior to I-131 with regard to imaging quality, sensitivity, and internal radiation dosimetry, with considerably lower or no stunning interference in subsequent I-131 ablation therapy (21 –24). I-123 iodine is a pure gamma radiation emitter with a peak energy of 159 keV. This is ideal for imaging with modern gamma cameras using a low to medium energy collimator, with a six times greater detectable photon flux than I-131 based on equal administered radioactivity (21 –24). Because I-123 also has a shorter half-life (13 hours), the actual iodine mass required for I-123 is much less than that of I-131. In addition, the absence of beta emission from I-123 will have less interaction with tissues, and hence, will minimize any stunning effects (21 –24). We have not observed any stunning effect from our I-123 pretherapy scans at YNHH. Therefore, concerns of stunning remaining thyroid tissue should not be used to justify not obtaining an I-123 pretherapy scan. However, I-123 is more expensive than I-131 ($306 for 1.4 mCi of I-123 compared to $65 for 1–2 mCi of I-131 at YNHH).
Van Nostrand et al. (25) showed that information from I-123 pretherapy scans may have altered management of thyroid cancer patients in up to 53% of 355 patients included in their study as compared to likely management had the pretherapy scan not been done. They also argued that if they limited their analysis to five scenarios for which “most nuclear medicine physicians, nuclear radiologists, and/or endocrinologists would alter management” the information from I-123 pretherapy scans would have altered management of thyroid cancer in about 29% of the patients. This percentage is similar to the value of 25% obtained in our study.
Among patients with well-differentiated thyroid cancer, tumor biology is variable, including the tumor's degree of iodine avidity. Furthermore, variation of iodine biodistribution should impact the degree of treatment efficacy from a fixed dose and total radiation dosimetry requirements. In agreement with McDougall (26), we believe it is important to know in advance what we are treating in order to prescribe the most appropriate dose. By obtaining an I-123 pretherapy scan, we can document the extent and iodine avidity of thyroid remnants and tumors and the biodistribution and clearance of iodine at 24 hours and detect distant metastases that would otherwise be missed. We recognize, however, that the posttreatment I-131 scan may provide additional information compared to the pretherapy scan.
If a pretherapy I-123 scan (or a pretherapy I-131 scan) is not obtained and the results of the I-131 therapy scan indicate that the dose administered was likely too low, patients can be treated with a second dose of I-131 to eradicate residual disease or metastases. We argue, however, that this inconveniences patients in terms of the additional home preparation required and is expensive for patients in terms of lost work time related to radiation safety concerns. It may also be associated with poor quality of life related to hypothyroidism if thyroid hormone withdrawal is used to prepare the patient for I-131 treatment, and it imposes emotional stress related, among other things, to isolation from family and friends. Furthermore, concerns of tissue stunning from an unsuccessful therapy dose will be much greater than had a pretherapy scan been obtained with I-123.
Conclusion
Our study demonstrates that pretherapy scans provide additional valuable information that impacts I-131 radioiodine treatment dosing, with no observed evidence of stunning. We believe that I-123 pretherapy scans should be performed routinely in order to prescribe the most appropriate dose of I-131 according the best outcome for definitive treatment.
Footnotes
Author Disclosure Statement
No competing financial interests exist.