
Abstract
Background:
Interactions between CD40 and its ligand (CD40L) have important roles in T-cell-dependent activation of B cells, which may be related to the thyrotoxic activity of Graves' disease (GD). Soluble forms of CD40 ligand (sCD40L) are released from activated T cells and platelets, and several types of inflammatory cytokines are increased in patients with hyperthyroid GD. The aim of this study was to assess sCD40L and other cytokines as clinical indicators of disease activity or as possible markers of remission in GD.
Methods:
Serum levels of sCD40L, interleukin 18 (IL-18), tumor necrosis factor-alpha (TNFα), and TNFα receptors 1 and 2 (TNFR1 and TNFR2) were investigated in patients with active GD (GD-A), intractable GD (GD-IT), inactive GD (GD-IA), GD in remission (GD-R), and Hashimoto's thyroiditis (HT), and in control subjects (CON).
Results:
Serum concentrations of sCD40L were higher in the GD-A and GD-IT groups than in the HT and CON groups. Similarly, serum concentrations of IL-18, which induces Th1 cytokines, such as interferon-γ, were higher in the GD-A and GD-IT groups than in all other groups. Serum levels of TNFR1 and TNFR2 were also significantly higher in the GD-A than in all other groups. The mean serum concentration of TNFα was higher in the GD-R compared with the GD-A and GD-IT groups, although the difference was not significant. Serum sCD40L concentrations in the GD-R group were lower than in the GD-A and GD-IT groups. Finally, the ratio of serum TNFα to sCD40L was higher in the GD-R group than in the GD-A and GD-IT groups. This is the first report that serum sCD40L is increased in active GD, and that the serum TNFα:sCD40L ratio is a marker for remission in GD.
Conclusions:
Our results suggest that not only thyrotoxicosis, but also the activity of the immunoreaction presenting as anti-thyrotropin receptor antibodies (TRAb) titer in GD, affects inflammatory cytokine serum profiles. Serum profiles of cytokines vary in patients with GD depending on disease activity. An elevated serum TNFα:sCD40L ratio indicates declining disease activity and reflects a shift from Th2 to Th1 dominance, suggesting that suppression of sCD40L or increased production of TNFα is required to initiate or maintain remission of GD.
Introduction
T cells, especially helper T (Th) cells, play pivotal roles in the immune response. Th cells are commonly divided into three subtypes depending on their ability to produce specific cytokines (12). An imbalance of Th1 and Th2 responsiveness and, more recently, that of Th17 and Treg has been demonstrated in various autoimmune diseases (13). Type 1 diabetes and Hashimoto's thyroiditis (HT) represent Th1-dominant diseases (14), while GD is considered to show Th2 or Th0 dominance. The balance between Th17 and Treg has not been established to date in autoimmune thyroid diseases compared with normal subjects.
We have previously reported that CD8+ cells (cytotoxic T cells) are decreased in hyperthyroid GD, and increased after the patients were rendered euthyroid or hypothyroid by antithyroid therapy (15). We have investigated the roles of CD8+ T cells in the disease activity of GD. Our previous studies also suggested the possible involvement of CD8+ cells in abnormal B cell activation, with evidence of an increase of BCGFs (5), a decrease in CD8+ cell numbers (16), and an increase in IL-10 production (17) following activation of B cells via anti-CD40 antibody and IL-4 in peripheral blood cells from patients with GD. Finally, we reported that Th2 cells in GD were predominantly induced through B cell activation via a CD40 pathway, resulting in overproduction of IL-10, and CD8+ cells inhibited this series of responses (18).
We hypothesized that the activity of GD may be related to the balance between serum Th1 and Th2 profiles. Th2 dominance in GD may induce an increased production of sCD40L. Conversely, a shift from Th2 dominance to Th1/Th2 equilibrium may contribute to the remission of GD. Therefore, it is important to classify the clinical activity of GD based upon patient levels of pro-inflammatory cytokines. This study aimed to clarify the clinical significance of cytokines as a surrogate marker to detect disease activity and to predict remission in GD.
Methods
Subjects
Subjects were outpatients who visited our hospital for treatment for GD and HT. Data were collected from patients who agreed to participate in this study and whose serum TSH, free triiodothyronine (FT3), and free thyroxine (FT4) were measured as a part of a routine follow-up. Controls (the CON group) were 37 healthy subjects without any past or present history of thyroid disease, who agreed to participate in this study. Subjects were divided into 6 groups based on the activity of their disease: (i) 49 patients with thyrotoxic active GD (the GD-A group); (ii) 30 patients with intractable GD (the GD-IT group) who were euthyroid to mildly toxic while on an antithyroid regimen for more than 5 years; (iii) 35 euthyroid patients with inactive GD (the GD-IA group) who were taking an antithyroid regimen for less than 5 years; (iv) 29 euthyroid patients with GD in remission (the GD-R group) who were not taking medication; (v) 49 patients with HT (the HT group); and (vi) 37 healthy controls (the CON group) with no history of thyroid disease. The clinical manifestations of each group are shown in Table 1.
Subjects with GD were divided into four groups as described in the Methods section.
GD, Graves' disease; M/F, male/female; TSH, thyrotropin; FT3, free triiodothyronine; FT4, free thyroxine; TRAb (TBII), anti-TSH receptor antibodies (TSH binding inhibitor immunoglobulins).
The university hospital's ethics review committee approved this descriptive study, and informed written consent was obtained from each patient. No exclusion criteria other than unwillingness to participate in the study were applied in the selection of the CON group.
Routine serum chemistry was measured using a Hitachi 7600 automatic analyzer (Hitachi High Technologies, Tokyo, Japan). Serum TSH, FT3, and FT4 concentrations were examined by chemiluminescent enzyme immunoassay (Ortho-Clinical Diagnostics, Raritan, NJ). Serum anti-TSH receptor antibodies (TRAb), anti-TPO antibodies, and anti-Tg antibodies were examined by radioimmunoassay (Cosmic Corporation, Tokyo, Japan). IL-18 concentrations were examined by ELISA (Medical & Biological Laboratories Co. Ltd., Nagoya, Japan). TNFα concentrations were examined by ELISA (Immunotech SAS, Marseille, France). The concentrations of soluble forms of CD40L (sCD40L) and TNFα receptors 1 and 2 (sTNFR1 and sTNFR2) were examined by ELISA (R&D Systems, Minneapolis, MN). The interassay variations for these cytokines were <6.4%, <8.6%, <0.6%, <6.8%, and <7.4%, respectively. The intra-assay variations were <3%, <7.3%, <5.1%, <9.1%, and <2.5%, respectively.
Statistical analysis
Results are expressed as mean±standard deviation. A two-sided unpaired Student's t-test or analysis of variance for multiple comparisons was used for statistical analysis. A difference between experimental groups was considered to be significant when the P value was <5%.
Results
The serum levels of IL-18, sCD40L, and other cytokines were investigated in the GD-A, GD-IT, GD-IA, GD-R, HT, and CON groups (Table 1). The serum concentration of IL-18, which induces Th1 cytokines, such as interferon-γ (IFN-γ), was higher in the GD-A and GD-IT groups than in other groups (Fig. 1), while the serum concentration of sCD40L, which contributes to B lymphocyte activation, was higher in the GD-A and GD-IT groups than in the HT and CON groups (Fig. 2). Serum levels of both TNFR1 and TNFR2 were significantly higher in the GD-A group than in all other groups (Fig. 3A, B). The correlation between each cytokine level and various thyroid parameters in GD is shown in Table 2. The values of IL-18, sTNFR1, or sTNFR2 were correlated with FT3 or TRAb, although such correlations were not found between these cytokines and TSH, TPOAb, or TgAb (Table 2). The mean serum concentration of TNFα in the GD-R group was higher than in the GD-A and GD-IT groups, although the difference was not statistically significant (Fig. 4). On the other hand, the mean concentration of sCD40L in the GD-R group was lower than that in the GD-A and GD-IT groups. When these results were combined, the ratio of serum TNFα to sCD40L was higher in the GD-R group than in the GD-A and GD-IT groups (Fig. 5). The serial changes of the TNFα:sCD40L ratio in the GD-IT and GD-R groups were investigated in several cases as shown in Figure 6. The increase rate of the ratio in the GD-R group was 46.2%, while the decrease rate of the ratio in the GD-IT groups was 22.2%, although it was not statistically significant. Further follow-up studies are required to clarify the clinical significance of this ratio.
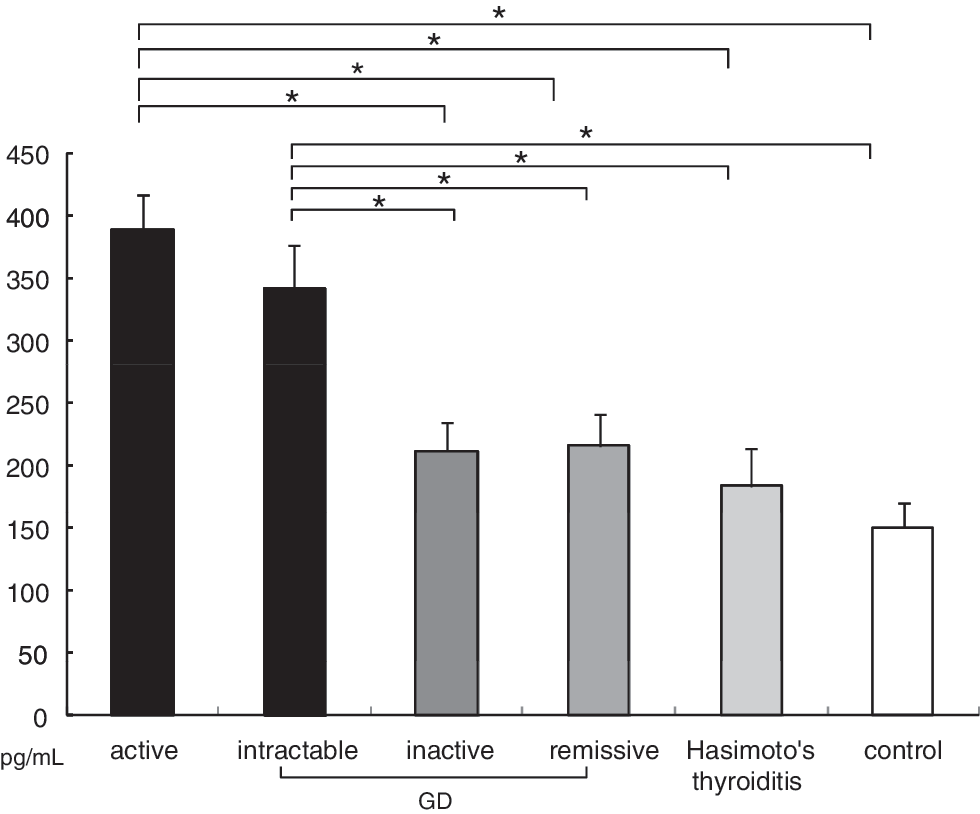
Concentrations of serum interleukin-18 (IL-18) among subjects with Graves' disease (GD), Hashimoto's thyroiditis (HT), and controls. Each value represents mean±standard deviation (SD); *p<0.05. Statistical analysis was done with analysis of variance (ANOVA) and Fisher's test.
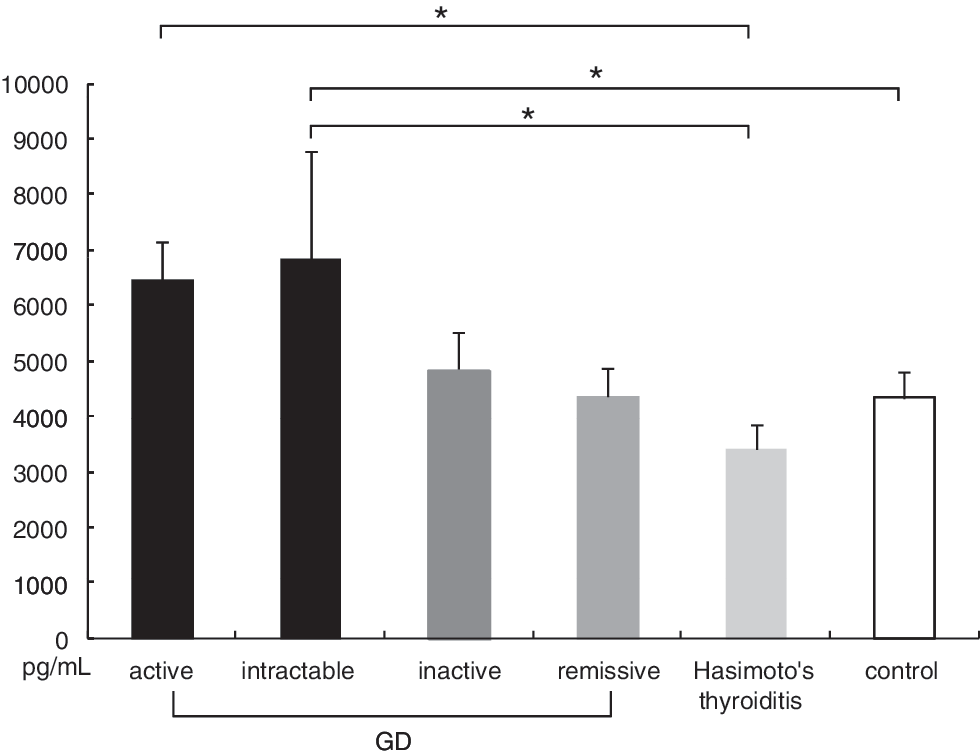
Concentrations of serum CD40L (soluble forms of CD40 ligand [sCD40L]) among subjects with GD, HT, and controls. Each value represents mean±SD; *p<0.05. Statistical analysis was done with ANOVA and Fisher's test.
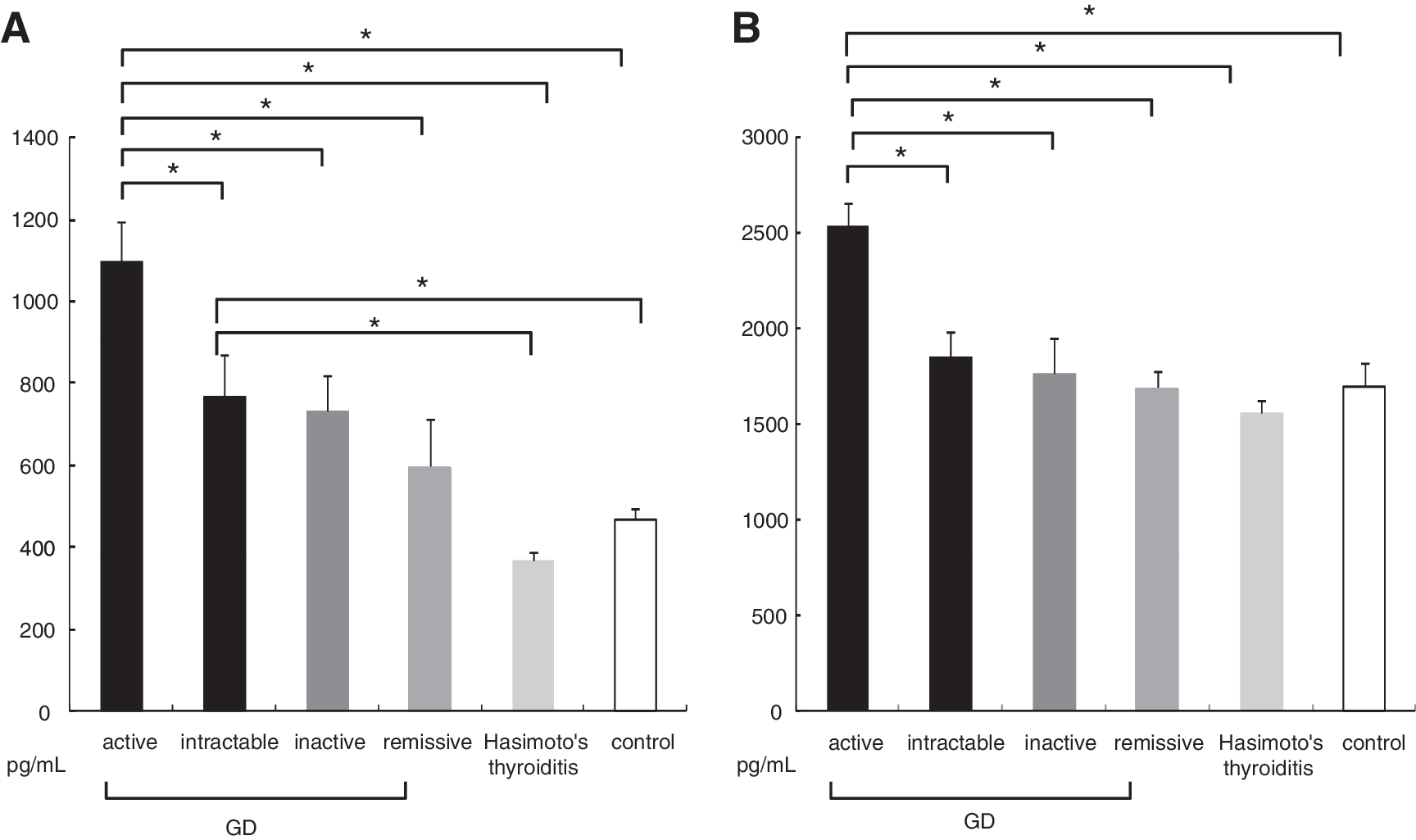
Concentrations of serum tumor necrosis factor-alpha (TNFα) receptors 1
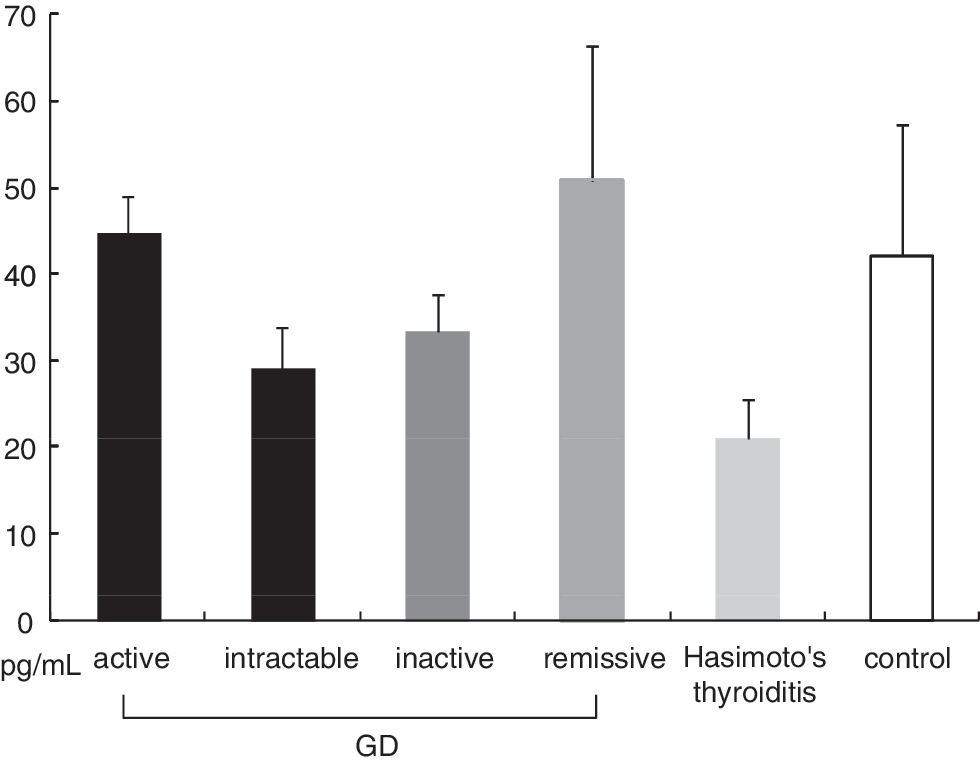
Concentrations of TNFα among subjects with GD. Each value represents mean±SD. Statistical analysis was done with ANOVA and Fisher's test.
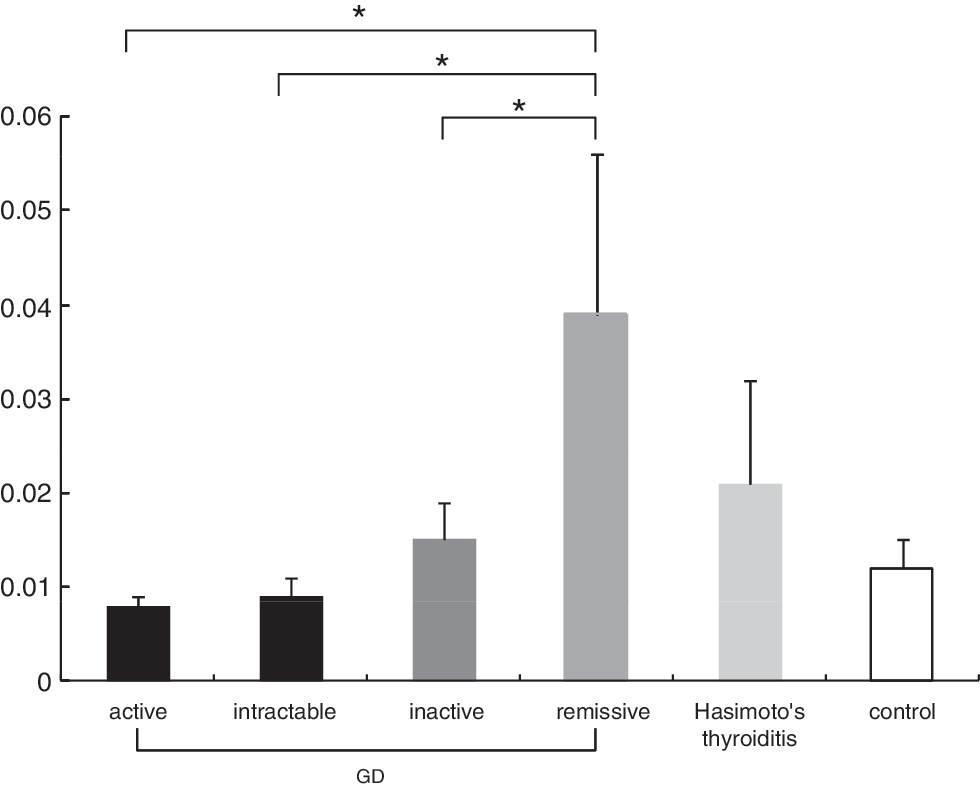
Concentrations of TNFα:sCD40L ratio among subjects with GD, HT, and controls. Each value represents mean±SD; *p<0.05, compared with the value of active GD. Statistical analysis was done with ANOVA and Fisher's test.
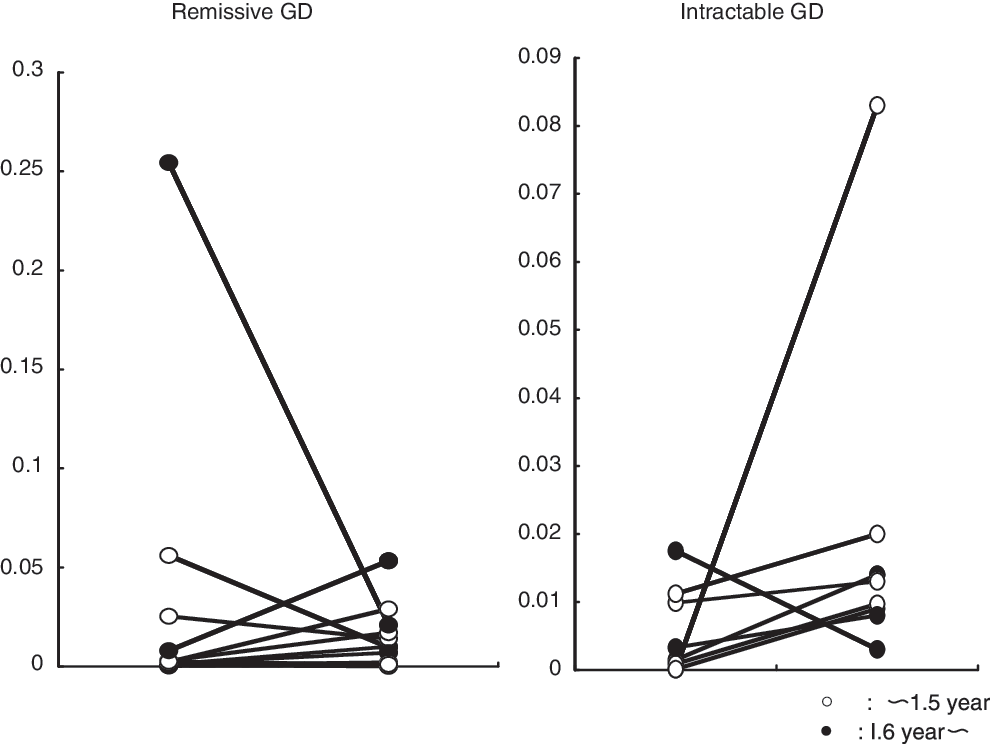
The serial changes of the TNFα:sCD40L ratio in intractable GD and remissive GD.
p<0.001.
p<0.01.
IL-18, interleukin-18; sCD40L, soluble form of CD40 ligand; TPO, thyroid peroxidase; TNFα, tumor necrosis factor-alpha; sTNFR1 and sTNFR2, soluble forms of TNFα receptors 1 and 2.
Discussion
It has been reported that several cytokines, such as IL-4, IL-5, IL-6, and IL-12, are increased in patients with active GD (19 –22). The serum concentration of IL-18 has also been reported to be increased (23 –25), with the exception of one report (26). The serum concentration of sCD40L has been reported to be increased (27) or decreased (28) in hypothyroid patients, while no data have been reported in patients with hyperthyroid GD. The serum concentration of TNFR1 has been reported to be increased in both hypothyroid (29) and active GD (30). Our results suggest that concentration of serum IL-18, sTNFR1, and sTNFR2 was increased in the GD-A or the GD-IT group, and moreover, it clearly showed that those concentrations were dependent on disease activity in GD.
While autoimmune thyroid diseases are quite common in the general population, their etiology and the mechanism by which they induce deterioration in thyroid function remain controversial. The seroconversion from thyrotropic immunoreaction to thyro-“suppressive” pattern during the clinical course and treatment of GD, and the coexistence of agonistic and antagonistic activity or anti-TSH receptor antibodies have occasionally been recognized in this disease. We have previously reported that Th2 cells were strongly induced by B cell activation via a CD40 pathway, resulting in overproduction of IL-10 in GD, and that CD8+ cells inhibited this series of responses (16). We have shown here that serum IL-18 levels in the GD-A group are significantly higher than in other thyroid disease groups, even in patients with treated (euthyroid) GD, suggesting the involvement of IL-18 in patients with hyperthyroid GD. This increase of IL-18 appears to be related to the activity of GD, as shown by the correlation with values of FT3 or TRAb. IL-18 plays an important role in the immune response through its ability to induce IFN-γ production in T cells and natural killer cells (31). IL-18 is also produced by macrophages during the innate immune response and has been shown to influence adaptive immunity (32). Further, IL-18 induces naive T cells to develop into Th2 cells, and is a unique cytokine that enhances innate immunity and both the Th1- and Th2-driven immune responses (33). Our results suggest that innate immunity and both the Th1- and Th2-driven immune responses are enhanced in hyperthyroidism. TSH has been reported to stimulate the expression of IL-18 in cultured thyroid cells, and methimazole suppressed this expression (34). The decrease of IL-18 in the GD-IA or the GD-R group might be related to the effect of treatment with antithyroid drugs.
We also examined whether the serum profiles of cytokines in GD patients might correlate with basal immunoreactivity during the clinical course of GD. Serum levels of proinflammatory cytokines, such as TNFR1, TNFR2, and CD40L, but not TNFα, were all increased in the GD-A group. The values of sTNFR1 or sTNFR2 were correlated with FT3 or TRAb, although no such correlation was found for sCD40L. These differences appear to reflect different roles among proinflammatory cytokines. Although the serum level of TNFα was not significantly decreased in the GD-A group, serum concentrations of TNFR1 and TNFR2 were significantly higher in the GD-A group than those in the GD-IA, GD-R, and CON groups. In addition, serum sCD40L levels were significantly lower in the GD-R group compared with the GD-A group. CD40L, in combination with IL-4, can enhance CD23 and CD25 expression on tonsillar B cells (35). Increased serum levels of sCD40L have been reported in various autoimmune diseases, as well as in atherosclerotic disease (11), and sCD40L is a risk factor for acute coronary disease (36). Increased sCD40L has also been reported to be associated with in vitro adhesion molecules and MCP-1 release, impaired migration in endothelial cells, and O2 generation in monocytes (37). Increased serum levels of sCD40L in hyperthyroid GD may therefore reflect a spectrum of inflammatory responses. Treatment with antithyroid drugs decreases serum levels of sCD40L and increases those of TNFα, resulting in an increased serum TNFα:sCD40L ratio. TNFα or CD40 binding has been reported to antagonize IL-10-mediated inhibition of DC function (38) and the change in this ratio may reflect these changes in immunological responses. The mean TNFα:sCD40L ratio was higher in the GD-R than in the GD-A group. These findings suggest to us that the assessment of cytokine profile during antithyroidal treatment in the patients with GD might contribute to the clinical assessment of their state with respect to remission in patients with treated GD. Long-term observations are needed, however, to evaluate the clinical significance of ratio of TNFα to sCD40L as a marker of remission for GD, since GD occasionally relapses several years after medication is discontinued. Further large-scale investigations are required to clarify this.
In conclusion, the serum profile of cytokines was shown to differ in patients with GD depending on their disease activity. Interestingly, an elevated serum TNFα:sCD40L ratio may reflect a shift from Th2 to Th1 dominance, which might initiate or maintain the remission of GD.
Footnotes
Acknowledgments
This work was supported by grants from Fujita Health University. The authors give special thanks to Ms. Saori Suzuoki and Ms. Natsuko Kimata for their excellent secretary work, and also appreciate Ms. Sayaka Nomura for her technical help.
Disclosure Statement
The authors declare that no competing financial interests exist.