
Abstract
Background:
Lungs and bones are the most common sites for distant metastases from papillary thyroid cancer (PTC). Metastases to the pancreas are extremely rare. Here we present a man with pancreatic metastases from PTC, report our experience with sorafenib therapy, and discuss the role of endoscopic ultrasound (EUS)-guided biopsy in its diagnosis.
Patient Findings:
A 56-year-old man underwent total thyroidectomy, right-modified neck dissection, and radioactive iodine (RAI) remnant ablation for PTC at age 47 years (in 2002). Between 2002 and 2007, he had three more neck surgeries, two RAI therapies, and external beam radiotherapy for persistent and subsequently metastatic PTC. In 2008, a computed tomography/positron emission tomography (CT/PET) scan showed an 18F-fluorodeoxyglucose (FDG)-avid pancreatic focus. Magnetic resonance imaging (MRI) revealed a pancreatic nodule at the same location. An EUS-guided biopsy confirmed the diagnosis of pancreatic metastasis from PTC, and molecular studies showed positive BRAF V600E mutation. He was treated with sorafenib for 6 months. Although a lung CT scan done 2 months after initiation of sorafenib suggested stability of the disease, MRI studies done at 3 and 6 months showed clear progression with an increase in the size of the lung and pancreatic metastases. Subsequently, he developed liver, bone, and omental metastases. He died in July 2011, 9 years and 8 months after the initial diagnosis of PTC and 20 months after discovery of the pancreatic metastasis.
Summary:
A middle-aged man with PTC developed lung metastases despite multiple surgeries and RAI therapies. Seven years after the initial diagnosis, a pancreatic metastasis was accidentally discovered. Both the metastasis and the primary thyroid tumor are positive for BRAF V600E mutation. The lung and pancreatic metastases progressed while the patient was receiving sorafenib for 6 months, and the patient died 20 months after diagnosis of pancreatic metastasis.
Conclusion:
PTC rarely metastasizes to the pancreas. In this patient, an FDG PET scan and EUS-guided biopsy played important roles in the diagnosis. PTC metastases to the pancreas usually occur in otherwise advanced disease. In the patient presented here, sorafenib may have slowed disease progression but the overall utility of tyrosine kinase inhibitors in pancreatic metastases from PTC is not clear.
Introduction
Patient
A previously healthy 47-year-old man was referred to our hospital in December 2001 with a right neck mass of 2-month duration. An ultrasound (US) of the neck revealed a 3.5-cm right thyroid nodule and multiple abnormal right cervical lymph nodes. A US-guided fine-needle aspiration biopsy (FNA) confirmed the diagnosis of PTC. The patient underwent total thyroidectomy with right central and lateral-modified neck dissection in February 2002. The tumor was adherent to the trachea and strap muscles, but there was no evidence of tracheal invasion. The histopathological examination confirmed the diagnosis of a 2-cm classic type of PTC in the right thyroid lobe with extrathyroidal extension and multiple lymph node metastases. The Tumor–Node–Metastases (TNM) stage was IVA (T4aN1bM0). There was no evidence of poor differentiation. In April 2002, the patient received 148 mCi for thyroid remnant ablation after withdrawal of thyroid hormones for 5 weeks. At that time, serum thyroglobulin (Tg) was 300 ng/mL with Tg autoantibodies <20 IU/L and thyroid-stimulating hormone (TSH) was 51 mIU/L, and preablation diagnostic radioactive iodine (RAI) whole-body scan (DxWBS) showed 0.2% uptake in the thyroid bed only. Postablation DxWBS showed similar findings without evidence of distant metastases. In October 2002, serum Tg while on
In July–August 2005, the patient received 6000 cGy of external beam radiotherapy to the lower neck and mediastinum. Following the fourth surgery and external beam radiotherapy, serum Tg while on
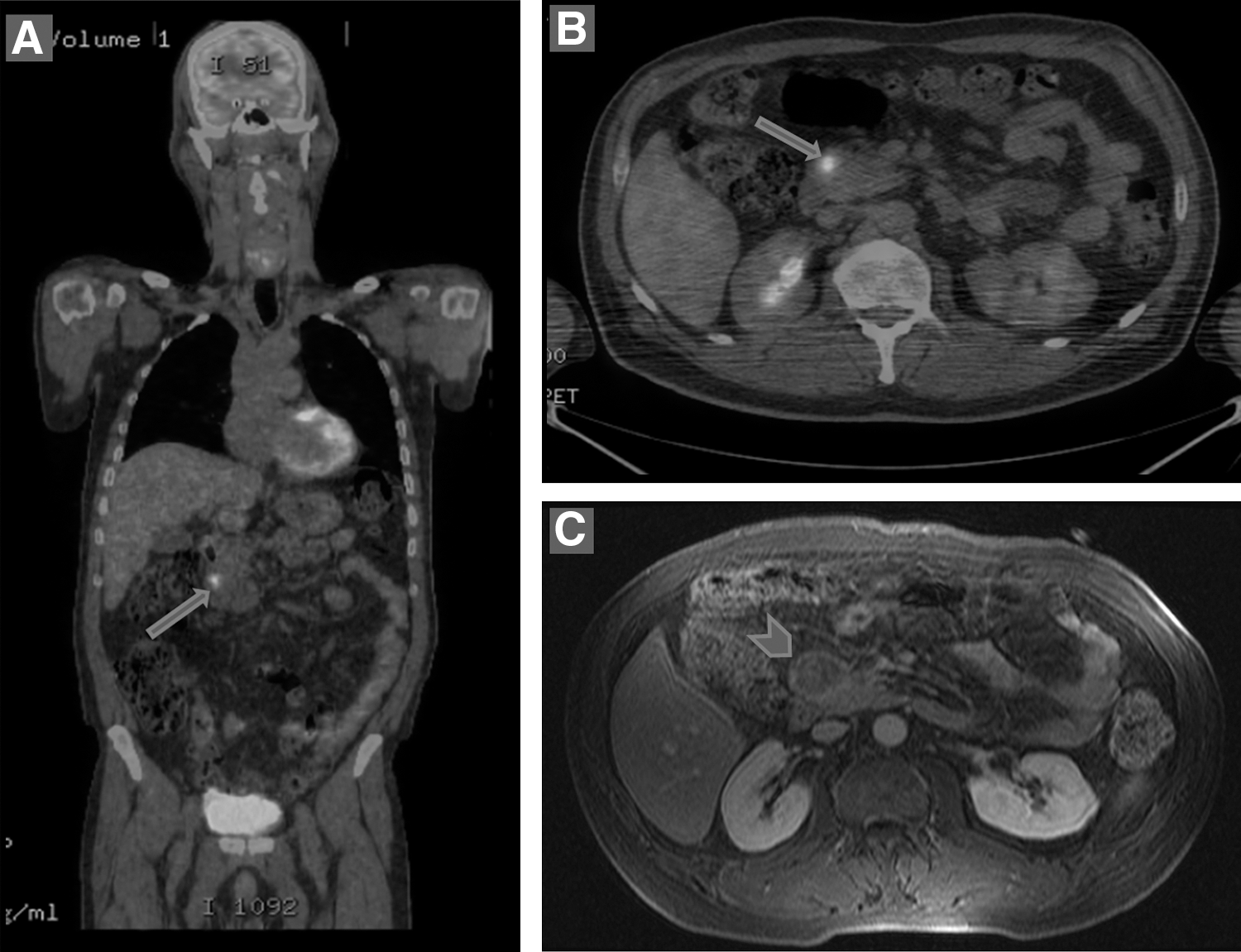
In November 2009, CT/PET whole-body scan revealed further progression of the lung metastases and a new lesion in the unicinate process of the pancreas (Fig. 1). An MRI of the pancreas confirmed the presence of a 1.7-cm pancreatic lesion (Fig. 1). An EUS-guided biopsy confirmed the diagnosis of pancreatic metastasis from PTC (Fig. 2). Part of the specimen was used for extraction of DNA for BRAF mutation testing. Using previously published primers and PCR conditions, exon 15 of the BRAF gene was amplified and directly sequenced (14). The result revealed the presence of BRAF
V600E mutation (Fig. 2). The same mutation was also confirmed in the original tumor obtained from the total thyroidectomy sample that was performed in February 2002. Due to the progression of the disease, the patient was referred to an oncologist for sorafenib therapy. He was started on sorafenib 400 mg orally twice daily in August 2009. He tolerated the drug well. Although chest CT scan performed 2 months after initiation of sorafenib showed mild improvement in the size of the lung metastases, serum Tg while on
Sagittal
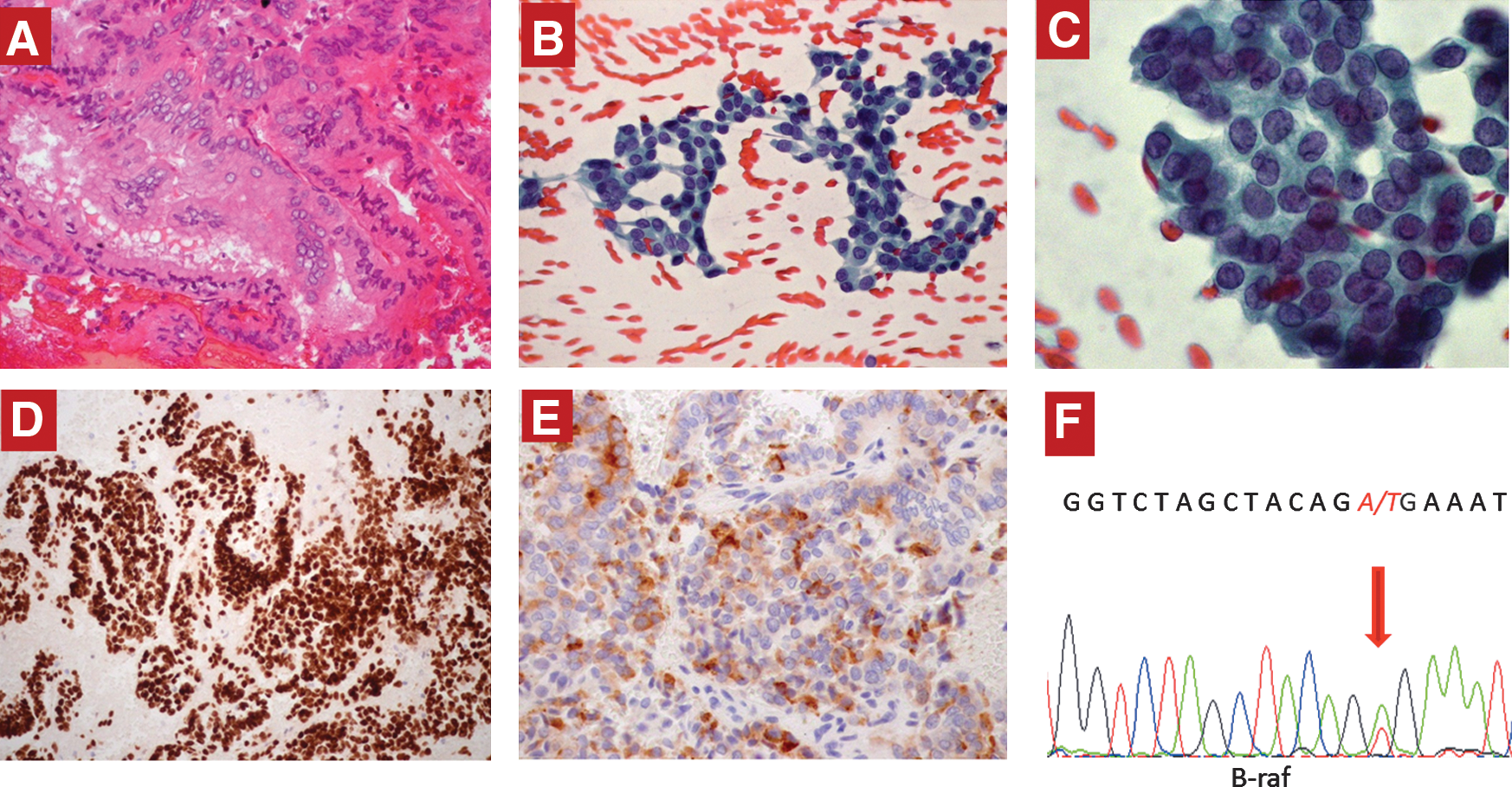
Histopathological and molecular studies of the pancreatic biopsy specimen, including
Discussion
In this report, we have described a middle-aged man with classic type of PTC who underwent total thyroidectomy and neck dissection and received RAI ablation. His disease continued to progress despite three more surgeries and three doses of RAI therapy (cumulative dose 496 mCi). He subsequently developed distant metastases to the lungs that showed no evidence of RAI uptake. The patient eventually developed a pancreatic mass that was discovered on CT/PET scan and confirmed on MRI of the pancreas. The nature of this lesion was confirmed to be metastatic PTC on histopathological examination of an EUS-guided biopsy. Molecular study showed the BRAF V600E mutation that is known to be associated with more aggressive forms of the disease (15).
Differentiated thyroid cancer (DTC) has been reported to present initially with distant metastases in about 4% of cases (16). During follow-up, distant metastases develop in 2%–34% of cases (7). The risk of distant metastases is related to the risk group of patients (4,5,17). Elderly patients are more likely to develop distant metastases and die from their disease when it is distantly metastatic (4,5,18). Distant metastases are strongly associated with increased risk of death from DTC (4,5). In patients with distant metastasis, the overall survival is 42% at 10 years, 33% at 15 years, and 29% at 20 years (4,5). The disease-specific survival rates are 40% at 5 years, 27% at 10 years, and 24% at 15 years (4,5). The most common sites for distant metastases in DTC are the lungs and, less commonly, the bones (4,5,19). Other sites are very infrequently involved. Metastases to the abdominal organs are quite rare. The most common site for abdominal metastases is the liver (7). However, metastases from DTC to the liver represent only 0.5% of all distant metastases from DTC and are frequently part of widespread distant metastases to other organs, although isolated liver metastases have been rarely described (7). Pancreatic metastases from DTC are extremely rare. To our knowledge, only seven patients have been identified in the literature (summarized in Table 1). Two of these patients had the tall cell variant of PTC (8 –13). Similar to our patient, most previously reported patients had known advanced DTC with metastases to other organs when they were found to have pancreatic metastases (8 –13). However, Angeles-Angeles et al. described a 72-year-old man whose initial presentation was abdominal pain due to a pancreatic mass that was thought to be a primary pancreatic tumor (8). The patient underwent pancreatectomy, and the histopathological examination showed features consistent with PTC. His investigations revealed PTC in an asymptomatic intrathoracic goiter with metastases to the vertebrae, brain, and pancreas (8).
PTC, papillary thyroid cancer; TC-PTC, tall cell variant-papillary thyroid cancer; FV-PTC, follicular variant-papillary thyroid cancer; CLNs, cervical lymph nodes; PET, positron emission tomography; RAI, radioactive iodine therapy; EUS-FNA, endoscopic-ultrasound-guided fine-needle aspiration biopsy; Dx, diagnosis; CT, computed tomography; US, ultrasound.
In most patients, pancreatic metastases and other metastatic foci lose their ability to take up RAI (5,7). Six of the eight patients who have been described in the literature and summarized in this report had non-RAI avid pancreatic metastases (8 –12). In the other two cases, no information on RAI uptake was available. Four cases were discovered on FDG PET or CT/PET scan done for evaluation of elevated Tg (9,12) while the other four cases were diagnosed by abdominal CT scans done for investigation of abdominal complaints (8,10,11,13). Their RAI nonavidity and FDG uptake suggest that these tumors were of a high grade (20). In our patient, this was further supported by the finding of a BRAF V600E mutation that had been found to correlate with poor prognosis in most studies (21). Of all the previously reported cases, only two were investigated for the presence of the BRAF V600E. Similar to our case, the BRAF V600E mutation was found in one case. However, testing for BRAF V600E was negative in the other case, and RET/PTC1 rearrangements were not detected in either case (9).
Once found on conventional imaging, pancreatic metastases are best confirmed by obtaining tissue for cytological or histopathological examination. EUS with EUS-guided biopsy is a very useful and easy technique if performed by an experienced endoscopist. This technique is especially sensitive for small pancreatic lesions (<2 cm) that may not be seen on CT scans (22,23). The sensitivity of EUS-guided biopsy ranges between 75% and 90% and is superior to CT-guided FNA (24,25). In our case, it yielded an adequate amount of tissue for cytopatholgical examination and DNA preparation for BRAF V600E mutation screening. Our patient is the second of the previously described cases of pancreatic metastases from DTC in which EUS-guided biopsy was used for the diagnosis (Table 1).
Due to the rare occurrence of pancreatic metastases from DTC, the best management for this condition is not clear (7). Since most cases are associated with metastases in other sites, surgical excision, with its attendant risks and limited efficacy, is not a practical solution. However, in cases where metastases are associated with significant compression of the adjacent structures and are causing obstructive jaundice or gastric outlet obstruction, palliative endoscopic or surgical procedures may be necessary. Interestingly, the surgical option was used in most previously described patients, in two patients primarily as a diagnostic procedure and in the other five patients as a therapeutic intervention (Table 1). Each of the previously reported patients had one reason or another to perform surgery. In one patient, the patient presented with abdominal pain and was found to have a pancreatic mass suspected to be a primary pancreatic neoplasm as he was not known to have thyroid cancer (8). In another patient, a pancreatic metastasis from thyroid cancer was considered a low possibility (9). It is unclear why biopsy was not performed in these two patients and pancreatic surgery was chosen as a diagnostic/therapeutic procedure. In another patient, the patient had severe bleeding from a pancreatic metastasis that invaded the duodenal wall and pancreatecoduodenectomy was performed to control bleeding (11). In two patients, surgery was performed due to abdominal pain (10,13). In two other patients, surgery was performed in an attempt to control the disease (9,12). With the exception of one patient who was reported to remain stable at 24 months after surgery (12), the disease progressed in all of these patients and pancreatic surgery did not seem to have had a long-term impact on the course of the disease (Table 1). Fortunately, none of those patients were reported to have suffered operative complications.
Tyrosine kinase inhibitors have been recently introduced for therapy of DTC (26,27). Sorafenib is a small multikinase inhibitor of the BRAF gene product, of platelet-derived growth factor receptor, rearranged in transformation (RET), kit kinase, and vascular endothelial growth factor receptor-2 (28). It was approved by the Food and Drug Administration for the treatment of renal cell and hepatocellular carcinoma. Previously reported phase II trials demonstrated therapeutic efficacy of sorafenib (29,30). Gupta-Abramson et al. reported 68% stability of disease and 32% partial response and progression-free survival of 21 months in patients with metastatsic progressive DTC (29). Kloos et al. reported 61% stable disease, 15% partial response, and 15 months of progression-free survival in patients treated with sorafenib for progressive PTC (30). In a recent trial combining sorafenib as an inhibitor of the mitogen-activated protein kinase (MAPK) pathway and tipifarnib, a farnesyltransferase inhibitor that inactivates Ras and other proteins, partial response rate was 4.5%, and stable disease for at least 6 months was 36% (31). In our patient, despite seemingly initial stabilization of the disease in the first 2 months of therapy, clear progression of the disease occurred while he was receiving sorafenib although the pattern of progression seemed to have become more rapid after discontinuation of the drug.
In summary, our patient and the previously described patients showed that pancreatic metastases from DTC can be readily and safely diagnosed with EUS-guided biopsy. Pancreatic surgery is generally ineffective approach for their management although it may have a palliative role but does not affect long-term survival. They are also not RAI responsive and are frequently associated with widespread metastases and poor outcome. This patient did not respond well to sorafenib but further experience is needed to determine the overall response rate to sorafenib in DTC with pancreatic metastases.
Footnotes
Disclosure Statement
The authors declare that there is no conflict of interest that could be perceived as prejudicing the impartiality of the research reported.