
Abstract
Background:
Secretion of cytokines and expression of cytokine receptors have been reported in the orbital connective tissue in Graves' orbitopathy (GO). Lacrimal glands are putative autoimmune targets, and changes in tear film and ocular surface have also been described. Our aim was to characterize the cytokine profile of tears in patients with Graves' disease (GD) with and without orbitopathy.
Methods:
Tear samples were collected from 54 eyes of GO patients (age 43.4±15.2 years), 18 eyes of GD patients (age 46.8±11.7 years), and 24 control eyes (age 38.6±13.8 years). Patients underwent ophthalmological examination including Clinical Activity Score (CAS). The level of interleukin (IL)-1β, IL-6, IL-13, IL-17A, IL-18, tumor necrosis factor (TNF)-α, and RANTES (regulated upon activation, normal T-cell expressed, and secreted) as well as plasminogen activator inhibitor-1 (PAI-1) were measured by multiplex bead array and release values were calculated.
Results:
The release of IL-1β, IL-6, IL-13, IL-17A, IL-18, TNF-α, and RANTES were significantly higher in GO patients compared to controls (p<0.05). There was a 2.5-fold increase of IL-6 release. No significant differences were found in cytokine release between the GO and GD groups. In the GO group, significant positive correlation was found between CAS and the release of IL-6 and PAI-1 into tears (r=0.27, p<0.05 and r=0.24, p<0.05, respectively). PAI-1 release was significantly higher in GO than in GD patients and was increased in both the GD and GO groups compared to controls.
Conclusions:
Impaired cytokine balance has been observed in tears of GO patients. Secretion of IL-6 into tears might be a useful indicator of disease activity in GO.
Introduction
Immune activity in orbitopathy is neither synonymous nor coincident with the clinical severity of eye disease (12). Several approaches have been proposed to evaluate disease activity in GO. Among them, Clinical Activity Score (CAS) (13) has been shown to be a useful method in everyday clinical practice.
Although the inflammation takes place in the retrobulbar space, changes in the anterior segment of the eye also appear in GO. Tears play an essential role in maintaining the homeostasis of the ocular surface. Cytokine release into tears is involved in the recruitment and activation of inflammatory cells. Alternations in the pattern of tear cytokine balance can be observed during the day (14) or by eye closure (15). Studies on tear cytokines have shown that many ocular or systemic diseases lead to changes in the cytokine profile of the tear film (16). Changes in cytokine levels in human tears can be caused by seasonal allergic conjunctivitis (17), cystic fibrosis (18), and even anti-glaucoma eyedrops (19). Sjögren's syndrome and keratoconjunctivitis sicca are also accompanied by alterations of cytokine balance in the tear fluid and conjunctival epithelium (20), and IL-6 and TNF-α levels are elevated in tears of patients with dry eye (21). Passive cigarette smoke exposure leads to alterations of the tear film and increased tear inflammatory cytokine levels (22). Similar changes in tear composition of healthy smokers and patients with GO have been reported (23).
Early studies reported abnormally high tear osmolarity and rapid tear film break-up time in patients with GO (24). Alterations in tear film profile, low break-up time, and Rose Bengal staining in late GO indicate the presence of drying epithelial cells (25). Changes in tear protein profile by high-performance liquid chromatography have also been published, suggesting that GO has an effect on the lacrimal gland (26). Lacrimal gland enlargement was found in 22% of GO patients by orbital computed tomography (27). Expression of the thyrotropin (TSH) receptor on lacrimal gland acinar cells has also been reported. In GO, TSH may bind to these cells causing lacrimal gland impairment (28). Also, lacrimal glands have been described as target organs for thyroid hormone (29). Probable involvement of the lacrimal gland as an area of immunological reaction in GO have been suggested based on octreotide scintigraphy (30,31). Impression cytology findings also underline the ocular surface changes in GO (32). According to proteomic analysis (biomarkers with a molecular weight between 3000 and 20,000 Da) the majority of tear proteins are down-regulated in GO, with only few overexpressed proteins (33). Specific polymorphisms in proinflammatory cytokine genes (IL-12, interferon γ [IFNγ], TNF-α, and IL-1β) are associated with susceptibility to GO among GD patients (34,35).
Plasminogen activator inhibitor-1 (PAI-1), besides being an inhibitor of fibrinolysis, also plays an important role in the regulation of vascular function and tissue remodelling (36,37). TNF-α is an agonist for PAI-1 expression, and the role of this cytokine in PAI-1 gene activation is well established (38). Increased PAI-1 activity has been found in the serum of GD patients (39).
In the present study, we investigated the cytokines IL-1β, IL-6, IL-13, IL-17A, IL-18, and TNF-α and the chemokine RANTES as well as PAI-1 in tear samples of patients with Graves' orbitopathy (GO), in patients with GD without orbitopathy, and in healthy controls.
Methods
Tear samples were collected from 54 eyes of 27 patients with GO (6 men, 21 women, age 43.4±15.2 years) and 18 eyes of nine GD patients without orbitopathy (one man, eight women, age 46.8±11.7 years) according to standard criteria (40). Patients underwent careful detailed ophthalmological examination (slit lamp microscopy, corneal staining, Schirmer I test, tear film break-up time [BUT], Hertel exophthalmometry, and indirect ophthalmoscopy). Before tear collection, the anterior ocular status of each subject was carefully assessed: a slit-lamp under low illumination was used to avoid reflex tearing, while all other ophthalmological evaluations were performed after sample collection. The CAS (13) was obtained in each case. None of the patients used any topical eye medications; only nonpreserved artificial tears were allowed, which could not be instilled on the morning of sample collection. Thyroid status including serum hormone levels (TSH, free thyroxine [FT4], free triiodothyronine [FT3], TSH receptor binding antibodies) were determined within a 5-day interval before or after tear collection using electrochemiluminescence immunoassay (TSH, FT3, FT4 assay by Elecsys/Cobas Roche Diagnostics GmbH, Mannheim, Germany). History of smoking and any significant general or ophthalmological disease were taken. The control group (C) consisted of 24 eyes of 12 healthy volunteers (four men, eight women, age 38.6±13.8 years). All enrolled patients gave informed consent and the Institutional Review Board approved the study protocol in accordance with the 1989 Declaration of Helsinki.
Tear samples were obtained by capillary flow with no nasal stimulation or previous installation of drugs or vital dyes, by the same examiner (BU). No anesthetic drops were instilled; samples were collected nontraumatically from the inferior meniscus without touching the cornea, conjunctiva, or eyelids. The amount of the tear sample collected (μL) and the collection time (seconds) were recorded. The samples were frozen without centrifugation within 15 minutes of collection and stored at −70°C until cytokine measurements were performed. Preliminary studies had demonstrated that centrifugation of the samples did not influence cytokine concentrations.
Levels of cytokines were measured by a multiplex bead array method. Combined FlowCytomix™ Simplex Kits were used with an appropriate FlowCytomix™ Basic Kit according to the manufacturer's instructions (Bender MedSystems GmbH, eBioscience Company, Vienna, Austria). Briefly, tear samples (in some cases diluted samples) or serial dilution of mixed cytokine standards were added to the wells of filter microplates containing the fluorescent cytokine capture bead mixtures. Biotin conjugated anti-cytokine antibody mixtures were applied, and the plates were incubated at room temperature for 2 hours and protected from light on a microplate shaker. The filter plates were washed using a MultiScreen HTS Vacuum Manifold (Millipore, Billerica, MA). Phycoerythrin-conjugated streptavidin solution was added to the samples and they were further incubated for 1 hour as described. Plates were washed again, then 150 μL of sample buffer was added to the wells, and sample data were acquired by multiparameter flow cytometric analysis with a FACS Array cytometer (BD Biosciences Immunocytometry Systems, San Jose, CA).
Data were analyzed with the BenderMedSystems FlowCytomix™ Pro 2.4 software. During the preparation of the human cytokine standards, additional dilutions were applied to achieve higher sensitivity, and modified standard curves were generated during the analysis. Assay sensitivities were 4.2 pg/mL for IL-1β, 1.2 pg/mL for IL-6, 4.5 pg/mL for IL-13, 2.5 pg/mL for IL-17A, 3.3 pg/mL for IL-18, 3.2 pg/mL for TNF-α, 25 pg/mL for RANTES, and 13.5 pg/mL for PAI-1.
Tears were collected from each eye for 2 minutes. For more precise evaluation we measured with a timer the exact collection time in seconds. The amount collected was also registered. The volume was calculated from the length of the tear column in the tube (100-mm length by 0.5-mm inner diameter capillary tubes were used) and was also checked when pipetting the samples for evaluation. We got the results of the flow cytometric assay in picograms per milliliter for all cytokine concentrations (C). The result was multiplied by the volume of tears collected (V, in μL) and divided by the collection time (t, in seconds):
The 2-minute cytokine release values (pg/2 min) were used for further statistical analysis.
Statistical analysis was carried out using the SAS for Windows 8.2 software. Hormone and cytokine levels in the three study groups (GO, GD, and C) were compared by analysis of variance (ANOVA) with Duncan post hoc testing. Both cytokine levels and cytokine releases were correlated with patient age, clinical parameters (CAS, Schirmer I test), and smoking (number of cigarettes per day) by Spearman correlation analysis.
Results
Medians and upper and lower quartiles of both concentrations and release values of cytokines in each patient group are shown in Table 1. Because release values reflect the real cytokine production, these were used for further analysis.
Values were compared by analysis of variance (ANOVA) with Duncan post hoc testing.
Values are significantly different from control (p<0.05).
PAI release and concentration are significantly higher in the GO group compared to the GD group.
PAI, plasminogen activator inhibitor; IL, interleukin; C, controls; GD, Graves' disease without orbitopathy; GO, Graves' orbitopathy; TNF, tumor necrosis factor; RANTES, regulated upon activation, normal T-cell expressed, and secreted.
ANOVA showed significant difference between the cytokine release values measured in the GO and C groups. The release of IL-1β, IL-6, IL-13, IL-17A, IL-18, TNF-α, and RANTES were significantly higher in the GO group as compared to the C group (p<0.05). No significant difference was found between GD and group C in the release of the cytokines tested. Also, no statistically significant differences were found between the cytokine release into the tears of GO and GD patients regarding any cytokine tested, although release values tended to be higher in the GO group; i.e., the values of GD patients were intermediate between the GO and C groups in the case of all cytokines (Fig. 1). Release of PAI-1 into tears was significantly higher in the GO group compared with GD patients, and both GO and GD patients' PAI-1 release values were significantly higher than the C group's (Table 1).
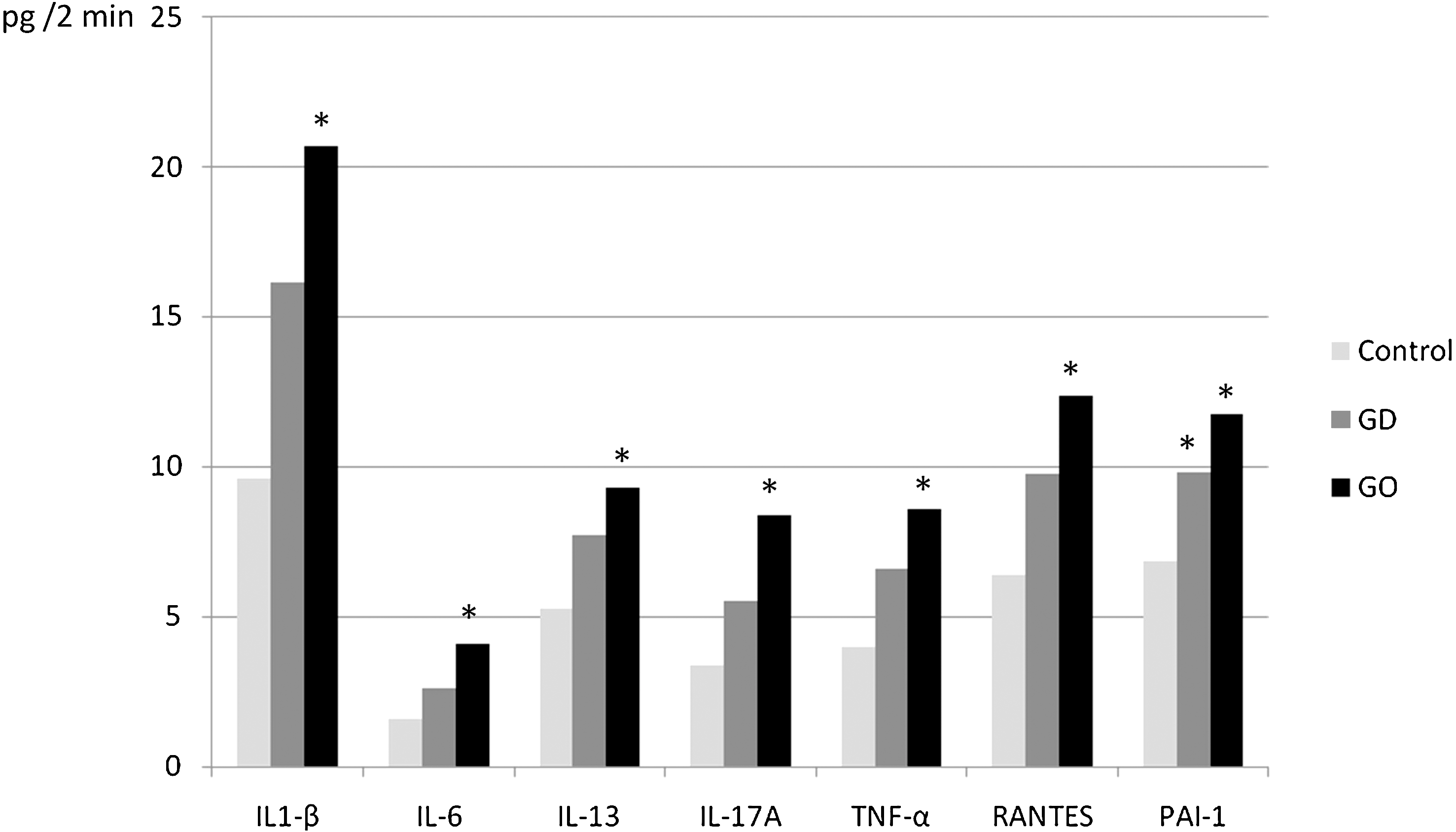
Median of tear cytokine and PAI-1 release values into tears (pg/2 min). GD patients were intermediate between the GO and the C groups in the case of all cytokines. This also applies to IL-18 (not shown in the figure). Cytokine releases marked with an asterisk (*) are significantly different from controls (p<0.05).
Positive correlations were found between the release of all tested cytokines and the secretion of PAI-1 in tears (IL-1β: r=0.23, p=0.002; IL-6: r=0.31, p=0.001; IL-13: r=0.30, p=0.001; IL-17A: r=0.23, p=0.015; IL-18: r=0.24, p=0.012; TNF-α: r=0.29, p=0.002; and RANTES: r=0.23, p=0.014).
We found strong correlation between the release of all examined cytokines, with the correlation coefficients ranging between 0.66 and 0.97 (p<0.01 in all comparisons). The strongest correlations were detected between the release of IL-1β and RANTES (r=0.96, p<0.001), as well as IL-1β and the other members of the IL-1 family (IL-18: r=0.97, p<0.001; IL-17A: r=0.89, p<0.001).
Except for IL-17A, we found no correlation between tear cytokine concentrations and age; for IL-17A, the correlation was negative (r=−0.21, p<0.05). Also, a weak negative correlation was found between age and PAI-1 release (r=−0.24 p<0.05). ANOVA showed no significant difference between the GO and GD groups regarding serum TSH, free thyroid hormone (FT4, FT3) and TSH receptor antibody levels.
We found significant differences between the left and right eyes in the release of all examined cytokines by both paired t test and Wilcoxon matched pairs test (p<0.05 for all examined cytokines, and p<0.001 for IL-6, IL-18, and PAI-1).
Ophthalmological evaluation of GO patients showed the signs of ocular surface drying. However, no corneal pathology (fluorescein staining, erosion, or ulceration) was present at the time of sample collection. Schirmer I test showed a mean lacrimal secretory capacity of 13.94±10.07 mm in the GO group, 14.22±8.04 mm in the GD group, and 19.37±9.17 mm in the C group; differences between the GO and GD patient groups were not statistically significant, however, both were significantly lower than the C group. The mean BUT was 3.58±2.35 seconds in the GO group [range from 4 to 32 seconds in healthy adults (41)]. The CAS in the GO group was 3.82±2.0.
Positive correlations were found between Schirmer I test and the release of all tested cytokines in the C group (IL-1β: r=0.53, p=0.002; IL-6: r=0.46, p=0.01; IL-13: r=0.50, p=0.005; IL-17A: r=0.54, p=0.002; IL-18: r=0.54, p=0.002; TNF-α: r=0.52, p=0.003; RANTES: r=0.56, p=0.001). Similarly, positive correlation were found between Schirmer I test and the release of PAI-1 in the C group (r=0.40, p=0.002). However, none of the cytokine release values were correlated with the lacrimal secretory capacity (Schirmer I test) and the BUT in the GO or GD group. We found a weak positive correlation between Schirmer I test and PAI-1 release in the GO group (r=0.28, p=0.04) but not in the GD group.
In the GO group, a positive correlation was found between IL-6 release and the CAS (r=0.27, p<0.05) as well as between IL-6 release and the degree of eyeball protrusion (millimeters in Hertel exophthalmometer) (r=0.34, p<0.05). Also positive correlation was found between PAI-1 release and the CAS (r=0.24, p=0.03).
Among the 27 GO patients, 10 were former or current smokers (cumulative number of cigarettes smoked 78,309±53,631 consuming an average of 14.73±6.61 cigarettes/day), while among the nine GD patients without orbitopathy, six were former or current smokers (cumulative number of cigarettes smoked 85,166±10,1169 with an average of 11.67±10.81 cigarettes/day). In the C group, no patient was a current or former smoker. We found no connection between tear cytokine levels or release values and smoking (by the number of cigarettes per day, or using dichotomized variables yes/no). When the cytokine release values were analyzed in all patients irrespective of the presence of GO, as well as in controls, and were regrouped according to smoking history, no differences were found in the release of any examined cytokine.
Discussion
Tears play an essential role in maintaining the homeostasis of the ocular surface. Many ocular or systemic diseases have been shown to lead to changes in the cytokine profile of the tear film (16 –21). In this study, we monitored the level of a selected set of cytokines that included TNF-α, IL-1β, IL-6, IL-18, IL-17A, IL-13, the chemokine RANTES, and PAI-1 in tear samples of Graves' patients with and without orbitopathy.
The multiplex bead array, which was used in the present series of experiments, is a highly sensitive technique that enabled us to carry out parallel measurements of multiple cytokines by flow cytometry in a small amount of tears. In contrast to previous results showing higher tissue concentrations of TNF-α, IL-1β, and IL-6 (42) as well as serum concentrations of IL-6 (43) and PAI-1 in GD when compared to healthy controls, we found no significant difference between the GD and C groups in the release of tear cytokines. These findings indicate that tear cytokines are regulated differently, and the appearance of proinflammatory cytokines in the tears of patients with GO, but not in those with GD without orbitopathy, is not the result of the thyroid disease but the orbitopathy itself. Sources of cytokines and chemokines in tears may include the main and accessory lacrimal glands, the corneal and conjunctival fibroblasts, and the immunovigilant cells normally present in the ocular surface (44). Previous studies have shown that the lacrimal gland is involved in GO and that it could also be an area of immunological reaction (26 –31). Reports have been published on the early conjunctival involvement in GD, suggesting that ocular surface impairment in GO is not only a consequence of mechanical events, but that ocular surface tissues are direct targets for autoantibodies in GD (45). Conjunctival and episcleral inflammation can occur before the classic signs of orbitopathy, and the pathogenesis is assumed to be similar to that involved in the extraocular muscle inflammation and lymphocytic infiltration in GO (46).
In our study, we found a significant increase of cytokine release of TNF-α, IL-1β, IL-6, IL-18, IL-17A, IL-13, and RANTES in the tears of the GO patient group as compared to controls. The importance of the macrophage-derived cytokines TNF-α and IL-1β in GO have been described (5,6) and were shown to stimulate ICAM-1 expression and glycosaminoglycan production by orbital fibroblasts (9). High release of TNF-α and IL-1β into tears of patients with GO may indicate their presence not only in the retrobulbar connective tissue, but also in the lacrimal gland and ocular surface. IL-1β–activated fibroblasts express high levels of T-cell chemoattractants such as RANTES (10), which may explain the increased release of RANTES in tears of patients with GO. A strong correlation between the releases of IL-1β and RANTES as well as IL-1β and IL-18 was also demonstrated in our study. Increased IL-18 serum levels in both GO and GD individuals have also been observed by others (47). In our study, however, elevated release of IL-18 could be measured only in the tears of GO patients, but not in the GD or the C group.
As we found a more than twofold IL-6 release in the tears of the GO group as compared to controls, we theorize that elevated IL-6 release in tears might be an indicator of disease activity. This assumption is further supported by the fact that in the GO group, we found a positive correlation between IL-6 release and the CAS. A positive correlation was also found between IL-6 release and the degree of eyeball protrusion.
Others found serum IL-6 levels to be elevated in hyperthyroid GD and GO (43). However, the serum levels are influenced by additional factors, such as thyroid status and therapy, which limits its use as an activity indicator in GO (8). Elevation of IL-6 tear concentration has also been described in dry eye and dysfunctional tear syndrome (48). Although GO is accompanied by dry eye, including the tear deficient form (non-Sjögren type dry eye) (24) and the evaporative form due to exophthalmos (25), GO is not associated with Sjögren's syndrome. IL-6 levels in tears of Sjögren's syndrome patients are higher than in non-Sjögren type tear-deficient dry eye (21). To evaluate lacrimal secretory capacity we performed the Schirmer I test. In both the GO and GD groups, tear secretion was diminished. Our findings correspond to the results of Gurdal et al. (49) who found significantly lower Schirmer test readings between GD patients, with and without orbitopathy, than in controls. The authors suggested that ocular surface damage and accompanying surface inflammation may precede the development of classic GO symptoms (49). However, elevated proinflammatory cytokine secretion into tears may also be the consequence of ocular surface inflammation, even when inflammation cannot be detected with clinical examination methods, and thus considered as an early sign for ocular involvement in GD. In the C group, we found a positive correlation between Schirmer I test and all the released cytokines that were measured, including IL-6. However, neither positive or negative correlations between the Schirmer I test and cytokine releases were detected in the GO and GD groups. This important finding supports the notion that increased cytokine releases are not the result of decreased lacrimal secretory capacity. Instead, cytokine release and lacrimal secretory capacity are two distinct mechanisms. The lacrimal glands' tear secretory function is damaged in GO and GD, while cytokine release is increased as part of the immune process.
IL-13 is a Th2 cytokine that plays a role in IgE-mediated immunity. In chronic ocular inflammation, where keratopathy is present, an increased level of IL-13 can be observed together with eotaxin-1 (50). About 30% of patients with GD have increased concentrations of IgE in their sera, and in one third of patients with hyperthyroid GD, Th2 cells are stimulated and secrete excess amounts of IL-13 (51). The elevated release of IL-13 in tears of patients with GO might be related to high serum IgE or may be simply an indicator of ocular surface repair of clinically nondetectable exposure keratopathy. The latter assumption is supported by the lack of fluorescein staining during slit lamp examination in all of our patients.
We believe that, to some extent, the ocular surface including the conjunctiva is involved in the autoimmune process in patients with GD. Cytokine release values of the GO group were higher only when compared to the tears of healthy controls, while cytokine releases of the GD group did not differ from either the GO or the C group. However, the release values tended to be highest in the GO group, followed by the GD and C groups (Fig. 1). We assume that this might be the result of the clinically nondetectable orbital involvement of patients in the GD group. We speculate that there are GD patients who fail to present with clinically detectable orbitopathy, although their orbital connective tissues and lacrimal glands are already affected. Subclinical eye involvement is common in the orbits: extraocular muscle enlargement has been found in nearly 70% of adult patients with Graves' hyperthyroidism by orbital imaging (52). Subclinical eye involvement in GD might remain silent but may proceed to manifest GO, resulting in continuous changes in the orbital structures that are represented in tears. Thus, tear cytokine release in these GD patients tends to be higher than in controls but remains below the values of GO patients, representing the possible manifestation of a subclinical disease.
PAI-1 release was significantly higher in the GO group than in the GD group and was higher in both the GO and GD groups than in group C (Table 1). Others have reported higher PAI-1 concentrations in the plasma of GD patients compared to controls (39). In our series, the only protein that we examined, that showed a statistically increased release in GO patients compared with GD patients, was PAI-1. The tissue remodeling function of PAI-1 (36,37) may account for the difference between the GD and GO groups, and favor more release in the latter. The role of PAI-1 in tears of normal healthy eyes is the maintenance of ocular surface integrity (53). Strong positive correlations have been found between the release of all examined cytokines and the release of PAI-1 in tears, supporting the previously described role of cytokines in PAI-1 gene activation (38). Both IL-6 and PAI-1 releases correlated with the CAS in our patients. PAI-1 release in tears may either be an indicator of disease activity in GO or simply the result of anterior segment changes in GO, which are also represented in the CAS. However, unlike IL-6 release, PAI-I does not seem to be a practical marker of disease activity in GO.
Passive cigarette smoke exposure leads to alterations in the tear film and increase in inflammatory cytokine levels (22). Similar changes in the tear composition of healthy smokers and patients with GO have been reported (23). We found no correlations between tear cytokine levels or releases and smoking history. Previously, Salvi et al. (8) described similar findings. Their findings were that there were no changes in serum IL-6, TNF-α, and IL-1β concentrations induced by smoking.
We are not aware of any previous studies on cytokines and PAI-1 in tears of patients with GD. We are the first to show that there is a correlation between disease activity and IL-6 release in tears in GO. Our findings demonstrate that GO results in changes in the cytokine profile of the tear film. We detected an elevation of the pro-inflammatory cytokines TNF-α, IL-1β, IL-6, IL-18, IL-17A, IL-13, and RANTES in the tears of patients with GO. Correlations between IL-6 release in tears and CAS as well as the degree of eyeball protrusion were also detected. We propose that high IL-6 release in tears may serve as a useful indicator of disease activity in GO.
Footnotes
Acknowledgment
The authors would like to thank Zsolt Karanyi for his contribution during the evaluation of the data and preparation of the manuscript.
Author Disclosure Statement
No competing financial interests exist.