
Abstract
Background:
Rare cases of Graves' disease occurring years after subacute thyroiditis (SAT) have been reported. Here, we present the first known case of simultaneous occurrence of Graves' disease and SAT.
Patient Findings:
A 41-year-old woman presented with 10 days of neck pain, dysphagia, and hyperthyroid symptoms. Neck pain had initially started at the base of the right anterior neck and gradually spread to her upper chest, the left side of her neck, and bilateral ears. Physical examination revealed a heart rate of 110 beats/minute and a diffusely enlarged tender thyroid gland without evidence of orbitopathy. There was a resting tremor of the fingers and brisk deep tendon reflexes. Laboratory values: thyrotropin<0.01 mcIU/mL (nL 0.39–5.33), free thyroxine 2.0 ng/dL (nL 0.59–1.60), free T3 6.6 pg/mL (nL 2.3–4.2), thyroglobulin 20.1 ng/mL (nL 2.0–35.0), thyroglobulin antibody 843 IU/mL (nL 0–80), thyroperoxidase antibody 130 IU/mL (nL 0–29), thyroid stimulating hormone receptor antibody 22.90 IU/L (nL<1.22), thyroid stimulating immunoglobulins 299 units (nL<140), erythrocyte sedimentation rate 120 mm/h (nL 0–20), and C-reactive protein 1.117 mg/dL (nL 0–0.5). Human leukocyte antigen (HLA) typing revealed DRB1, DR8, B35, B39, DQB1, DQ4, and DQ5. A thyroid ultrasound showed an enlarged heterogeneous gland with mild hypervascularity. Fine-needle aspiration (FNA) biopsies of both thyroid lobes revealed granulomatous thyroiditis. The thyroid scan showed a diffusely enlarged gland and heterogeneous trapping. There was a focal area of relatively increased radiotracer accumulation in the right upper pole. The 5-hour uptake (123I) was 6.6% (nL 4–15). The patient was symptomatically treated. Over the next several weeks, she developed hypothyroidism requiring levothyroxine treatment.
Summary:
This case illustrates a rare simultaneous occurrence of Graves' disease and SAT. Previous case studies have shown that Graves' disease may develop months to years after an episode of SAT. A strong family history of autoimmune thyroid disorders was noted in this patient. Genetic predilection was also shown by HLA typing.
Conclusion:
Although the occurrence of SAT with Graves' disease may be coincidental, SAT-induced autoimmune alteration may promote the development of Graves' disease in susceptible patients. Genetically mediated mechanisms, as seen in this patient by HLA typing and a strong family history, may also be involved.
Introduction
Patient Presentation
A 41-year-old Caucasian woman with no past history of thyroid disorders presented with 10 days of neck pain, as well as fatigue, sweating, subjective fever, chills, dysphagia, odynophagia, hand tremors, palpitations, hyperdefecation, irritability, moodiness, heat intolerance, nonproductive cough, and headaches. Neck pain had initially started at the base of the right anterior neck and gradually spread to her upper chest, the left side of her neck, and bilateral ears. Ibuprofen, 600 mg every 8 hours, was prescribed with an improvement of symptoms. She denied experiencing vision problems, weight changes, or lower extremity edema. Past medical history was only significant for seasonal allergies. Before this presentation, she had not taken any medications at home. She drank one beer with dinner and did not smoke. Family history was pertinent for her mother and sister with hypothyroidism and her father with hyperthyroidism at the age of 71 years. On physical examination, the patient had a heart rate of 110 beats/minute, blood pressure of 111/73 mmHg, weight of 125 lbs, and a body mass index of 22.9 kg/m2. She had mild bilateral fine hand tremors and warmth of the skin. There was no proptosis, lid lag, conjunctival redness, periorbital edema, or erythema. Her clinical activity score for Graves' opthalomopathy was 0. Her thyroid gland was enlarged to approximately 60 g without palpable nodules or lymphadenopathy. The left side of the anterior thyroid gland was tender to palpation. A cardiovascular examination showed regular tachycardia with normal S1, S2, without murmurs. Her lungs were clear to auscultation. A neurological exam showed brisk patellar reflexes. Laboratory examination revealed the following values (Table 1): erythrocyte sedimentation rate 120 mm/h (reference 0–20), high sensitivity C-reactive protein 1.117 mg/dL (reference 0–0.5), thyrotropin (TSH)<0.01 mcIU/mL (reference 0.39–5.33), serum free thyroxine (FT4) 2.0 ng/dL (reference 0.59–1.60), free triiodothyronine 6.6 pg/mL (reference 2.3–4.2), thyroglobulin 20.1 ng/mL (reference 2.0–35.0), thyroglobulin antibody 843 IU/mL (reference 0–80), thyroperoxidase antibody 130 IU/mL (reference 0–29), thyroid stimulating hormone receptor antibody (TSH-R Ab) 22.90 IU/L (reference<1.22), and thyroid stimulating immunoglobulins (TSIs) 299 units (reference<140). Complete blood count, renal panel, and liver function tests were within normal limit. Human leukocyte antigen (HLA) typing revealed DRB1, DR8, B35, B39, DQB1, DQ4, and DQ5. A thyroid ultrasound showed an enlarged heterogeneous hypoechoic thyroid gland with hypervascularity and without discrete nodules (Fig. 1). A fine-needle aspiration (FNA) of the hypoechoic areas in both lobes was performed to exclude intrathyroidal hemorrhage. The aspirate revealed numerous groups of follicular cells with features consistent with granulomatous (subacute) thyroiditis (Fig. 2). Thyroid scan showed a diffusely enlarged gland and heterogeneous trapping throughout with alternating areas of increased and decreased uptake. There was a focal area of relatively increased radiotracer accumulation in the right upper pole. Additionally, there was a visible pyramidal lobe emanating from the superior-medial aspect of the left lobe. A 5-hour uptake (123I) was 6.6% (normal 4%–15%; Fig. 3). Noncontrast computed tomography scan of the chest and frontal/lateral plain films of the chest were normal. The patient was prescribed atenolol and guaifenesin, and advised to continue ibuprofen for pain. Over the next several weeks, her symptoms resolved, and she developed hypothyroidism requiring levothyroxine treatment.

Thyroid ultrasound, transverse view, showing a diffusely heterogeneous gland with hypoechoic areas and without nodule identified. There is increased vascular flow noted bilaterally. Color images available online at

Fine-needle aspiration of thyroid gland showed numerous groups of follicular cells with features consistent with granulomatous (subacute) thyroiditis. Color images available online at
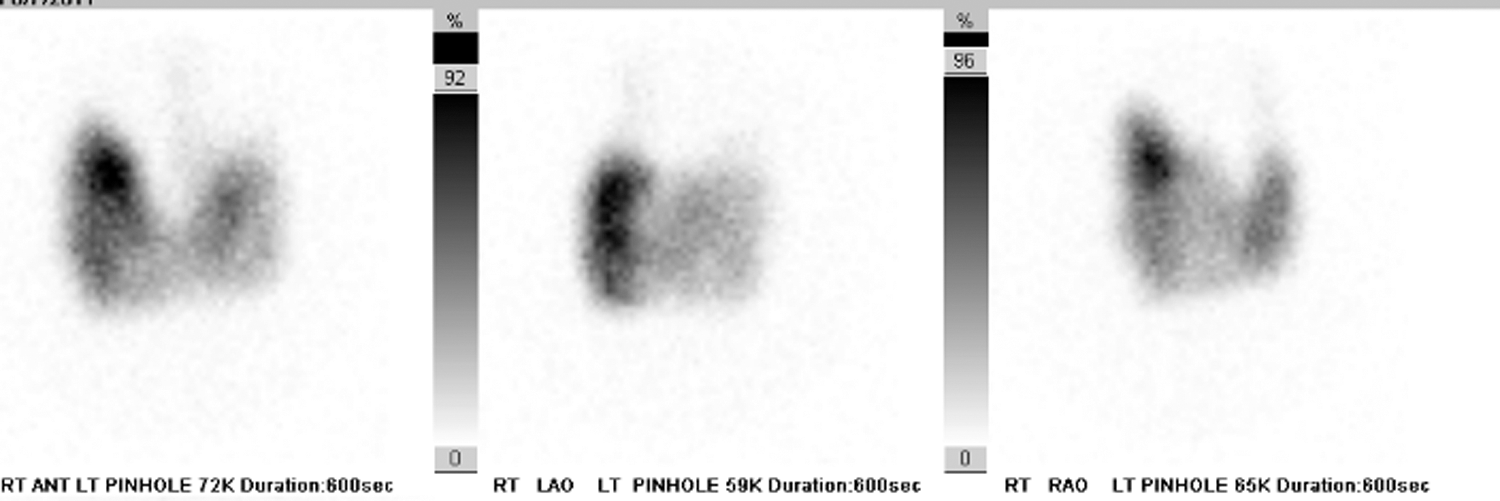
Thyroid scan showed a diffusely enlarged gland and heterogeneous trapping throughout with alternating areas of increased and decreased uptake. There was a focal area of relatively increased radiotracer accumulation in the right upper pole. Additionally, there was a pyramidal lobe emanating from the superior-medial aspect of the left lobe. A 5-hour uptake (123I) was 6.6% (normal 4%–15%).
Normal laboratory values are given in parentheses.
ESR, erythrocyte sedimentation rate; FT4, free thyroxine; TSH, thyrotropin; TT3, total triiodothyronine; TSI, thyroid stimulating immunoglobulin; TSH-RAb, thyroid stimulating hormone receptor antibody; TgAb, thyroglobulin antibody; TPO, thyroperoxidase antibody; Tg, thyroglobulin.
Discussion
SAT is a transient inflammatory thyroid disorder that is characterized by painful goiter with hyperthyroidism and laboratory evidence of systemic inflammation. In most cases, patients will completely recover; <1% may become hypothyroid (2). Previous reports have described Graves' disease occurring after SAT (1,3 –7) and found that the interval between the onset of thyroiditis and the diagnosis of Graves' disease varied from 4 months to 8 years. These reports suggested various mechanisms leading to Graves' disease after SAT, such as stress of SAT on the immune system in predisposed patients, release or expression of autoantigens in susceptible patients, and/or genetic susceptibility to the disease.
Our patient had no previous exposure or risk factors that may have predisposed her to thyroiditis, such as radioactive iodine, immunosuppressive therapy, recent neck manipulation from parathyroid or cervical surgery, or neck radiotherapy. Consistent with SAT, she presented with neck pain, laboratory evidence of systemic inflammation, and thyrotoxicosis. This diagnosis was further confirmed with the FNA biopsy result. In addition, initial laboratory data revealed high titers of TSI and TSH-R Ab, thus suggesting an underlying autoimmune Graves' disease. Radioactive iodine uptake of the thyroid is usually decreased in SAT; this finding is due to suppressed TSH, inflammation leading to destruction of thyroid follicles and/or, possibly, increased intra-thyroidal iodine content (8,9). The simultaneous presence of both SAT and Graves' disease at the initial presentation may explain why her thyroid uptake, particularly in the right upper lobe and pyramidal lobe, was well preserved, and not high as typically seen in Graves' disease or low as seen in SAT. The increased tissue vascularity visualized in the affected thyroid on color doppler ultrasound also supported the diagnosis of Graves' disease; whereas in SAT, the vascularity is usually markedly decreased (10). In the same manner, the relative preservation of thyroid uptake in this patient was probably due to the presence of circulating TSIs. The thyrotoxicosis possibly resulted from the release of thyroid hormone from destroyed thyroid tissue as well as increased synthesis of thyroid hormone as would be seen in Graves' disease. Although both mechanisms may be involved, the relative elevation in the initial serum free T3 concentration and normal 123I uptake further supported autonomous hypersecretion of thyroid hormones due to Graves' disease. Her symptoms of acute thyroiditis quickly resolved with nonsteroidal anti-inflammatory medication and without antithyroid medications. Despite the presence of Graves' disease, laboratory examination showed hypothyroidism 5–6 weeks after initial presentation, a disease course consistent with SAT. In this case, FNA biopsy of both lobes and RAI scan demonstrated that SAT was more diffuse than focal. The diffuse thyroiditis may have led to complete destruction and auto-ablation of the thyroid gland, which would explain the lack of clinical manifestations of Graves' disease.
The strong family history of autoimmune thyroid disorders supports a genetic predisposition in our patient. Mediated genetic susceptibility has been shown in both SAT and Graves' disease. A strong linkage between HLA-B35 and SAT has been found in all genetic groups (11 –13), whereas HLA-DRB1 and -DQB1 are consistently associated with Graves' disease (14 –16). The patient's analysis of HLA typing supports a genetic predilection for both Graves's disease (HLA-DRB1, DQB1) and SAT (HLA-B35). In addition to genetic susceptibility, the simultaneous occurrence of Graves' disease could also be due to autoimmunity induced either by SAT or a viral infection. Alternatively, the simultaneous presentation of these two disorders may be coincidental. So far, the paucity of longitudinal evaluations of TSI, TSH-R Abs antibodies, and nuclear imaging studies in these patients make it difficult to determine the prevalence of simultaneous thyroid autoimmunity and SAT, or the exact time of the transition from SAT to Graves' disease. The patient may have latent Graves' disease, which might become overt in the future (6,17).
Conclusion
This case illustrates a rare occurrence of simultaneous Graves' disease and SAT. Previous reports have shown the development of Graves' disease months to years after an episode of SAT. Although the occurrence of SAT with Graves' disease may be coincidental, SAT-induced autoimmune alteration may promote the development of Graves' disease in susceptible patients. Genetically mediated mechanisms may also be involved.
Disclaimers
The views expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Department of the Navy, Department of Defense, or the U.S. Government.
The authors certify that all individuals who qualify as authors have been listed; that each has participated in the conception and design of this work, the analysis of data, the writing of the document, and the approval of the submission of this version; that the document represents valid work; that if they used information derived from another source, then they had obtained all necessary approvals to use it and made appropriate acknowledgements in the document; and that each takes public responsibility for it.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.