
Abstract
Background:
Concern about potential harmful effects of early maternal hypothyroidism (MH) on fetal brain development has led to calls for universal screening early in, or even before, pregnancy. However, evidence in humans that adverse effects are irreversible if thyroid hormone replacement is initiated after the first trimester is limited. Severe MH due to thyrotropin (TSH) receptor blocking antibodies (Abs) is associated with profound cognitive delay in the offspring if MH is untreated or inadequately treated; here, we sought to determine the outcome if treatment is given in early pregnancy.
Methods:
We identified three women who had TSH receptor blocking Ab–induced MH during pregnancy and were treated with L-thyroxine (L-T4), starting at 27 weeks, 5 weeks, and the first month of gestation. The corresponding pretreatment serum TSH levels in the two women in whom data were available were 68 and 65 mU/L, falling to 6 mU/L at 25 and 24 weeks of gestation, respectively. The third woman with MH required 0.5 mg of L-T4 to normalize her thyroid hormone levels by 4 months of gestation. Their infants were also treated with L-T4 after neonatal screening that identified congenital hypothyroidism (CH). Neuropsychological tests to assess intelligence, language, memory, and visual-motor performance were administered to these three infants at 5.4 years of age (range 5.1–6.1) and to three sibling controls at 6.8 years (range 9.1–3.0).
Results:
Children born after MH had average or above average results on all parameters. Comparative scores of the neuropsychological tests in sibling pairs for full-scale intelligence quotient (IQ) and performance IQ were variable; some scores were higher and some were lower in CH children.
Conclusions:
Although the findings do not exclude a subtle impact of MH during early gestation on intellectual function, the normal cognitive outcome despite overt MH should provide data with which to counsel mothers who have overt hypothyroidism early in pregnancy. Aggressive thyroid hormone replacement as soon as possible is important, but early termination of the pregnancy because of fear that the baby will have significant cognitive delay is not warranted.
Introduction
This growing array of in vitro data has led to concern about possible adverse effects of early maternal hypothyroidism (MH) on the fetus and calls for universal screening of pregnant women early in pregnancy or even prior to pregnancy (9,10). In some cases, we are even aware of pregnant women found to be severely hypothyroid who considered early termination of pregnancy because of fear that their infant might have significant cognitive delay. Yet, evidence in humans that such adverse effects on fetal brain development are irreversible if thyroid hormone replacement is initiated after the first trimester and the precise window of time by which MH should be corrected remain unclear. In 1999, Haddow et al. showed that children born to untreated hypothyroid mothers had a 7-point deficit in their intelligence quotient (IQ) at 7–9 years of age as compared with similarly aged children born to matched women whose serum thyrotropin (TSH) levels were normal. In contrast, the IQ deficit was only 4 points, a difference that was not significant, when children of the entire group of hypothyroid mothers (both treated and untreated) were compared with controls (11). Although these results have been widely interpreted as supporting the need for diagnosis and therapy of MH early in pregnancy, these investigators only measured maternal TSH once at 17 weeks so it is also possible that therapy at some time later in gestation accounted for the reduced IQ deficit seen in the offspring of the treated subgroup of hypothyroid mothers.
As part of a large population survey, we previously identified nine children with transient TSH receptor blocking antibody (Ab)–induced congenital hypothyroidism (CH). In all babies, neonatal hypothyroidism had been identified and corrected soon after birth (12). In three of these children, MH was present in the early part of their gestation. The purposes of the present study were to comprehensively evaluate the cognitive development in the three children whose mothers had MH early in their gestation. As a control we performed similar studies in sibling pairs born after a gestation in which MH was not present.
Methods
The results of thyroid function testing performed during pregnancy were obtained retrospectively by interviewing the women's primary endocrinologist and reviewing thyroid function test results determined as part of their routine care. Not all data were available in all patients.
A battery of neuropsychological tests was administered to assess intelligence, language, memory, and visual-motor performance. All tests were performed by one of two experienced, pediatric clinical psychologists without knowledge of maternal thyroid function during pregnancy. In four of the six cases, the psychological evaluation was performed in the children's home. The study was approved by the University of Massachusetts Medical Center Committee for the Protection of Human Subjects in Research.
For children >7 years of age (n=2), the Wechsler Intelligence Scale for Children, third edition (WISC III), was selected since this was the most widely used intelligence test for children at the time the study was performed and utilizing it facilitated comparison with similar previous studies (13). For children >5–7 years of age (n=3), the Wechsler Preschool and Primary Scale of Intelligence Revised (WPPSI-R), a well-standardized test for younger children, adapted in part from the WISC III, was employed (14). One child was <5 years of age, and in her case, the McCarthy's Scales of Children's Abilities was used (15).
We employed the Story Memory Test (from Wide Range Assessment of Memory and Learning [WRAML]) to assess memory (16), and the Peabody Picture Vocabulary Test (17) and the Expressive One-Word Picture Vocabulary Test (18) to evaluate receptive and expressive vocabulary, respectively. To assess visual perception and fine motor skills, the Developmental Test of Visual-Motor Integration (19) was used. The Grooved Pegboard Test was administered to assess visual-motor co-ordination, fine motor skills, and dexterity (20). In this test, the time required (seconds) to insert pegs with the dominant and nondominant hand is recorded.
Results on all tests except the Grooved Pegboard Test were standardized for age. An average score on the WRAML Story Memory Test is 10±3 (mean±1 SD); on all other tests (except the Pegboard) an average score is 100±15 (mean±1 SD).
Results
Maternal thyroid function
Clinical information, including thyroid function tests, regarding the three hypothyroid mothers is summarized in Table 1. In one mother, overt hypothyroidism followed radioactive iodine therapy for severe Graves' disease whereas the other two mothers presented initially with overt hypothyroidism. In patients M-1 and M-3, MH was corrected before the end of the second trimester; in patient M-2, the free T4 concentration was normalized by the end of the first trimester but the TSH concentration remained slightly elevated throughout pregnancy. Three siblings were also evaluated. Sibling 1 was born prior to the recognition of maternal Graves' disease. Siblings 2 and 3 were born after pregnancies in which MH was controlled with 0.3 and 0.2 mg L-T4, respectively.
RAI for severe Graves' disease 4 months prior to conception. Hypothyroidism noted at 3rd week of gestation and treatment initiated. Required up to 0.45 mg L-T4 until 7 months of gestation for control of thyroid hormone levels.
Hypothyroidism, first diagnosed at 18 years of age, recurred at 5th week of gestation after prescription expired. Placed on L-T4 of 0.15 mg daily, with a gradual increase to 0.225 mg daily.
Severe hypothyroidism diagnosed at 1 month gestation. L-T4 dose progressively increased from 0.1 to 0.5 mg L-T4 with normalization of thyroid hormone levels at 4 months. Postpartum L-T4 discontinued; subsequent serum T4 concentration <1.3 μg/dL, TSH >638 mU/L.
RAI, radioactive iodine; TSH, thyrotropin; T4, thyroxine.
Neonatal thyroid function
The three children born to hypothyroid mothers had a definitive diagnosis of CH; this was diagnosed and treated within 15 days of birth (Table 2). In all babies, potent TSH receptor blocking Abs were detected on their neonatal blood filter papers and confirmed in their mothers. This information has been reported previously (12). One sibling (#1) had normal results on newborn thyroid screening, while the two other control siblings (#2 and #3) were born with CH that was adequately controlled postnatally.
Blocking activity was expressed either as % inhibition or quantitatively by comparison with a standard curve.
To convert to nM, multiply by 12.8717.
NB, newborn; DOL, day of life.
Tests of cognitive function
Results of verbal IQ, performance IQ, and full-scale IQ are shown in Figure 1 and in Table 3. Results in the other tests of language, memory, and visual-motor performance are also provided in Table 3. The average age at the time of testing of the children born after MH was 5.4 years (range 5.1–6.1) and that of their siblings was 6.8 years (range 3.0–9.1). One of the siblings was <5 years; in this latter child who was 3 years of age not all the tests were performed. Children born after MH had an average or above average result in all domains. Of interest, the child of mother M-2, who remained mildly hypothyroid despite the institution of treatment until the end of her pregnancy, scored less well than his sibling in all parameters (Table 3). Comparative scores of the neuropsychological tests in sibling pairs for full-scale IQ, verbal IQ, and performance IQ were variable; some scores were higher and some were lower in CH children compared with their normal sibling.
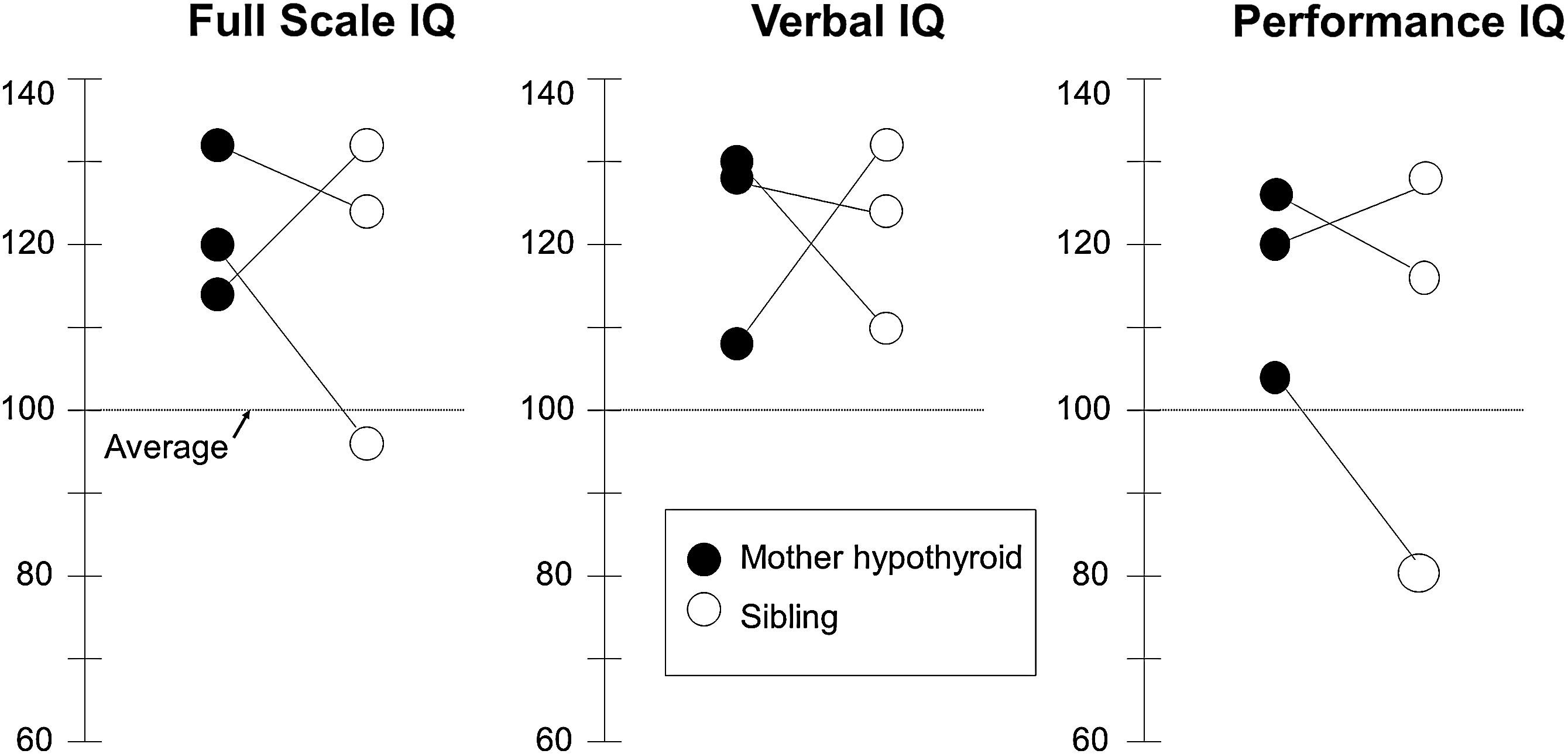
Full-scale intelligence quotient (IQ), verbal IQ, and performance IQ in children with thyrotropin receptor blocking antibody–induced congenital hypothyroidism born after maternal hypothyroidism (•) compared with their siblings (○). Sibling pairs are connected with a line. An average score is 100±15 (mean±SD). Note the average to above-average performance in all domains.
Average score is 100±15 (mean±1 SD).
Average score is 10±3.
Norms for Grooved Pegboard Test (seconds):
ND, not done; IQ, intelligence quotient; WRAML, Wide Range Assessment of Memory and Learning.
Discussion
Evidence for a potentially important role of maternal thyroid hormone in the first trimester of pregnancy prior to the onset of fetal thyroid action has led to widespread concern that babies born after early MH or even after early isolated maternal hypothyroxinemia will have significant permanent cognitive delay irrespective of later substitution therapy, yet there is a paucity of direct evidence in humans to support this concern. The three children born to hypothyroid mothers in this report are illuminating cases because their mother all had overt hypothyroidism in the first half of pregnancy. Indeed, of 2000 consecutive pregnant women in Maine studied by Klein et al., none had a serum TSH concentration as high as the women we studied (21). Similarly, only 1 of the 62 women with MH studied by Haddow et al. had a serum TSH concentration >60 mU/L (11). Although the small sample size in this study and its retrospective design provides limited ability to discern a small difference between the children of hypothyroid and euthyroid mothers statistically, our findings of an average to above average IQ should be reassuring as we are aware of several mothers who considered early termination of pregnancy when they were found to have severe hypothyroidism early in gestation. The present results suggest that prompt substitution therapy to normalize thyroid hormone levels as quickly as possible should be sufficient to ensure a normal fetal cognitive outcome and that more drastic measures are not indicated.
Since thyroid-hormone-dependent brain development occurs in a highly regulated, spatial- and temporal-specific manner (22,23), we cannot exclude the possibility that subtle deficits in other domains were present in association with MH (24). We did not measure attention, vision, or hearing, and so it is possible that our patients had small deficits in these areas. None of the patients had strabismus, however, and tests of visuomotor integration were normal. Similarly, it is unlikely that our patients had significant hearing deficits since thyroid-hormone-dependent cochlear development and auditory function develop predominantly later in human pregnancies (the first postnatal week in rodents, roughly equivalent to the third trimester of human pregnancy) (25). Nonetheless, future studies in our patients and similar patients will be important to determine school performance, attention, and executive functioning before we can conclude that the severe MH has no impact on working memory, planning, organization, flexibility, and other higher level cognitive functions that do not coalesce until age 11 years or later.
In the model of MH we studied, MH alone is present early in pregnancy whereas combined maternal and fetal hypothyroidism develops after the first half of gestation as transplacental passage of immunoglobulin G increases (26) and the fetal TSH receptor is expressed (27). One might have expected, therefore, a more pernicious effect of MH on fetal brain development than if only the maternal compartment was thyroid hormone deficient. Indeed, in a previous study from Japan, the mean IQ was only 67 in five children with TSH receptor blocking Ab–induced CH whose mothers were hypothyroid during pregnancy. This compares with the normal IQ [104] in the remaining 12 children whose mothers were rendered euthyroid with therapy (28). Consistent with our data, four of the five mothers received no treatment or inadequate therapy throughout gestation, while the fifth mother had discontinued therapy only in the third trimester.
Untreated CH causes severe cognitive defects in later life. Although our three children whose mothers were hypothyroid in early pregnancy were born with severe CH, their normal cognitive outcome is consistent with that in babies born with other forms of severe CH that are treated early and adequately and in whom maternal thyroid function is normal.
Our more detailed neurodevelopmental evaluation also supports and extends the findings of most previous studies in which the offspring of mothers with either maternal hypothyroxinemia or isolated MH was formally assessed. More than 30 years ago, Man et al. showed that the IQ of offspring of hypothyroxinemic women at 4 and 7 years of age was indistinguishable from controls as long as “adequate” thyroid hormone replacement was begun by 12–29 weeks (29,30). In 2003, Pop et al. compared 57 children born to mothers with hypothyroxinemia (defined as a serum T4 concentration <10th percentile associated with a normal TSH) and 58 controls. At the age of 2 years there was an 8-point deficit in mental development and a 10-point deficit in motor development in children after maternal hypothyroxinemia at 12 weeks of gestation but this difference disappeared if the free T4 concentration was normal at 24 and 32 weeks (31). Similarly, Liu et al. found no difference in IQ between eight children whose mothers had severe hypothyroidism secondary to autoimmune thyroiditis and six sibling controls. In these mothers, the mean serum TSH concentration was 106 mU/L in the first trimester of pregnancy but thyroid hormone levels were restored to normal by 13–28 weeks (32). Similar results have been obtained by Momotani et al. in five additional patients (33). Recently, a large, prospective, randomized, controlled trial failed to demonstrate a difference in IQ at 3 years of age in the offspring of treated versus untreated patients with early MH (34).
The commonest cause of thyroid dysfunction in pregnant women in North America is autoimmune thyroiditis. In contrast, iodine deficiency, like TSH receptor blocking Abs, affects both the fetal and maternal thyroid gland and would therefore be expected to have a more severe impact on brain development than a similar degree of MH alone. It is of interest and potential significance that most of the animal data demonstrating an effect of early MH employed either iodine deficiency or antithyroid medication as experimental models (4,35). Both of these paradigms affect maternal as well as fetal thyroid function. Results in humans have been variable. Consistent with our data, Cao et al. concluded that iodine replacement of pregnant women in an area of severe iodine deficiency up to the end of the second trimester was associated with a normal neurocognitive outcome (36). In contrast, more recently, Berbel et al. reported a significant decrease in neurobehavioral performance at 18 months in offspring whose mothers had isolated hypothyroxinemia associated with mild iodine deficiency at 12–14 gestational weeks but not at term (37). Since performance at 18 months is not a reliable indicator of future development, more long-term studies at an older age will be important to determine whether the deficit observed by these investigators will be sustained.
In conclusion, we report three children with average or above average intelligence, language, memory, and visual-motor performance despite severe MH early in gestation due to TSH receptor blocking Abs. Although further data are required to exclude a more subtle impact on cognitive function, the present findings, together with other studies in the medical literature, do not support widespread concern that affected infants whose mothers are treated after the first trimester of pregnancy will have significant intellectual delay as long as maternal thyroid function is normalized before the third trimester. Larger randomized control trials of patients with early MH are necessary to exclude a more subtle impact on neurocognitive function.
Footnotes
Acknowledgments
The authors are indebted to Dr. Susan Waisbren for critical assessment of the data, and Drs. Joseph Majzoub and Del Fisher for helpful review of the article. This work was supported by a grant from the Thyroid Research Advisory Council, Knoll Pharmaceuticals (now Abbott Laboratories).
Disclosure Statement
The authors have nothing to disclose.