
Abstract
Background:
Anaplastic transformation of differentiated thyroid carcinoma (DTC) is a rare event with a poor clinical outcome. It usually occurs in the primary site or in regional lymph nodes, but rarely in distant metastatic lesions.
Summary:
A 55-year-old woman with persistent pain in the left hip joint visited our hospital. She had a history of DTC that had been surgically removed 12 years earlier. Clinical images showed a tumorous mass in the left pelvis, indicative of bone metastasis. The patient underwent surgery to remove the tumor and remained stable until local recurrence was found 5 weeks after the surgery. The patient subsequently underwent radiation therapy; however, she died of respiratory failure due to lung metastases 2 months after the surgery for the recurrent lesion. The surgical specimens were diagnosed as anaplastic thyroid carcinoma, indicating that anaplastic transformation of thyroid follicular carcinoma occurred in the metastatic skeletal lesion. In addition, the patient had an unusually high white blood cell count throughout the course. Based on elevated serum granulocyte colony-stimulating factor (G-CSF) levels and positive immunostaining for G-CSF in the surgical specimens, the patient was diagnosed with paraneoplastic leukocytosis.
Conclusion:
To our knowledge, this is the first case of anaplastic transformation of DTC arising in a metastatic bone lesion described in the literature. In addition, the present case also exhibited severe leukocytosis accompanied by elevated serum G-CSF levels. Clinicians should be aware of the possibility of this occurring in their patients with DTC, as this development calls for a rapid change from observational follow-up to aggressive treatment.
Introduction
We herein present a very rare case of anaplastic transformation of metastatic follicular thyroid carcinoma in a metastatic skeletal lesion, which, to our knowledge, is the first case reported in the literature. The present case is also unique in that it was accompanied by paraneoplastic leukocytosis, which is known to herald a poor clinical outcome in a variety of cancers. Since anaplastic transformation forebodes an extremely poor prognosis, clinicians seeing patients with a history of DTC should be aware of this condition, because it often heralds a progressively deteriorating clinical course.
Patient
A 55-year-old woman was referred to our service with a 3-month history of left hip pain and gait disturbance. She had a history of thyroid cancer that had been treated with total thyroidectomy at the age of 43 years. She subsequently developed multiple skeletal metastases and underwent spinal cord decompression and posterior spinal fusion for a pathological fracture in the thoracic vertebrae at the age of 51 years. The surgical specimens were histologically diagnosed as well-differentiated follicular thyroid carcinoma with no findings suggestive of anaplastic transformation. Radioactive iodine (131I) therapy was administered thrice after the surgery.
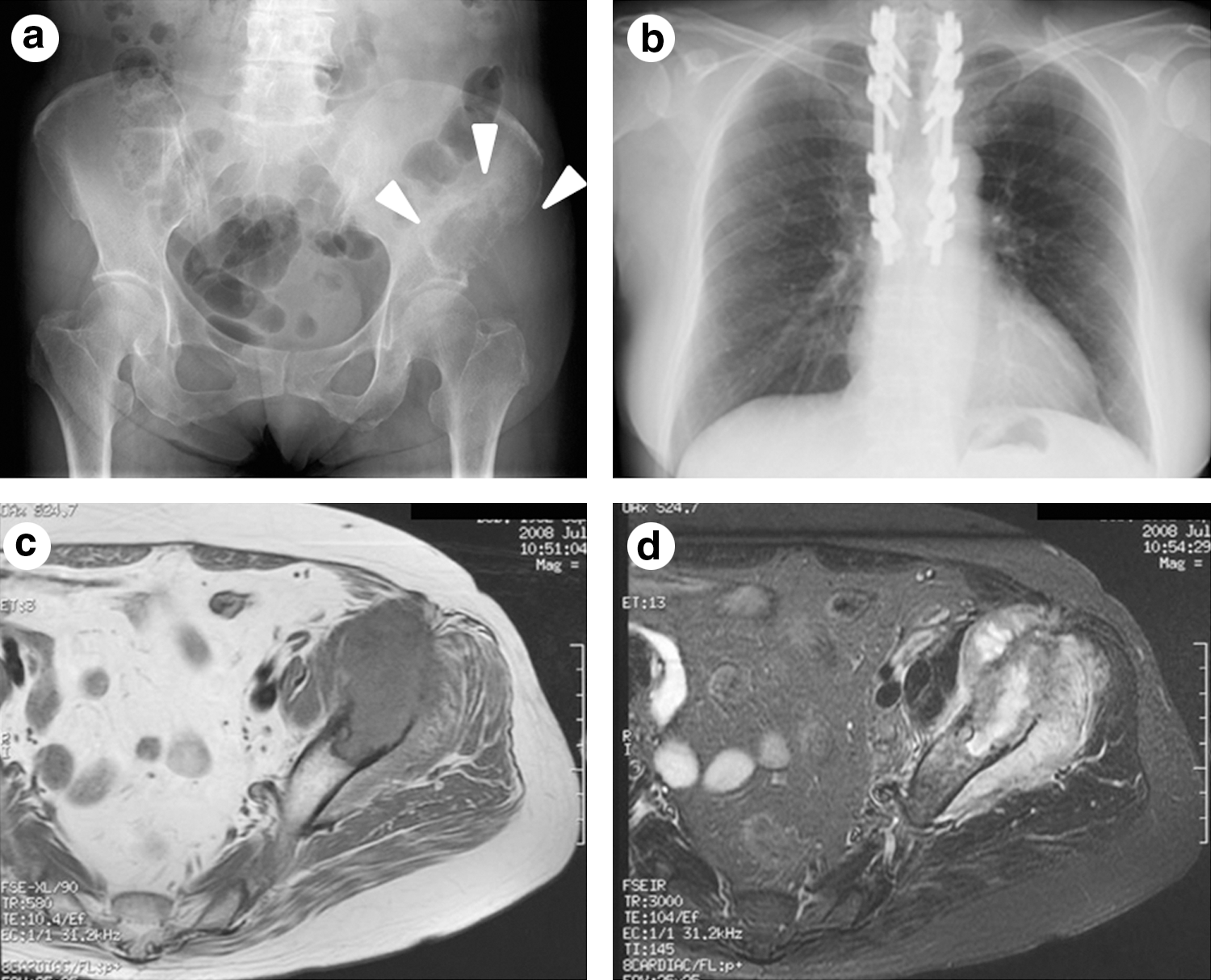
At presentation, X-rays of the pelvis revealed an osteolytic lesion in the left periacetabular region (Fig. 1a). Magnetic resonance imaging of the pelvis showed a bone tumor located in the left anterior inferior iliac spine extending to the superior ramus of the left pubis (Fig. 1c, d). The tumor was infiltrating into the surrounding soft tissue, and there was extensive edema around the lesion. Technetium99m bone scintigraphy showed strong uptake in the same region and faint accumulation in the skull, ribs, and spinal column. Chest X-ray showed no apparent metastatic nodules in the lung (Fig. 1b). In addition, there was a marked increase in the white blood cell (WBC) count (29,800/μL), despite the fact that the patient showed no sign of infection. To alleviate the pain and disability caused by the tumor in the hip, extensive curettage was performed. The postoperative course was uneventful, and she was discharged from the hospital two weeks after the surgery.
On gross observation, the tumor was tan-whitish in color with areas of extensive coagulative necrosis and infiltration into the surrounding soft tissues. Histological analysis revealed that the tumor cells were composed of anaplastic cells containing eosinophilic cytoplasm and hyperchromatic nuclei with prominent nucleoli. Follicular arrangements seen in the previous surgical specimens were totally lost. Moreover, an overt infiltration of neutrophils and lymphocytes was observed. Immunohistochemical analysis revealed that the tumor cells were positive for pankeratin (AE1/AE3) and vimentin and negative for thyroglobulin and thyroid transcription factor (TTF-1). The MIB-1 labeling index reached ∼10%. Based on these findings, a diagnosis of anaplastic transformation of DTC in the metastatic bone lesion was made (Fig. 2a, b).

The patient returned to our hospital with a complaint of worsening hip pain and swelling around the surgical wound site three weeks after her discharge. Pelvic computed tomography revealed an expanding mass with peripheral enhancement around the left acetabulum (Fig. 3a). Laboratory test results revealed a sharp increase in the WBC count (35,300/μL). Given these findings, infection at the surgical site was initially suspected, and emergency debridement was performed. However, there was no apparent abscess formation, but a tan-whitish necrotic mass reminiscent of the previous tumor. The bacterial culture showed negative results, and the surgical specimens were diagnosed as anaplastic carcinoma. At this point, the levels of hematopoietic cytokines in the serum were examined to investigate the cause of the increased granulopoiesis. The serum levels of granulocyte colony-stimulating factor (G-CSF) were highly upregulated (73.7 pg/mL; normal range, <18.1 pg/mL, intra-assay coefficient of variation; 2.75%–4.53%, interassay coefficient of variation; 10.4%–13.2%). In addition, immunostaining of the surgical specimens revealed positive staining for G-CSF (Fig. 2c). Since there were no findings indicative of infection, the patient was diagnosed with local recurrence and paraneoplastic leukocytosis caused by aberrant production of G-CSF from the tumor cells.
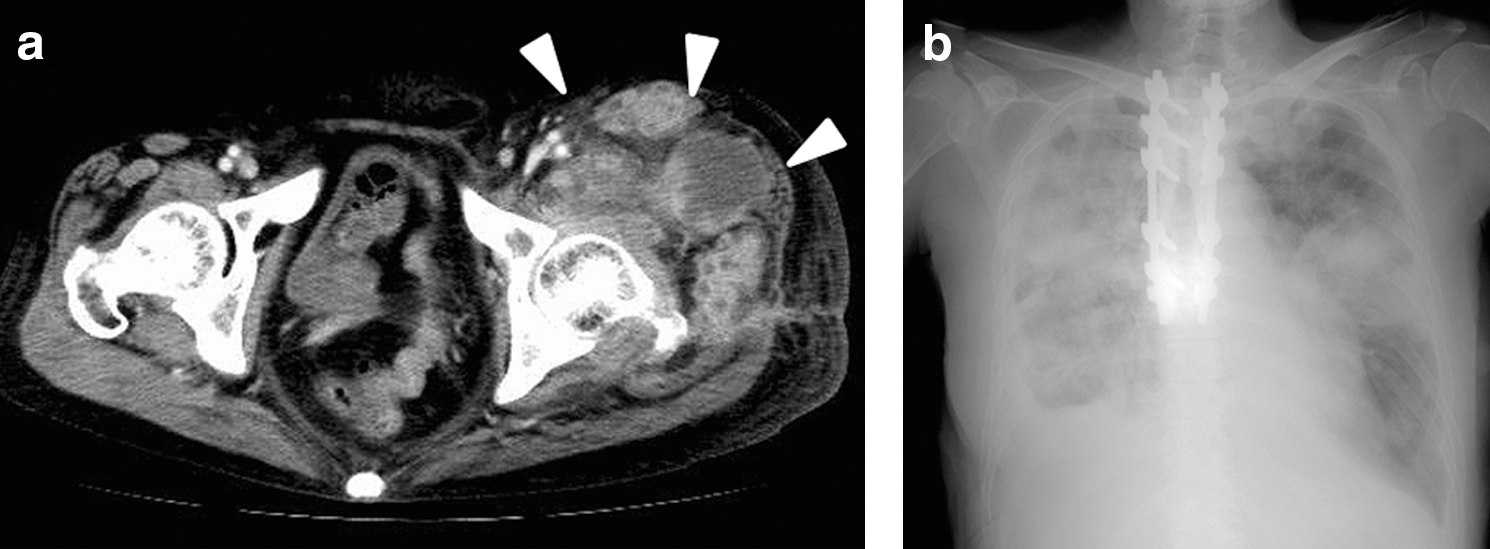
External beam radiation therapy at a dose of 50 Gy (25 fr) to the left pelvic region was subsequently initiated, and there was a temporal resolution in the symptoms and leukocytosis (Fig. 4). However, around the same time, the patient developed severe pleural effusion due to rapidly enlarging pulmonary tumors suspected to be metastases from the pelvic lesion (Fig. 3b). Her general condition deteriorated soon after, and she died 14 weeks after the initial pelvic surgery.
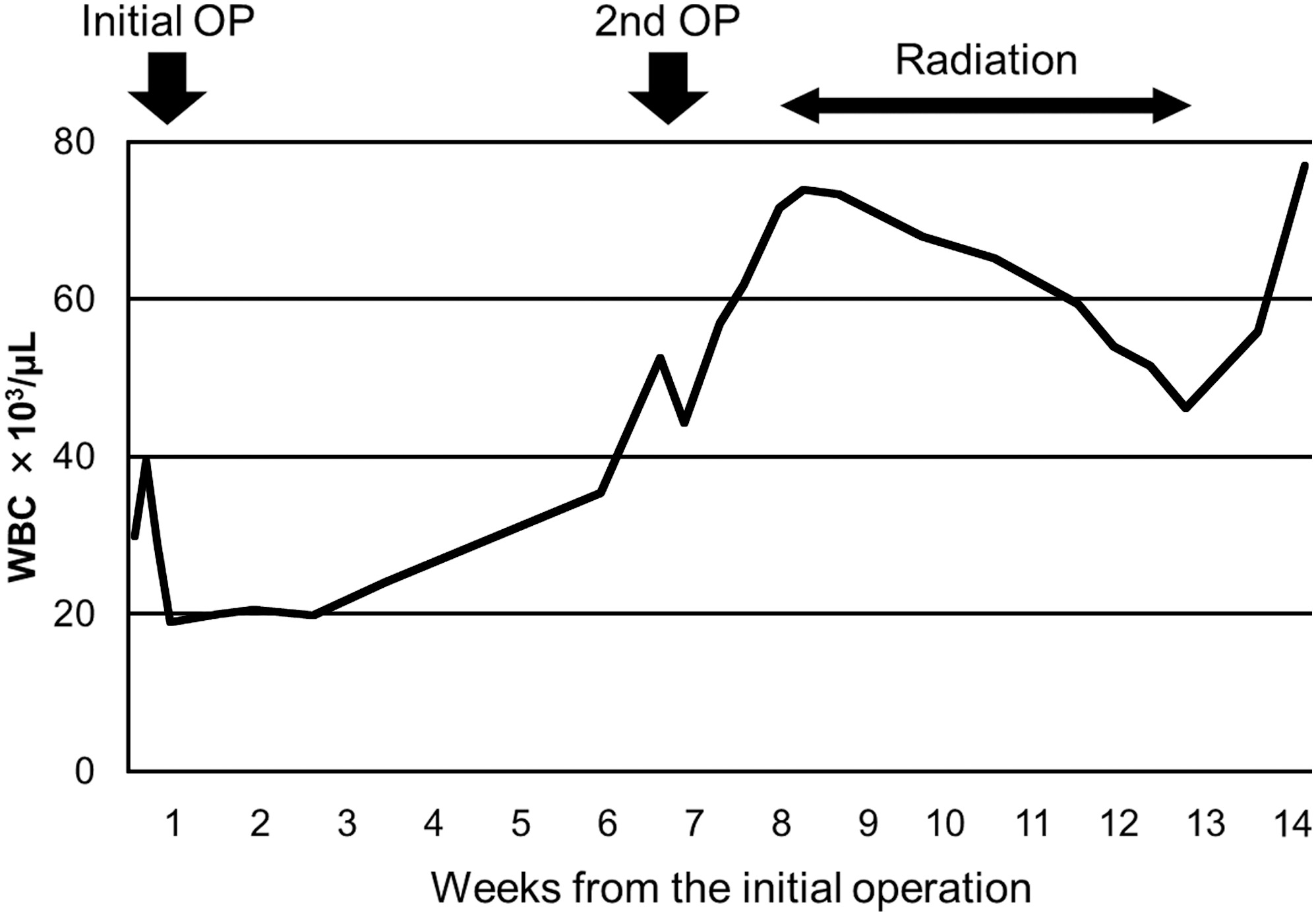
Time course of the WBC count during the clinical course. Temporal remission of leukocytosis was achieved after each treatment; however, the WBC count continuously rose throughout the course and reached 77,000/μL at the time of death. OP, operation; WBC, white blood cell.
Discussion
Anaplastic transformation of DTC is a rare event that usually occurs in the thyroid gland in situ or in surrounding cervical lymph nodes (8,13). To our knowledge, this is the first report that describes anaplastic transformation arising in a metastatic bone lesion.
Anaplastic transformation of DTC in distant extrathyroid sites is an uncommon event, and only a few case reports in the literature have described this condition (14 –18). In the present case, we concluded that the anaplastic transformation had occurred in the metastatic pelvic bone lesion in situ, but was not the result of metastatic dissemination of ATC to the bone for the following reasons: (i) in our patient, there was no metastatic lesion in the cervical lymph nodes, and the thyroid had been surgically removed 12 years before the onset of the pelvic lesion; (ii) the metastatic lesions in the lung and spine showed no significant change in size and remained clinically stable; and (iii) the tumor in the left pelvic bone was the first lesion that showed a rapid increase in size throughout the course.
Another important clinical feature of the present case is the involvement of paraneoplastic leukocytosis. Although we cannot rule out the possibility that the increase in G-CSF production was derived from inflammatory reaction and/or metastatic lesions other than the pelvic tumor, positive immunostaining for G-CSF in the pelvic tumor cells indicates the pelvic lesion as the major source of G-CSF in the present case. Paraneoplastic leukocytosis is often seen in patients with lung, gastrointestinal, genitourinary, or head and neck cancers (19 –22). This condition is manifested by an abnormally high WBC count often caused by aberrant production of hematopoietic cytokines, including granulocyte-macrophage CSF, G-CSF, interleukin 3, and interleukin 6, from the tumor cells (23 –27). Paraneoplastic leukocytosis rarely occurs in thyroid tumors, and there are only a few case reports in the literature (28 –35). Of note, this phenomenon is seen more frequently in patients with ATC than in those with DTC (35), indicating that aberrant production of cytokines tends to occur when the tumor cells undergo anaplastic transformation. Furthermore, in a multivariate analysis by Sugitani et al., leukocytosis (WBC count of >10,000/μL) was found to be an independent prognostic factor for patients with ATC in addition to the duration of complaints (<1 month), tumor size (>5 cm), and presence of distant metastatic lesions (36). However, their study did not clarify whether the leukocytosis was caused by abnormal production of hematopoietic cytokines from the tumor cells or derived secondary to the inflammatory reaction. Therefore, further studies are warranted to elucidate the cause of leukocytosis in patients with ATC and to determine how leukocytosis affects the biological behavior of the tumor.
In summary, we report a case of anaplastic transformation of follicular carcinoma in a metastatic skeletal lesion, which was accompanied by severe paraneoplastic leukocytosis. Although this event is not common, clinicians should be aware of the possibility of anaplastic transformation in metastatic foci, because occurrence of this event could drastically affect the treatment modality of patients diagnosed with DTC who would have been expected to have a relatively indolent clinical course and longer prognosis.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.