
Abstract
Background:
A combination of bilateral superficial cervical plexus block (BSCPB) and general anesthesia is recommended for thyroid surgery. Proof of the efficacy of this combination remains weak. Furthermore, data on the safety of this regimen are lacking. Therefore, a meta-analysis of randomized controlled trials (RCT) to evaluate the efficacy and safety of BSCPB as an adjunct to general anesthesia in patients receiving thyroid surgery was performed.
Methods:
A meta-analysis of RCT was performed that included interventional groups evaluating the efficacy of BSCPB 6 and 24 hours after thyroid surgery.
Results:
Eight RCT, including a total of 799 patients (463 who underwent BSCPB and 336 controls), were analyzed. A meta-analysis demonstrated a reduction in pain scores 6 hours (Hedges' g: −0.46 [95% CI: −0.74 to −0.19]; p=0.001) and 24 hours postoperatively (Hedges' g: −0.49 [95% CI: −0.71 to −0.27]; p<0.001) in patients who had undergone BSCPB. The relative risk for postoperative nausea and vomiting (PONV) was 0.80 (95% CI: 0.58 to 1.09, p=0.159) in patients receiving BSCPB. Procedure-related adverse events were reported in three of the 476 patients who had undergone BSCPB (0.6%; 95% CI: 0.1% to 2.0%). These three patients had transient paresis of the brachial plexus, combined with a diaphragmatic paresis in one case, and all spontaneously resolved.
Conclusion:
The combination of BSCPB and general anesthesia has a significant benefit in reducing pain 6 and 24 hours after thyroid surgery. However, the effect on pain reduction is too small to be of clinical relevance. Although it is a safe procedure, the existing evidence allows for no recommendation concerning the application of BSCPB in thyroid surgery. Further trials should evaluate a dose-response relationship and the incidence of PONV with this regimen.
Introduction
During the past decade, several randomized controlled trials (RCT) investigated the effect of cervical block together with general anesthesia on pain. The reported effects are quite inconsistent. Some trials could not find any beneficial effect (4,5). In contrast, other studies have shown a significant decrease in postoperative pain associated with the use of BSCPB (6,7). In one trial, the positive effect of the BSCPB was limited to the first few hours postoperatively (8). Another trial concluded that the combination of BSCPB and general anesthesia had a positive effect on postoperative pain for a period of 4 days after the surgery (9). In summary, evidence for the efficacy of BSCPB remains weak. Furthermore, the risk of PONV after thyroid surgery is high, with ∼50% of the patients affected (10). Reports of the effect of BSCPB on PONV are also controversial. While Suh et al. reported a significant decrease in PONV in patients who received BSCPB (11), other RCTs did not find such an effect (5,8).
The present study evaluated the efficacy and the safety of BSCPB when used as an adjunct to general anesthesia in patients undergoing thyroid surgery by performing a meta-analysis of the evidence available from RCT.
Methods
This meta-analysis was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (12).
Literature search
Relevant studies and reviews were identified by searching the Medline and Cochrane Library databases. The search was performed in December 2010. It was restricted to publications in English. The following search terms were used: (“thyroidectomy” [MeSH] OR “thyroid neoplasms” [MeSH] OR “thyroid gland” [MeSH] OR “thyroid dysgenesis” [MeSH] OR “thyroid nodule” [MeSH] OR “thyroid diseases” [MeSH]) AND (“nerve block” [MeSH] OR “cervical plexus” [MeSH]) OR ((“thyroidectomy” OR “thyroid”) AND (“superficial” AND “cervical” AND “block”)). Two investigators (R.W. and U.B.) independently performed the literature search. To broaden the search criteria, the “related article” function was applied. Articles referenced in the publications retrieved were also reviewed to identify additional relevant studies for potential inclusion.
Selection criteria
Only RCTs with at least one interventional arm receiving BSCPB in combination with general anesthesia for thyroid surgery were selected. Studies were included only if they provided information about at least one of the outcome measures defined next. Studies or treatment arms evaluating BSCPB without general anesthesia were excluded, as were studies or treatment arms combining BSCPB with a deep cervical plexus block. Studies or treatment arms assessing a wound infiltration with a local anesthesia were also excluded. Each trial was critically appraised by two investigators (R.W. and U.B.). The data were extracted independently by the same two reviewers and crosschecked.
Outcomes data extraction
Outcomes were analyzed on an intention-to-treat basis. Any discrepancies between the two reviewers were resolved by discussion. The patient's pain intensity was measured with self-reported pain scales reaching from the absence of pain to the most intense pain imaginable. On a visual analog scale (VAS) the patients specify their pain intensity by marking a position on a 10 cm long line. The distance from the left end in cm represents the score. While the patient can mark any position on a VAS (continuous data), on a numeric rating scale (NRS), the patient has to select one out of 11 options (0–10) (ordinal data). Both scales were considered equivalent for this study. Pain at 6 and 24 hours postoperatively were defined as the main outcome measures. These two time points were chosen, because most studies reported the data, and the patients were most likely awake for pain assessment, as thyroid surgery is usually performed during regular working hours. In cases where pain was not assessed at 6 hours postoperatively, data were calculated by linear interpolation based on the assessment of pain at 4 and 8 hours postoperatively. If data were not available from the text or tables, they were measured from the published figures. For trials that did not report the mean and standard deviation for the primary outcome measurement (5,7,8,13), the corresponding authors were contacted by e-mail, and the original data were requested. Raw data were available from one trial (9) that did not report the mean and standard deviation of the primary outcome. To assess the safety of the combined procedure, we evaluated the procedure-related adverse events (AEs) described in each RCT. The incidence of PONV was defined as a secondary outcome measure. The occurrence of PONV was recorded (yes vs. no) independent of its severity or treatment.
Quality assessment
The quality of reporting was assessed by two validated scores (14 –16). The Jadad score assesses the study design and reporting quality of a clinical trial using three items (blinding, randomization, and description of withdrawals and dropouts). The range of possible scores is 0 (poor) to 5 (good) (15). The Consort score assesses the quality of a clinical trial using a 25-item scale based on the Consort Statement. The range of possible scores is 0 (poor) to 25 (good) (16). Assessment was performed independently by two reviewers (U.B. and V.P.). Discrepancies were resolved by consensus in the presence of a third investigator (T.S.). The scores were not used to decide whether or not the trials would be included in the analysis.
Statistical analysis
Statistical analysis was performed using SAS version 9.1 (SAS Institute, Cary, NC.) and the R environment version 2.10.1 (
In trials with more than one intervention group, multiple treatment groups were combined to create single pair-wise comparisons as recommended by the Handbook of the Cochrane Collaboration (18). In the primary analysis, data were pooled using a random-effects model to adjust for possible variations in the treatment effect between the studies as described by DerSimonian and Laird (19). A sensitivity analysis and additional fixed-effect models were conducted. Statistical heterogeneity was quantified using I 2 and assessed by visual examination of the forest plot (20). Furthermore, heterogeneity was formally tested with Cochran's Q statistic (21). A funnel plot was used to examine the possibility of publication bias. Triangular regions were plotted in the funnel plot; 95% of the studies would be expected to fall in these regions under a fixed-effects model in the absence of biases or heterogeneity. A rank correlation test of funnel plot asymmetry was applied (22).
To assess statistical heterogeneity, fixed-effect meta-regressions were performed on the treatment arm level rather than on the study level and pooled for 6 and 24 hours postoperatively as sensitivity analyses. Shared control groups were divided out evenly among the comparison groups (18). The influence of two- versus three-point BSCPB, pre- versus postoperative administration of BSCPB, the use of ropivacaine versus bupivacaine, the amount of local anesthetics used in BSCPB, and placebo versus observation in the control group were analyzed to determine the efficacy of the BSCPB.
Results
Study selection and data extraction
Figure 1 summarizes the process of trial identification, inclusion, and exclusion. The initial search identified 69 studies. After screening, nine prospective trials were identified. One of these trials was then excluded, as the BSCPB was applied only in combination with a deep cervical plexus block (23). Finally, eight RCT including 799 patients undergoing thyroid surgery were eligible for analysis (4 –9,11,13). A total of 463 patients received BSCPB in combination with general anesthesia, whereas 336 patients received only general anesthesia (control group). Table 1 summarizes the interventions in the identified trials. Quality of reporting was high (six of eight studies had a Jadad score>3). However, none of the studies reported all 25 items of the Consort statement checklist (Table 2).
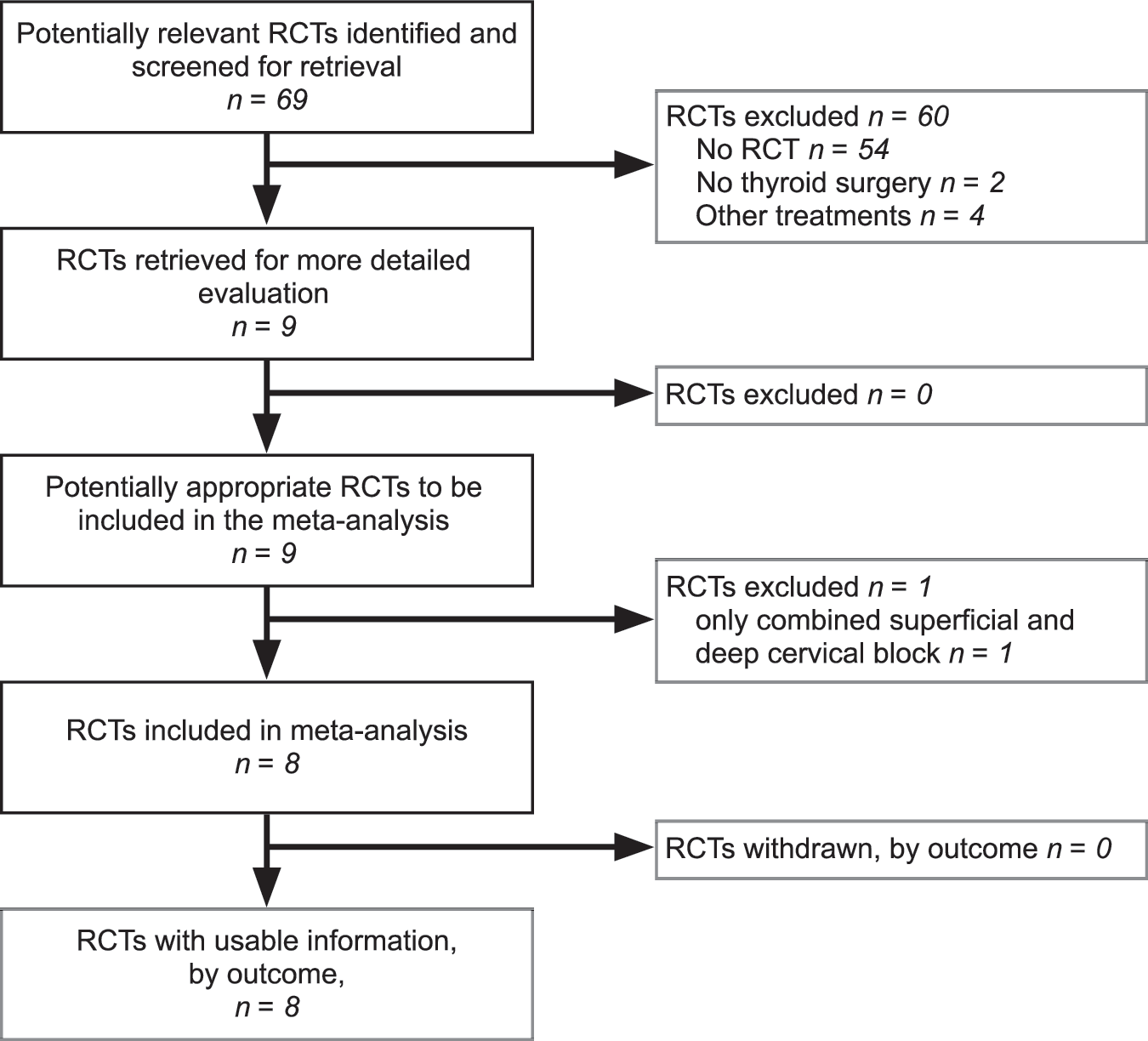
PRISMA flow chart for data inclusion.
The Jadad score (15) assesses the design and reporting quality of a clinical trial in regard to blinding, randomization, and description of withdrawals and dropouts.
The Consort score (16) assesses the quality of a clinical trial based on the 25 items of the Consort statement.
Number of patients considered in meta-analysis.
Outcomes data extraction
All eight trials reported postoperative pain using rating scores. Four studies (5,8,11,13) reported pain using NRS (11 steps from 0 to 10). The other four studies (4,6,7,9) used VAS scores. Pain 6 hours after surgery was reported by six studies, and pain at 24 hours was reported by all eight studies. For the two trials (5,7) not reporting pain after 6 hours, the pain scores were calculated from the scores assessed at 4 and 8 hours postoperatively. In five studies, the pain scores had to be extracted from figures, whereas three studies provided the pain scores in the text or in tables and one provided the raw data. Table 3 summarizes the extracted data regarding postoperative pain.
Extracted raw values are expressed as mean±standard deviation, median [25th–75th percentile], or median {10th–90th percentile}.
NRS, numeric rating scale with range; VAS, visual analogue scale with range.
Primary outcome analysis
Six hours postoperatively, pain was significantly less in patients who had undergone BSCPB compared with that in controls (Fig. 2). The SMD in the random-effects model (primary analysis) was −0.46 (95% CI: −0.74 to −0.19, p=0.001). The fixed-effect model, performed as a sensitivity analysis, yielded similar results. The forest plot, the I 2 value, and the Cochran's Q statistic indicated considerable statistical heterogeneity (24). Neither the funnel plot itself (not shown) nor the rank correlation test of funnel plot asymmetry (p=0.805) revealed evidence of publication bias.
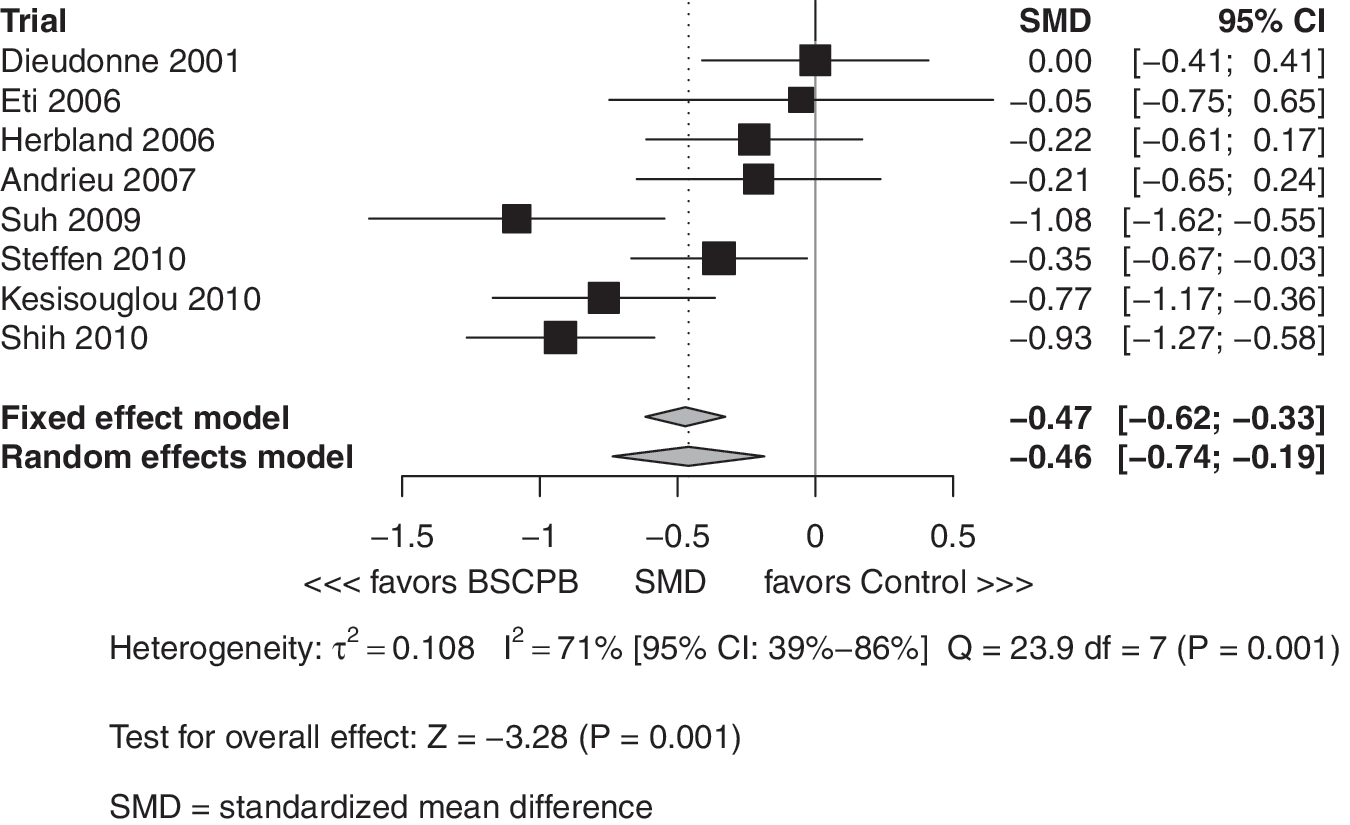
Meta-analysis of pain intensity scores 6 hours postoperatively: aggregated treatment arms.
Twenty-four hours postoperatively, the pain scores were again significantly lower in patients who had undergone BSCPB compared with that in controls (Fig. 3). The SMD in the random-effects model was −0.49 (95% CI: −0.71 to −0.27, p<0.001). The fixed-effect model confirmed the results of the primary analysis. The forest plot, I 2, and Cochran's Q statistic indicated considerable statistical heterogeneity (24). The funnel plot (Fig. 4) revealed a tendency for left-sided asymmetry, indicating a lack of smaller studies with significant results; this tendency was not significant as evaluated by the rank correlation test (p=0.216).
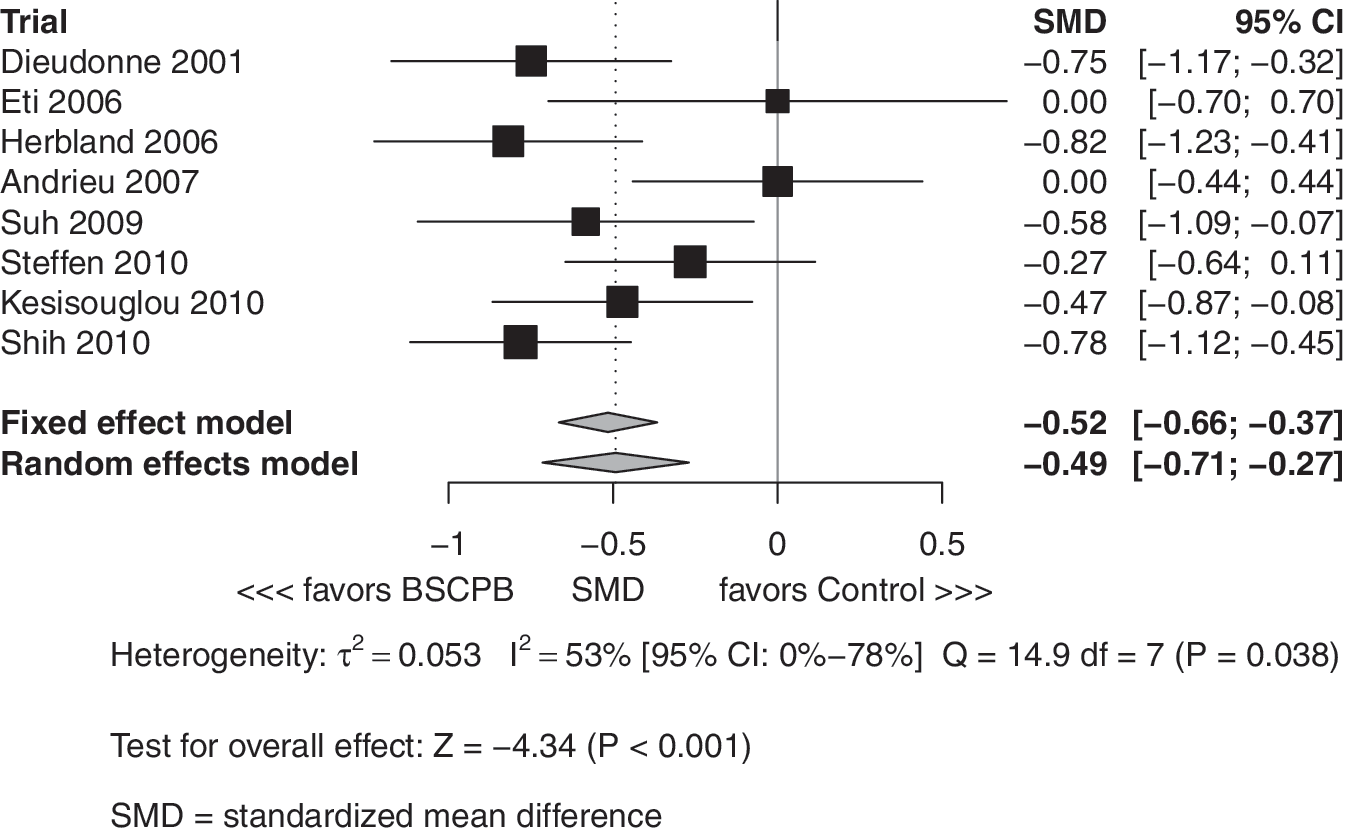
Meta-analysis of pain intensity scores 24 hours postoperatively: aggregated treatment arms.
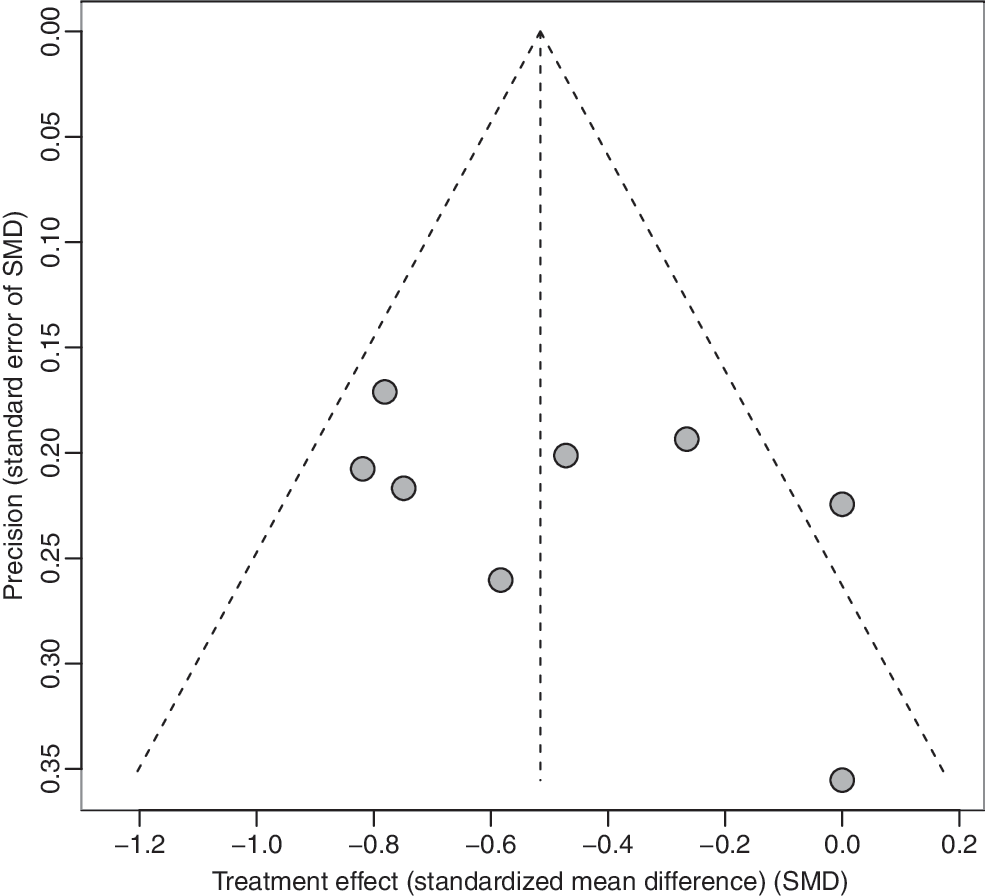
Funnel plot to explore potential publication bias for pain scores 24 hours postoperatively. Effect estimates of individual studies (standardized mean difference [SMD]) are scattered against the precision of the studies (standard error of SMD).
Analysis of heterogeneity
After applying a fixed-effect meta-regression at the study arm level and pooling the results of 6 and 24 hours postoperatively, the amount of local anesthetics used for the BSCPB significantly correlated with the efficacy of the BSCPB (p=0.024). For every 50 mg of local anesthetic used, the SMD decreased by 0.19 (95% CI: 0.03 to 0.34). The efficacy of the BSCPB did not differ significantly whether assessed after 6 versus 24 hours (SMD: 0.07; 95% CI: −0.18 to 0.31; p=0.560). Performing a two- versus three-point BSCPB (SMD: 0.21; 95% CI: −0.11 to 0.54; p=0.189), administering BSCPB pre- versus postoperatively (SMD: 0.03; 95% CI: −0.23 to 0.29; p=0.802), using bupivacaine versus ropivacaine (SMD: −0.02; 95% CI: −0.21 to 0.25; p=0.860), and using a placebo versus observation in the control group (SMD: −0.03; 95% CI: −0.29 to 0.23; p=0.831) did not significantly affect the observed efficacy of the BSCPB.
Secondary outcome analysis
Six RCT, including a total of 537 patients (330 patients with BSCPB and 207 patients without BSCPB), were eligible for analysis of PONV. The prevalence of PONV varied from 21.7% to 63.3%. While BSCPB reduced the RR for PONV by more than 20% in the meta-analysis, this reduction failed to reach statistical significance (Fig. 5). The RR in the random-effects model was 0.80 (95% CI: 0.58 to 1.09; p=0.159). The forest plot, the amount of I 2, and the Cochran's Q statistic indicated low-to-moderate heterogeneity (24). The funnel plot indicated the presence of missing studies with low precision and results favoring the BSCPB (not shown), whereas the rank correlation test did not show evidence of a publication bias (p=0.188).
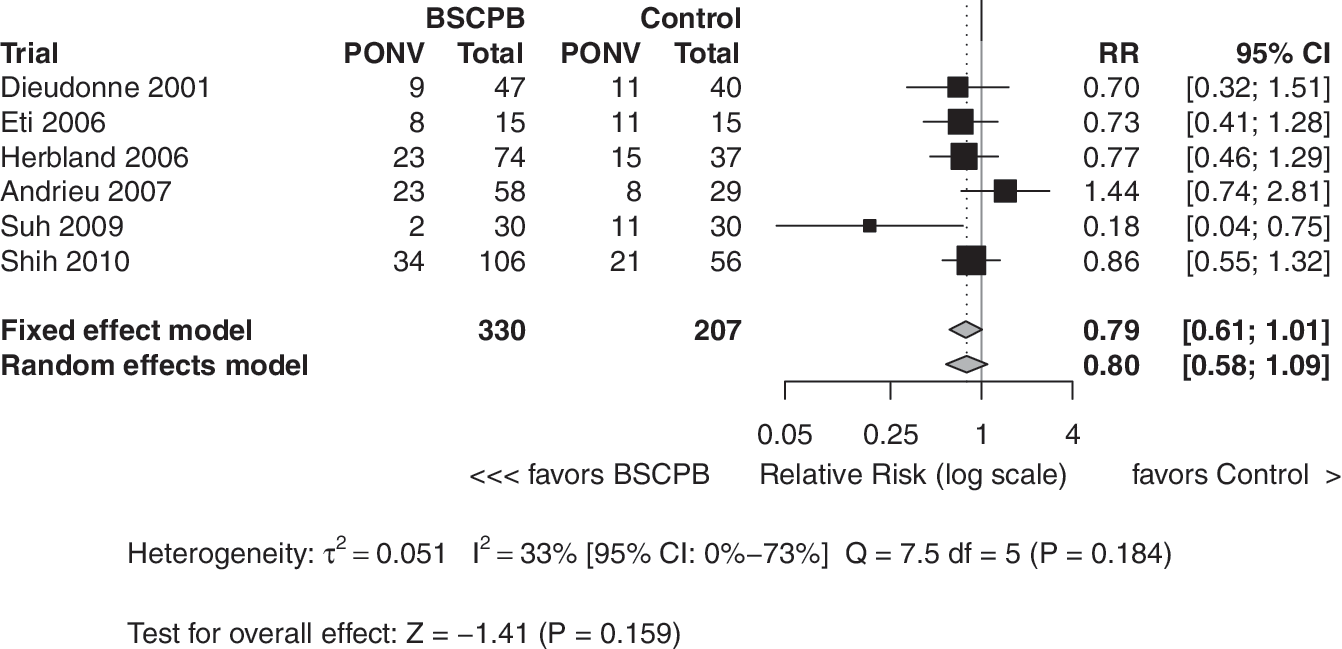
Meta-analysis of the relative risk of postoperative nausea and vomiting (PONV).
Safety analysis
AEs after BSCPB were reported in two of the eight included trials. Herbland et al. reported on one patient with a left brachial plexus paralysis and another patient with a partial motor block in the right arm after BSCPB. The AE completely resolved after 2 and 4 hours, respectively without any special therapeutic measures (5). Shih et al. reported that one thin female patient experienced a transient diaphragmatic paresis and a brachial plexus block after BSCPB; this AE was likely related to a deeper than intended injection of the BSCPB. The AE resolved completely after 6 hours without any treatment (7). Steffen et al. described a temporary numbness in the earlobe lasting for a few hours in about half of the patients with a cervical block; however, numbness resolved in all cases without consequences (9). Andrieu et al. reported a prevalence of transient vocal cord paresis diagnosed immediately after surgery by direct laryngoscopy in 4 of 29 patients (14%) in the placebo group and in 10 of the 58 patients (17%) who had undergone BSCPB (p=0.680)(8). Transient vocal cord paresis occurred in 8 of 29 (28%) of patients receiving BSCPB with clonidine as an adjunct to the BSCPB in contrast to 2 of 29 (7%) patients with BSCPB performed only with ropivacaine. In summary, relevant procedure-related AE were reported in three of 463 patients receiving BSCPB with local anesthetics, which amounts to a prevalence of 0.6% (95% CI: 0.1–2.0%). No serious adverse events were reported.
Discussion
Although this meta-analysis of eight RCT identified a significant benefit of BSCPB in pain reduction 6 and 24 hours after thyroid surgery, the observed pain reduction was not clinically relevant. Among potentially influencing factors, the amount of the local anesthetic administered in BSCPB was the only factor significantly influencing the treatment effect identified in the sensitivity analysis. In the secondary outcome analysis, which included six trials providing the necessary data, the meta-analysis failed to demonstrate a statistically significant decrease in the incidence of PONV with BSCPB. The prevalence of BSCPB-related AE was as low as 0.6%.
At the authors' institution, BSCPB is routinely performed (9). The clinical impression of a substantial benefit for the patient could not be confirmed by this meta-analysis. The treatment effect of BSCPB 6 hours postoperatively, estimated as the SMD, was only −0.46. Therefore, the application of BSCPB would reduce the mean VAS pain score in untreated controls from 3.4±2.0 (range 0–10) 6 hours postoperatively to a mean VAS score of 2.5. This finding might be explained by the statistically heterogeneous treatment effect of BSCPB, corresponding to the diversity in the design of the included trials. Specifically, the trials included BSCPB performed with two- and three-point injections; pre- or postoperatively; and with bupivacaine, ropivacaine, or levobupivacaine in different amounts, volumes, and concentrations. Furthermore, BSCPB was compared with no treatment in some trials and placebo in others.
Two different methods were used to block the main emerging branches of the superficial cervical plexus. The two-injection method involves applying local anesthesia in the caudal and cranial direction along the posterior border of the sternocleidomastoid muscle (5,6). The three-injection BSCPB method also includes a third subcutaneous transverse injection to block the transverse cervical branches (4,7 –9,11,13). In a sensitivity analysis, no significant difference in pain scores was identified between the two- and three-injection methods. Furthermore, preoperative versus postoperative administration of the BSCPB had no significant effect on its efficacy. The use of bupivacaine versus ropivacaine also had no significant impact on the BSCPB's efficacy. Although one would expect the contrary (25,26), the observed efficacy of the BSCPB was not significantly affected by using a no-treatment versus a placebo group as a control. From trials assessing the efficacy of wound infiltration with local anesthetics, a significant dose-response relationship is known to exist, with an increasing beneficial effect with higher concentrations of local anesthetics (27 –30). Eti et al. used 0.25% bupivacaine for the BSCPB and failed to demonstrate a clinically relevant effect, citing the low concentration of the local anesthetic as the reason for their negative finding (4). This assumption is supported by the present meta-analysis. Although only assessed in a sensitivity analysis, an increased amount of the administered local anesthetic for the BSCPB was associated with an enhanced treatment effect. Further studies should assess this dose-response relationship to determine the optimal dose of local anesthetic solution for the BSCPB.
Thyroid surgery is associated with a high prevalence of PONV, affecting up to 50% of patients (10). PONV is associated with the use of postoperative opioids and volatile anesthetics (31). The prevalence of PONV varied between 21.7% and 63.3% in the present meta-analysis. Although BSCPB was associated with a decrease in PONV, this effect was not statistically significant. The lack of significance may well be explained by the low power in the present meta-analysis. Therefore, we need further trials to assess the prevalence of PONV after thyroid surgery and the relationship between PONV and the use of a BSCPB.
All trials included in this meta-analysis were longitudinal studies with multiple time points for pain assessment, from 24 hours to 4 days postoperatively. While recent meta-analytic techniques are available for correlations between treatment effects in longitudinal studies, the authors opted against using such sophisticated modeling techniques, because the true values of the necessary parameters are not known and, therefore, no confirmation of better estimates exists (32). In contrast, the present meta-analysis was performed at two distinct time points using standard meta-analytic models. Evaluating the efficacy of the BSCPB at 6 and 24 hours postoperatively typically avoids surveying patients during the night hours. The reliability of pain scores assessed when waking up a patient two or three times a night to ask for a number on a pain scale seemed questionable. Furthermore, choosing these two distinct time points can account for the circadian variation in pain perception with lower intensity during the daytime (33 –35).
BSCPB-related AE, including partial brachial plexus and phrenic nerve blocks, have already been described (36). From the eight trials included in this meta-analysis, such AE occurred in three out of 463 patients. All AE resolved completely without the need for special treatment. Apart from these BSCPB-related AE, one study described a temporary numbness of the earlobe lasting for a few hours in about half of the patients who had undergone BSCPB, which was not considered a complication but rather a part of the treatment effect. Interestingly, in the study performed by Andrieu et al. (8), the prevalence of transient vocal cord paresis was much higher when performing the BSCPB with clonidine as an adjunct to ropivacaine. It can be hypothesized that with this adjunct the local concentration is higher and this might lead to the higher prevalence of transient vocal cord paresis by diffusion. Recurrent laryngeal nerve dysfunction is not uncommon in thyroid surgery, occurring from<1% to 20% of the time, depending on various factors (37,38) Therefore, a transient vocal cord paresis was not considered a BSCPB-specific AE.
Conclusion
Although this meta-analysis identified a significant effect of BSCPB in reducing postoperative pain after thyroid surgery this effect is of doubtful clinical relevance concerning pain reduction. With the presently existing evidence, a general recommendation concerning the application of BSCPB as an adjunct to general anesthesia in thyroid surgery cannot be made. Future trials should focus on finding a dose-dependent relationship. Furthermore, a possible benefit of BSCPB on PONV should be addressed.
Footnotes
Acknowledgments
The authors thank Dr. Verena Pioch for independently assessing the quality of the included trials.
Disclosure Statement
The authors declare that no competing financial interests exist.