
Abstract
Background:
Many studies on thyroid follicular tumors have reported the presence of somatic mutations to three forms of RAS: HRAS, KRAS, and NRAS. However, the frequency and clinical significance of these RAS mutations remain unclear, in large part due to the different methodologies being used for mutation analysis and the limited number of cases featured in studies. To clarify the significance of RAS mutations, we examined a large number of follicular adenomas and carcinomas obtained from a single institute using established methods for the analysis of RAS.
Methods:
Tumor samples from 40 follicular adenoma and 58 follicular carcinoma patients treated at the Kanagawa Cancer Center Hospital were analyzed. The three RAS mutations at codons 12 and 61 were assessed with a polymerase chain reaction–based loop-hybrid mobility shift assay followed by confirmation with direct sequencing. The relationships between mutation status and clinicopathological features at the time of the initial operation and the prognosis of the patients were also analyzed.
Results:
Twelve out of 40 (30%) adenomas harbored RAS mutations. In contrast, 33 out of 58 (57%) follicular carcinomas harbored RAS mutations, and the mutation was predominantly found in the NRAS codon 61 (22/33, 67%, p<0.01). The rate of gene mutations was significantly higher in the carcinomas than in the adenomas (p<0.01). The NRAS codon 61 mutation in follicular carcinomas was positively associated with distant metastases through the entire clinical course of the patients (p<0.05), and RAS mutations were associated with poor overall patient survival (p<0.05).
Conclusions:
We investigated the frequency of RAS mutations in follicular thyroid tumors from a large number of cases obtained from a single institute. The predominance of NRAS codon 61 mutations as a feature of carcinomas indicates that the diagnosis of adenoma alongside the presence of this mutation should be made cautiously. Our study raises the possibility that follicular adenomas with the RAS mutations have an inherent malignant potential; however, the clinical significance of this finding should be further investigated in more patients and over a longer follow-up period.
Introduction
In recent years, multiple studies have shown that many thyroid tumors, especially follicular tumors, harbor somatic mutations to three forms of RAS: HRAS, KRAS, and NRAS. With respect to thyroid tumors, the association between the frequency of RAS mutations and malignant potential in the different histological subtypes is still unresolved, in large part due to methodological differences and the small numbers of cases typically examined. A pooled literature analysis based on 39 reported studies by Vasko et al. revealed that mutations on NRAS codon 61 were significantly more frequent in follicular tumors (38%) than in papillary carcinomas (5%), and in follicular tumors, these mutations were significantly more frequent in carcinomas (24%) than in adenomas (14%) (10). However, this study involved cases reporting no NRAS mutation in adenomas or carcinomas, indicating the vast heterogeneity of the cases included (11,12). Several previous reports have also suggested that RAS mutations are a marker of aggressive behavior in thyroid cancer (13 –15), but these studies compared well-differentiated carcinomas with poorly differentiated ones; therefore, the clinical significance of RAS mutations, specifically in follicular thyroid tumors, which harbor the mutation most frequently, is still unclear.
In the present study, we analyzed the frequency mutations in all three of the RAS variants in a cohort of patients who had undergone surgery for follicular adenoma or carcinoma. We further analyzed the clinical significance of the mutation with regard to the clinicopathological features of follicular tumors and prognosis in these patients.
Methods
Patients
In a retrospective analysis of thyroid tumor patients treated at the Kanagawa Cancer Center Hospital (KCCH) during the 6 consecutive years from 1994 to 1999, 44 patients were found to have follicular thyroid adenoma. During the 16 consecutive years from 1990 to 2005, 65 patients were found to have FTC. At the time of analysis, all samples were re-reviewed by a surgical pathologist who specializes in thyroid tumors (H.H). Another specialist of thyroid tumor pathology (T.K.) was consulted for cases where the diagnosis was difficult, and consensus was reached between the two individuals. The pathologic diagnosis was made according to the latest World Health Organization (WHO) classification of thyroid cancer (6). The patients with adenoma involved in this study had been followed-up for >10 years, and the diagnosis of adenoma in this group was considered reliable. Follicular carcinomas were further differentially diagnosed as either being (a) minimally invasive carcinomas with limited trans-capsular invasion and/or limited vascular invasion, or being (b) widely invasive carcinomas with widespread invasion into perithyroidal tissues or organs and/or vascular invasion, again according to the WHO classifications. Those cases where >5% of the total follicular carcinoma tissue mass comprised a poorly differentiated component were defined as cases with poorly differentiated components. The Kanagawa Cancer Center institutional review board approved this study.
Mutation analysis of the RAS in patients
Mutations of the HRAS, KRAS, and NRAS at codons 12, 13, and 61 were examined using a loop-hybrid mobility shift assay (LH-MSA) developed elsewhere (16). DNA was extracted from thin-sliced formalin-fixed and paraffin-embedded tumor samples using a Pinpoint slide DNA isolation system (ZYMO Research). Briefly, the deparaffinized tissues were digested with proteinase-K followed by heat inactivation at 95°C for 10 minutes, and directly subjected to polymerase chain reaction (PCR) with primers designed to amplify genomic DNA, including the site to be examined. At the end of the 45 cycles of PCR, the 72-mer loop-hybrid generator (LH-G), specific to each mutation, was added to the reaction mixture at a final concentration of 500 nM and processed using heat-denaturation followed by an annealing step to generate loop-hybrids. The PCR primer and LH-G probe sequences are provided in Table 1. The final PCR products were separated on native 10% polyacrylamide gels (ATTO, Inc.). After electrophoresis, the gels were stained with SYBER Green I (Cambrex Bio Science), and the DNA bands were detected using a laser-scanning imager Storm860 (GE Health Care BioScience). The gene mutations were identified as mobility-shifted loop-hybrid bands. Each LH-G is a single-strand oligonucleotide with an artificial internal 10-nucleotide deletion that generates a small loop in the hybridized complementary strand adjacent to the mutated nucleotides. The PCR products found to contain mutated loop-hybrid bands by LH-MSA were further confirmed by direct sequencing with the 3130 Genetic Analyzer (Applied Biosystems/Life Technologies).
fw, forward primer; rv, reverse primer; LH-G, loop-hybrid generator; bps, base pairs.
Statistic analyses
Associations between the mutation status of the respective RAS variants and clinicopathological features of each of the tumor samples were evaluated with a χ 2 test. The following clinicopathological features were examined: age, gender, tumor size, presence or absence of lymph node metastases, distant metastases, capsular or vascular invasion, and the presence of poorly differentiated tumor components. The overall survival rate and the disease-free survival rate were assessed using Kaplan–Meier analysis. All statistical analyses were conducted using SPSS II software (version 11.0.1J for Windows).
Results
Mutation status of RAS variants in follicular thyroid tumors
PCR amplification was performed successfully on 40 adenomas and 58 carcinomas. However, most likely due to poor-quality DNA, PCR amplification was not possible in four adenoma and seven carcinoma specimens. Thus, these samples were excluded from the subsequent analysis. The mutations found in the group of adenoma samples (HRAS codon 61, NRAS codon 12, and NRAS codon 61) are shown in Figure 1. Representative results for the HRAS codon 12 and the KRAS codons 12 and 61 mutations were selected from the follicular carcinoma cases, because the adenomas did not have these mutations. A single loop-hybrid band was found in samples without mutations, and loop-hybrids with mutations appeared just below or above the normal band, indicating that the mutations were heterozygous. Electrophoretic mobility of the mutated loop-hybrids was slightly different from each other. For example, NRAS Q61K (CAA>AAA) and Q61R (CAA>CGC) moved faster than the most common mutant Q61R (CAA>CGA) (Fig. 1, lanes 13, 14, and 15, respectively) (where CAA is the normal 61st codon of NRAS, and Q, R, and K are one letter abbreviations for the amino acids glutamine, arginine, and lysine, respectively). Only one NRAS Q61K mutant was found throughout the adenomas and carcinomas examined. A homozygous RAS mutation without the normal loop-hybrid band was identified only in one case, and that was the NRAS Q61K mutation in an adenoma sample.
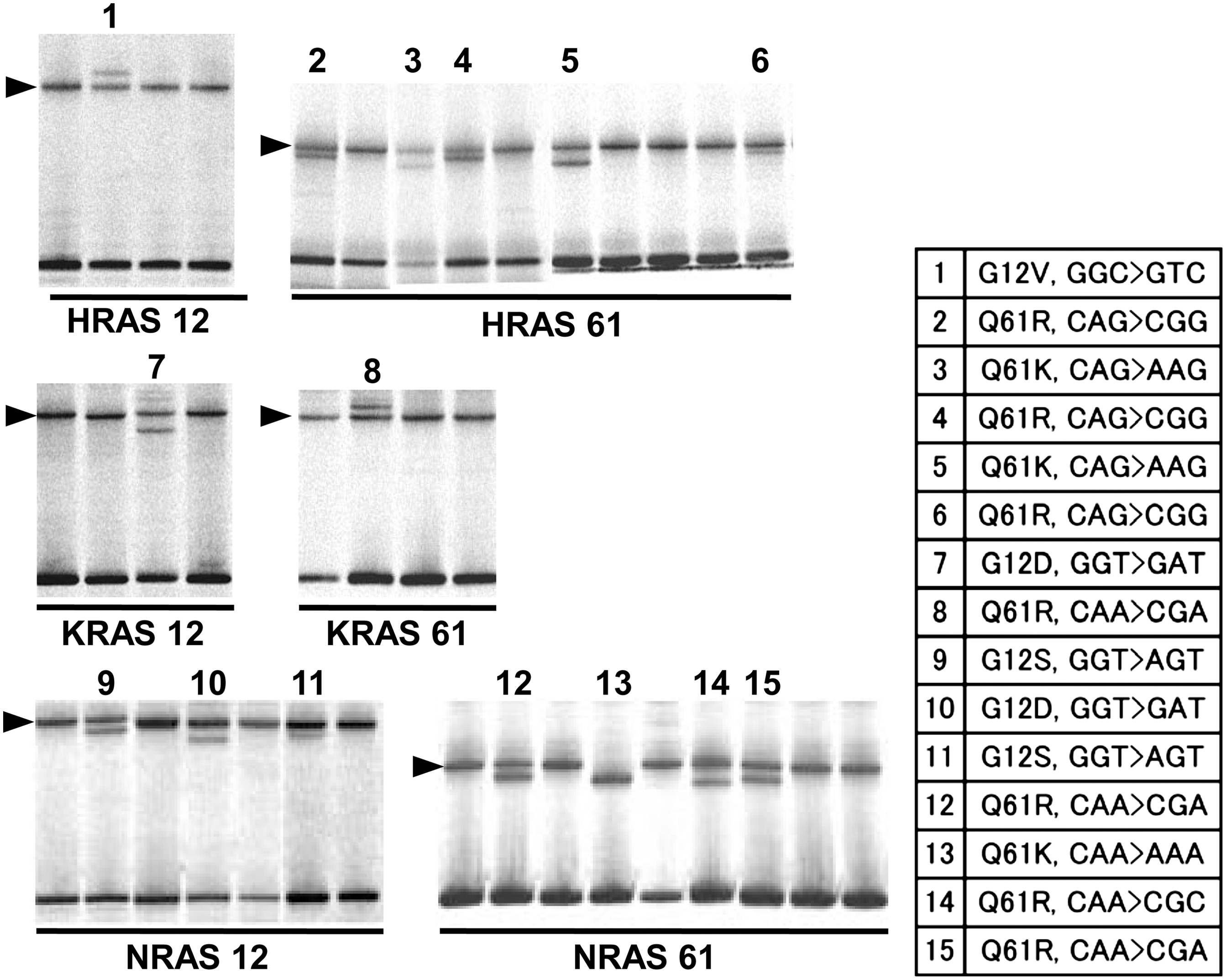
Detection of RAS mutations using the LH-MSA method. All types of RAS mutations demonstrated by the loop-hybrid mobility shift assay (LH-MSA) are shown. For the adenoma, the HRAS codon 61 and NRAS codons 12 and 61 are shown. Mutations on the HRAS codon 12 and KRAS codons 12 and 61 were selected from follicular carcinoma specimens. An arrowhead on the left side of each panel indicates the loop-hybrid band corresponding to the wild-type sequence. Lanes with Arabic numerals above contain loop-hybrid bands with the mutation just below or above the wild-type ones. The gene symbols followed by the codon number of the mutation are provided below each panel. The table on the right side indicates the nucleotide sequence of the mutation determined by direct sequencing (the wild-type codon is on the left and the mutated codon is on the right). V, valine; R, arginine; Q, glutamine; D, aspartic acid; S, serine; K, lysine.
The frequency of each RAS mutation in follicular tumors is summarized in Table 2. In total, 12 out of 40 adenomas (30%) and 33 out of 58 carcinomas (57%) harbored RAS mutations, and the frequency was significantly higher in carcinomas than in adenomas (p<0.01). In carcinoma samples, most RAS mutations were found at the NRAS codon 61 (p<0.01).
Previous reports examining follicular adenomas and carcinomas simultaneously with the same method that examined at least 20 adenomas or carcinomas. Vasco's pooled: the results of this pooled analysis from 22 reported studies in Vasco et al. (10)
In the present study, any RAS gene mutation was significantly more frequent in follicular carcinomas than in follicular adenomas (p<0.01).
Carcinomas, where the RAS mutation was significantly accumulated on NRAS codon 61 (p<0.01). This accumulation was not observed in adenomas.
Clinicopathological characteristics and status of RAS mutations in follicular adenoma samples
The age of patients with thyroid adenomas ranged from 21 to 83 years (median, 51 years) and included only one male (Supplementary Table S1). In the patients with adenomas, none of the clinicopathological characteristics, including patient age, gender, tumor size, or histological variations (normo- and macro-follicular or micro-follicular adenomas), were found to significantly correlate with the overall RAS mutation status (Table 3). Although each case number was small (four HRAS codon 61, four NRAS codon 12, and four NRAS codon 61), the HRAS codon 61 mutation showed a tendency to be associated with the micro-follicular subtype of adenomas (p=0.056). In the adenomas tested, there were no detected KRAS mutations or HRAS codon 12 mutations.
Clinicopathological characteristics and outcomes in patients with follicular carcinomas harboring RAS mutations
The age of follicular carcinoma patients ranged from 11 to 78 years (median, 51 years) and included 14 males and 44 females. In nine patients, distant metastases were found at the initial operation, seven to the bone and two to the lung. Fifty-one tumors were minimally invasive carcinomas, and 7 were widely invasive. Histological examination revealed capsular invasion in 50 tumors, and vascular invasion in 24 tumors. Ten tumors had a poorly differentiated component that was estimated to occupy approximately >5% of each tumor. In this study, the median follow-up time was 8 years. Within this period, five patients suffered recurrence as new distant metastases in the bone (four patients) or the lung (one patient), and five patients died (due to cancer-specific events in four of these patients). Precise clinicopathological information relating to the specific RAS mutations is presented in Table 4 and Supplementary Table S2 (Supplementary Data are available online at
“Poorly components” indicates the number of cases containing poorly differentiated components according to the criteria described in the text.
N, refers to the numbers of patients with microscopic nodal metastasis; M, indicates the presence of distant metastasis at the initial operation.
The relationship to the clinicopathological features present at the time of the initial tumor resection was also analyzed, and follicular carcinomas with the NRAS codon 61 mutation showed a tendency to have distant metastases (p=0.053) (Table 4). When distant metastases were found both at the time of the initial operation and as a recurrence, these cases were significantly associated with the NRAS codon 61 mutation (p=0.020) and showed a tendency to have any of the RAS mutations (p=0.060) (Table 5). In the analyses relating to patient prognosis, there was a significant association between follicular carcinoma patients harboring any RAS mutation and mortality (p<0.05) (Table 5). When restricted to the NRAS codon 61 mutation, the association was not significant (p=0.36). The Kaplan–Meier analysis demonstrated a significant association between the presence of any RAS mutation and poor overall patient survival (p<0.05) (Fig. 2). For each RAS mutation, one of two follicular carcinoma patients with the KRAS codon 61 mutation presented with recurrent bone metastasis and died of the disease. In this case, the risk of recurrence and cancer-specific death were significant (p<0.01 and p<0.05, respectively) (Supplementary Table S2).
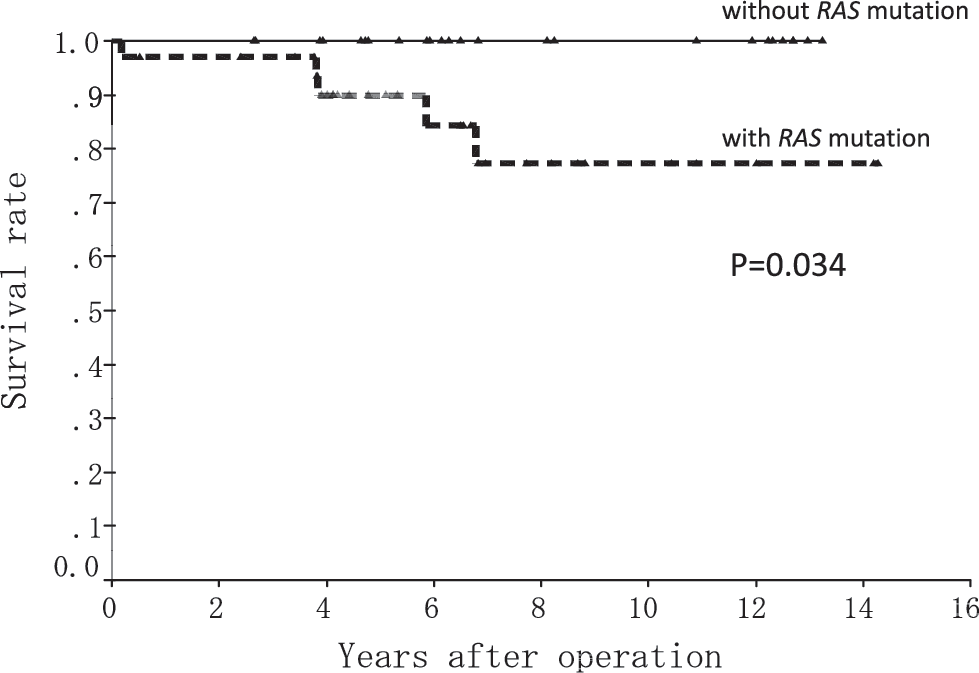
Overall survival of follicular carcinoma patients with or without the RAS mutations.
“Distant metastasis” includes both metastasis at the initial operation and metastasis found as a recurrence.
Discussion
As summarized in Table 2, this is the first study to simultaneously examine a large number of cases of follicular adenoma and carcinoma for mutations in all three forms of RAS. In thyroid tumors, the frequency of NRAS mutations, especially at codon 61, has been reported to lie within a wide range of values, from 8% to 50% in adenoma to 7% to 62% in carcinoma (2,4,10,13,17,18). Such large differences may reflect the different experimental methodologies used in each study and the typically small number of cases examined. For instance, Vasko et al. reported that the rate of mutation was significantly lower with direct sequencing than without (10). However, in the present study, LH-MSA followed by direct sequencing of the PCR products was able to confirm the presence of mutations and clearly demonstrated that RAS mutations are significantly more frequent in follicular carcinomas than in adenomas. Mutations of the respective RAS were most frequently detected on the NRAS codon 61, which is consistent with several other reports (4,10,13,19 –21). In contrast to the carcinomas, the mutations detected in the adenoma samples were scattered among the HRAS codon 61 and the NRAS codons 12 and 61 at a similar frequency. The HRAS codon 61 mutation was significantly associated with micro-follicular adenoma, but this was limited to only a small number of cases (n=4), and further investigation is required to clarify this association. Because the NRAS codon 61 was frequently detected in the carcinomas samples, the diagnosis of adenoma alongside the presence of this mutation should be made cautiously. However, >10 years have passed without any disease progression in all four of the adenoma cases with the mutation (data not shown). Further studies on a larger number of adenoma cases are required to determine the significance of the NRAS codon 61 mutation in adenomas.
The NRAS codon 61 mutation, the most frequent RAS mutation in follicular carcinomas, showed a positive association with the overall distant metastasis. Basolo et al. reported that two of the five follicular carcinomas with bone metastasis examined had the NRAS codon 61 mutation (14). Follicular carcinomas with this mutation might have the potential to be metastatic. Garcia-Rostan et al. further suggested that RAS mutations are a marker of aggressive thyroid cancer behavior and poor outcomes, but their analyses did not focus on follicular tumors (13). Although the NRAS codon 61 mutation was associated with distant metastases, it was not directly associated with the death or the disease-specific death of the patients in our study. However, the overall presence of RAS mutations together with the NRAS codon 12 and the other two RAS mutations were significantly associated with patient mortality. One of 5 patients with the HRAS mutation and 1 of 4 patients with the KRAS mutation died of the disease, which represents half of the cancer-specific deaths in the 58 patients examined. There is a possibility that the malignant potential of the NRAS codon 61 mutation, although the most frequent RAS mutation, may not confer the same malignant potential as the other two forms of RAS, and that a longer period to develop into life-threatening disease is required.
In the present study, we clarified the frequency of RAS mutations in a sizeable number of follicular thyroid tumor cases, and also raised some possibilities concerning the clinical significance of these mutations. However, follow-up studies in a larger cohort of patients with a longer follow-up period are required to fully understand the significance of these mutations in thyroid follicular tumors.
Footnotes
Acknowledgments
This work was partly supported by a grant from the Japanese Ministry of Education, Culture, Sports, Science and Technology (to Y. Miyagi) and by a grant for Collaboration between Hospital and Research Institute, Kanagawa Cancer Center (to Y. Miyagi and A. Yoshida).
Disclosure Statement
None of the authors involved in the present study has any conflicts of interest to disclose.