
Abstract
Background:
Hyperthyroidism has been associated with liver function abnormalities; however, cholestasis as the presenting feature of adolescent Graves' disease has not been previously reported.
Patient Summary:
The patient was a 17-year-old girl who presented with severe cholestasis and was found to have Graves' disease. She also had a positive hepatitis A immunoglobulin M antibody but her clinical course, the liver histopathology, and her mildly elevated transaminases indicated that the acute hepatitis A infection was not dominant at the time of presentation with severe cholestasis. Other causes of cholestasis, including congestive heart failure, autoimmune hepatitis, and viral infection, were excluded. Treatment with methimazole resolved the hyperthyroidism, and the cholestasis improved, as well.
Conclusion:
Severe cholestasis is a rare presenting feature of Graves' disease. With careful monitoring, methimazole can be used to treat the hyperthyroidism in the setting of cholestasis.
Introduction
Patient
Two weeks prior to admission to the Mount Sinai Medical Center (MSMC), a 17-year-old girl was hospitalized in Haiti with vomiting, diarrhea, dark-colored urine, and jaundice. There she was diagnosed with acute hepatitis A based on a positive hepatitis A immunoglobulin M (IgM) and aspartate aminotransferase (AST) and alanine aminotransferase (ALT) measuring in “the thousands.” She was treated only with vitamin K and vitamin B12. One week prior to hospitalization in Haiti, she reported a painful neck mass and had laboratory tests consistent with hyperthyroidism (Table 1) but no treatment was given. Two days prior to admission to MSMC, she was hospitalized in the United States with jaundice, abdominal pain, pruritus, and 10–20 pound weight loss. She had elevated total and direct bilirubin levels. Her thyroid function tests were consistent with hyperthyroidism (Table 1). She had sinus tachycardia (heart rate 137 beats/min); electrocardiogram and echocardiogram were otherwise normal. One day prior to admission to MSMC, she was treated with vitamin K, propranolol, prednisone, and methimazole. She was transferred for “impending liver failure” based on an elevated international normalized ratio and liver transaminases (Table 1).
The following are the normal ranges and units for the tests at the various institutions.
MedLab Laboratoire Medical (Port-au-Prince, Haiti): TSH=0.32–5.0 μIU/mL, total T3=80–200 ng/dL, total T4=5.0–12.0 μg/dL.
Maimonides Medical Center Laboratory (Brooklyn, NY): TSH=0.43–5.3 mcIU/mL, total T3=0.7–1.7 ng/mL, total T4=5.0–10.4 mcg/dL, total bilirubin=0.2–0.9 mg/dL, direct bilirubin=0.1–0.5 mg/dL, ALT=10–40 IU/L, AST=15–37 IU/L, INR=0.9–1.2.
Mount Sinai Medical Center Laboratory (New York, NY): Free T4=0.60–1.10 ng/dL, TSH=0.34–5.60 μIU/mL, total T3=87–178 ng/dL, total T4=6.1–12.2 mcg/dL, total bilirubin=0.1–1.2 mg/dL, direct bilirubin=0.0–0.8 mg/dL, ALT=1–53 U/L, AST=1–50 U/L, GGT=8–35 U/L, INR=0.9–1.2.
Quest Diagnostic Laboratory (Chantilly, VA): TSI<125%.
Methimazole was started one day prior to admission at a dose of 20 mg by mouth every 12 hours. The dose was increased to 20 mg by mouth every 8 hours on the day of admission and she remained on that dose until 49 days following admission.
Day of admission.
↑, elevated value for the laboratory; ↓, low value for the laboratory; ALT, alanine aminotransferase; AST, aspartate aminotransferase; GGT, gamma-glutamyl transpeptidase; INR, international normalized ratio; TSI, thyroid-stimulating immunoglobulin; T4, thyroxine; T3, triiodothyronine.
On physical exam, she was in mild distress, with tachycardia (128 beats/min). Blood pressure was (111–136)/(56–69) mmHg; she was afebrile. Her weight was 63.4 kg, height 170.9 cm, and body mass index 21.7 kg/m2, which were at the 75th, 88th, and 56th percentiles for age, respectively. She had exophthalmos, scleral icterus, sublingual icterus, melanonychia parallel to the fingernail beds, and a diffusely enlarged, nontender thyroid gland without nodules. Laboratory results were consistent with severe cholestasis and Graves' disease but not liver failure (Table 1). Autoimmune hepatitis (AIH)–related antibodies, including antinuclear antibody, anti-liver-kidney microsomal antibody, and antismooth muscle antibody, as well as antimitochondrial antibody and rheumatoid factor, were negative. Total immunoglobulin G was mildly elevated at 1627 mg/dL (549–1584 mg/dL). IgM antibodies were positive for hepatitis A virus (HAV) infection; however, liver biopsy viral culture did not isolate the virus. Hepatitis B serologies, hepatitis C ribonucleic acid, Epstein Barr virus polymerase chain reaction (PCR), cytomegalovirus PCR, human immunodeficiency virus-1 (HIV-1) antibodies, and HIV-1 enzyme-linked immunosorbent assay were negative. Her alpha 1–antitrypsin phenotype was normal (MM). The histologic appearance of the liver biopsy revealed portal tracts with mild mixed inflammation and mild ductular proliferation. The hepatic lobules exhibited diffuse hepatocellular cholestasis with no significant inflammation, apoptotic hepatocytes, or architecture disarray. Electron microscopy (EM) showed cholestasis and a mixture of normal-sized hepatocytes and larger hepatocytes with numerous mitochondria and lack of glycogen, suggestive of increased metabolic demand.
Shortly after admission, prednisone was discontinued. Treatment was continued with propranolol and methimazole. She was also treated with ursodeoxycholic acid, rifampin, vitamin K, vitamin ADEK, and esomeprazole. Over the course of the following month, her thyroid function normalized and the cholestasis resolved (Table 1 and Fig. 1).
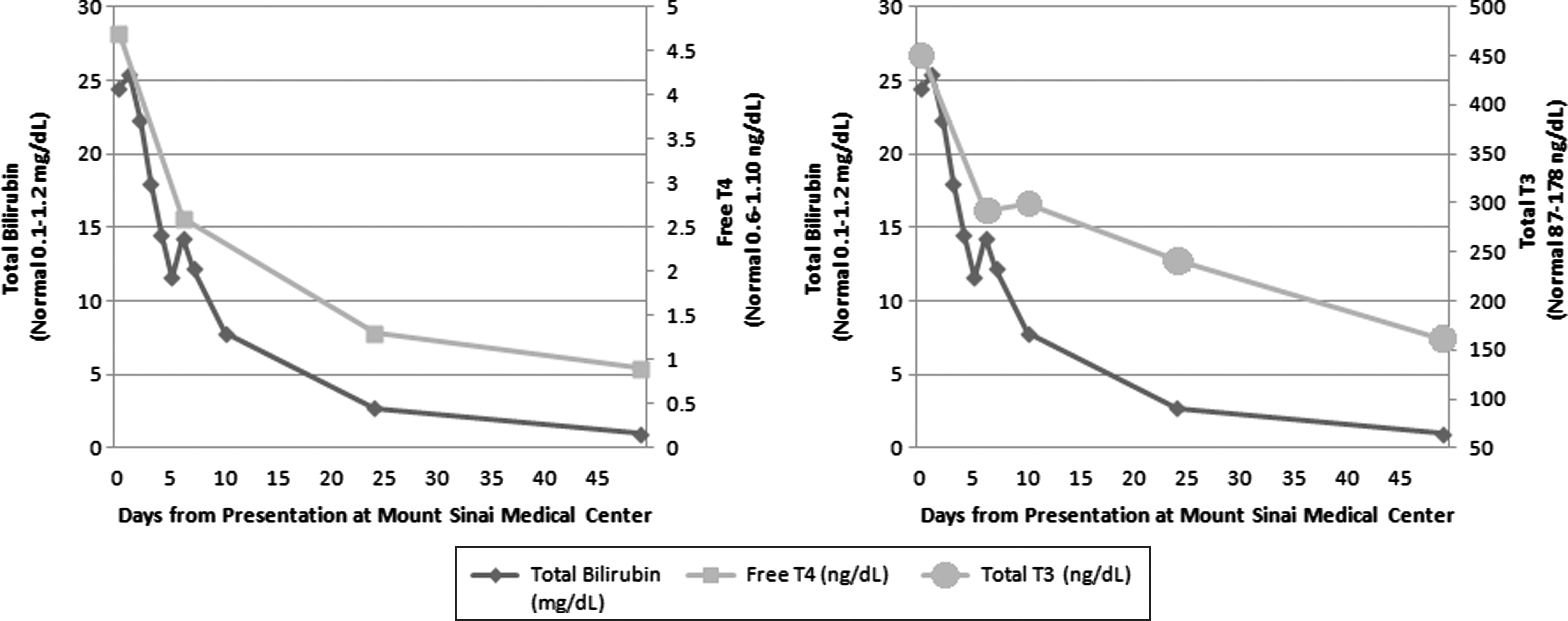
The total bilirubin trended down, as the free thyroxine (T4) and total triiodothyronine (T3) normalized with methimazole treatment.
The patient remained on propranolol and methimazole for 3 months until definitive Graves' disease treatment with thyroidectomy. Postoperatively, she developed hypothyroidism and was treated with levothyroxine. Her liver function tests remained normal for 8 months and she has had no recurrence of cholestasis symptoms for over a year.
Discussion
The patient presented is unique in that cholestasis was the presenting feature of Graves' disease. Hyperthyroidism is associated with liver function abnormalities, including elevations in transaminases, alkaline phosphatase, prothrombin activity, and bilirubin and low serum albumin, although the mechanism of liver dysfunction is unclear (9). Hepatic injury is thought to be due to low hepatic blood flow relative to increased hepatic oxygen demand caused by hyperthyroidism (10). This hypothesis explains cholestasis associated with hyperthyroidism-induced CHF. The patient did not have associated heart failure, but it is possible that the metabolic demands were so great that oxygen supply to the liver was limited, even with normal cardiac function. The EM findings, including lack of glycogen stores and numerous mitochondria, support a high metabolic demand as a cause for the cholestasis.
The correlation of the improvement in bilirubin with the improvement in the thyroid function tests seems to go along with hyperthyroidism being the crucial contributing factor to the cholestasis. There were no other documented causes for the severe cholestasis, including AIH. HAV IgM was positive but viral culture from the biopsy was negative and IgM can remain positive for 4–6 months following a primary HAV infection (11). Cholestasis associated with HAV usually occurs in the setting of chronic infection, which is rare, and typically has a prolonged recovery time of 12–18 weeks (12). In the setting of acute hepatitis A infection, cholestasis lasts 4–30 days and is associated with bilirubin levels usually only as high as 5–10 mg/dL (11). In the United States, at the time of presentation with severe cholestasis (total bilirubin level as high as 28 mg/dL), the patient's transaminases were not significantly elevated (ALT as high as 145 IU/L, AST as high as 152 IU/L), indicating that hepatocyte inflammation, and thus HAV infection, was not dominant at the time of severe cholestasis. The full resolution of cholestasis within three and a half weeks of initiation of methimazole treatment also made HAV infection an unlikely cause of the severe cholestasis. Furthermore, EM did not reveal inflammatory infiltrates, as would be expected in the setting of HAV infection. A prior HAV infection may, however, have increased the patient's metabolic demands, causing an exacerbation of the hyperthyroidism-induced cholestasis.
Of note, the patient had resolution of both the hyperthyroidism and cholestasis while treated with methimazole, an agent known to, on occasion, cause cholestasis (13 –15). Propylthiouracil was not used for treatment due to recent publications reporting higher rates of hepatotoxicity in children (16). The patient's improved thyroid status without further liver dysfunction suggests that methimazole can be used to treat hyperthyroidism in the setting of cholestasis. Further studies are needed to confirm the safety of methimazole in patients with liver abnormalities.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.