
Abstract
Background:
Patients who have thyroidectomies for thyroid nodules that are suspected of being malignant, called here “main nodules,” occasionally have second nodules, called here “accessory nodules” that are evaluated by ultrasonography (US) and fine-needle aspiration cytology (FNAC). Most accessory nodules are diagnosed as benign based on preoperative US and FNAC. To evaluate the accuracy of US and FNAC for a group of nodules which were likely to be mostly benign we evaluated procedures to diagnose accessory nodules.
Patients and Methods:
In a total of 643 patients who underwent thyroidectomy for their main nodules, 866 accessory nodules were evaluated by US and/or FNAC preoperatively. All were evaluated by histopathological examination postoperatively. Of the 866 accessory nodules, 501 were evaluated by US only and 365 were evaluated by US and FNAC.
Results:
While the 363 accessory nodules were diagnosed as malignant by histopathology, 235 nodules were malignant by US and histopathology and 115 nodules were malignant by FNAC and histopathology. Among the accessory nodules that were diagnosed as benign by histopathology, 7.2% were malignant by US, and 4.4% were malignant by FNAC. Among the accessory nodules that were diagnosed as benign by FNAC, 15.0% were malignant by histopathology. This was a significantly higher percentage than the value of 6.2% for the accessory nodules diagnosed as benign by US but malignant by histopathology. Accessory nodules with a benign cytology on FNAC that were malignant were significantly smaller than those with a benign cytology and histopathology. Among the 126 accessory nodules that were read as benign by both US and FNAC, only one (0.8%) was diagnosed as papillary thyroid carcinoma by histopathology.
Conclusion:
These data suggest that diagnostic accuracy of benign nodules based on both US and cytological evaluation was supported by the evidence of high-level histopathological compatibility in accessory nodules. FNAC and US have a low but not negligible false-negative diagnostic rate. When FNAC is combined with US the false-negative rate is probably very low.
Introduction
When thyroid nodules are judged to be benign by US and FNAC examination, periodic observation is recommended by Papini et al. (7). This recommendation is supported by the observation that these nodules usually decrease in size or only have a slow growth during long-term observation (8,9). Most benign cytology readings are predictive of similar findings on long-term follow-up (10 –12). Therefore, immediate surgery is only used for a minor proportion of preoperatively benign nodules, such as huge nodules causing tracheal compression or other suspicious findings for malignancy.
Because there are few large series in which thyroid nodules that are very likely to be considered benign by US and FNAC were subjected to histopathological examination, we studied a series of nodules in this category that also were subjected to histopathological examination because thyroidectomy was performed, usually not to evaluate these nodules, but for another more clinically evident nodule.
Patients and Methods
Subjects
A total of 1378 patients underwent surgical resection of their thyroid nodules between January and December 2008 in our hospital. Subsequent histopathological examination showed 1050 malignant and 328 benign nodules, respectively. Among them, 643 patients additionally had one or more nodular lesions (total: 866 nodules) that were evaluated by US and/or US-guided FNAC examinations preoperatively and by histopathological examination postoperatively (Fig. 1).
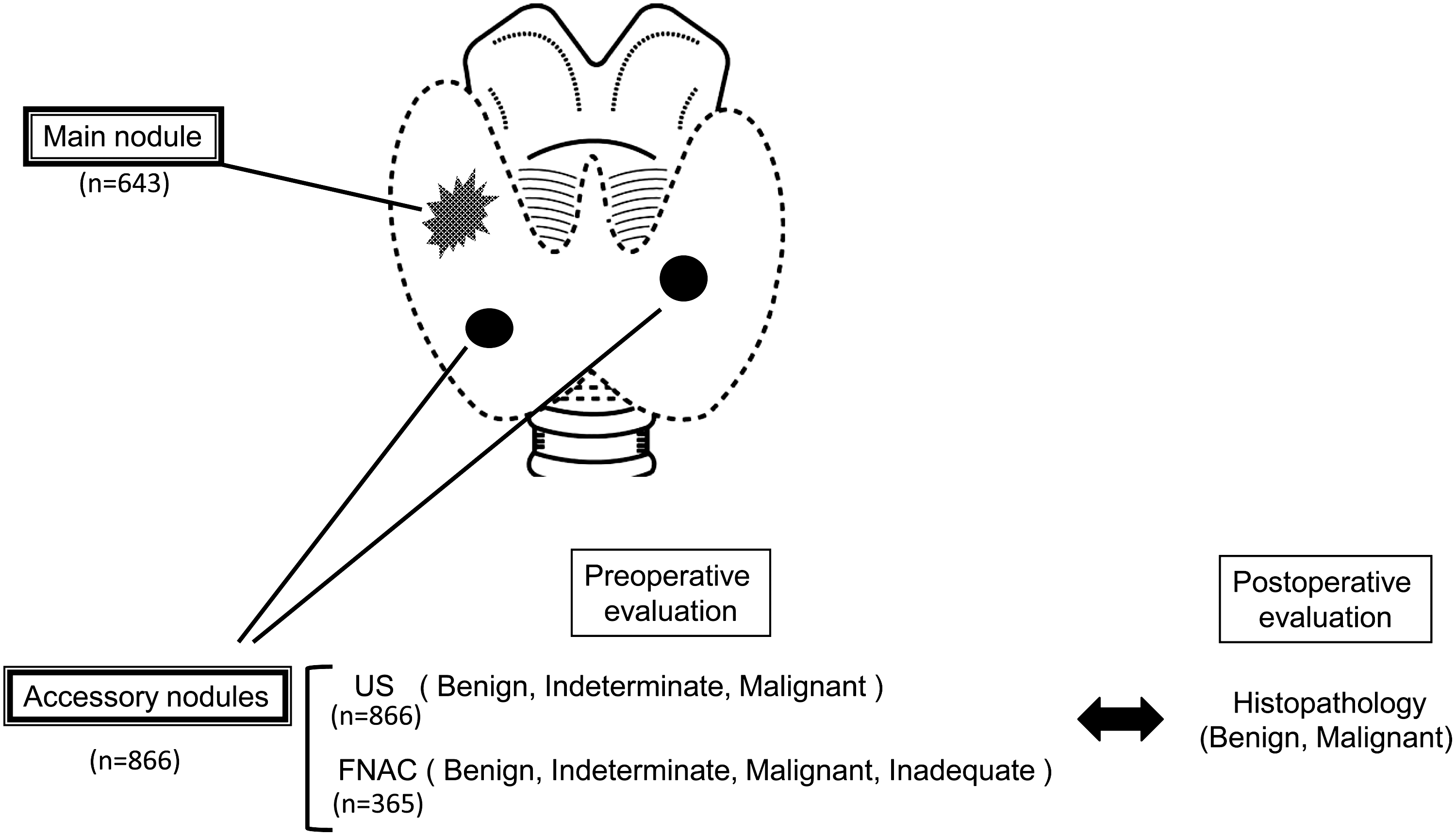
Main nodules and accessory nodules. The relationship between main nodules and accessory nodules is illustrated with their numbers.
Definition of main nodules and accessory nodules
The primary thyroid nodule which was subject to surgical treatment in each patient, was termed the “main nodule.” The main nodules in these 643 patients were malignant in 559 patients and benign in 84 patients. The other nodules that occurred in the same thyroid as the main nodule were evaluated by US and/or US-guided FNAC examinations preoperatively and by histopathological examination postoperatively. They are referred to here as “accessory nodules.” There were 501 accessory nodules that were evaluated by US only and 365 nodules that were evaluated by both US and FNAC (Fig. 1). None of the accessory nodules were evaluated by FNAC only.
The ultrasound diagnostic equipment used was SSA-770A (Aprio; Toshiba Medical Systems, Odawara, Japan) in connection with two linear transducers, an 8-MHz probe (PLT-805AT), and 12-MHz probe (PLT-1204AT). US examinations were performed by well-trained, registered medical sonographers. The malignant grading for US classification systems in Kuma Hospital was previously described (3,13). The cytological results of US-guided FNA were classified as benign, indeterminate (follicular lesions), malignant (including suspected of malignancy), or inadequate. The preoperative diagnosis for all accessory nodules was compared with subsequent histopathological findings from surgical specimens (Fig. 1).
Statistical analysis
Comparisons of accessory nodule sizes were performed employing the Mann–Whitney test. The frequency distribution of malignancy in the different groups preoperatively judged as benign was compared by χ 2 test. p<0.05 was accepted as indicating significance.
Results
The correlation of the preoperative US judgment with histopathological diagnosis among total 866 accessory nodules is shown in Table 1. The positive predictive value (the percentage of malignant US diagnoses that had a malignant histopathology) and the negative predictive value (the percentage of benign US diagnoses that had a benign histopathology) were 86.7% and 93.8%, respectively. Twenty-six misjudged tumors with a benign US but malignant histopathology consisted of 22 papillary thyroid carcinomas, 3 follicular carcinomas, and 1 medullary carcinoma. The size of tumors with a benign US reading but malignant histopathology (range: 5–39 mm, median: 8.5 mm) was significantly less than that of nodules with both a benign US and histopathology (range: 3–57 mm, median: 15 mm; p=0.0002). FNAC judgment among 365 accessory nodules was compared with the histopathological diagnosis (Table 2). These positive and negative predictive values were 92.7% and 85.0%, respectively. The 28 misjudged tumors that had a benign cytology but a malignant histopathology were all papillary thyroid carcinomas. The size of the tumors with a benign cytology but malignant histopathology (range: 2–30 mm, median: 8 mm) was significantly less than that of nodules with both a benign cytology and histopathology (range: 3–64 mm, median: 20 mm; p<0.00001).
Size is presented as median values.
US, ultrasonography.
Size is presented as median values.
FNAC, fine-needle aspiration cytology.
The rate of accessory nodules that were malignant but were read as benign by FNAC (15.0%) was significantly higher than the value of 6.2% for accessory nodules that were malignant but were read as benign by US (χ 2=12.18; p<0.001). When these accessory nodules were divided into two groups, nodules smaller than 1 cm in size and nodules 1 cm or larger, the false-negative rate (20/44, 45.5%) based on FNAC was significantly higher than that (15/123, 12.2%) based on US judgment in the smaller group of nodules (χ 2=21.64; p<0.001) but not in the larger group of nodules (χ 2=0.81; p=0.369).
Among all 866 accessory nodules, 126 nodules in 126 patients had a diagnosis of benign on both US and FNAC criteria. Total thyroidectomy was carried out for 91 patients (72%) and lobectomy for 35 patients (28%). Sixty-nine accessory nodules judged as benign on both US and FNAC (55%) were located in the lobe of the thyroid contralateral to the main nodules that consisted of 96 malignant and 30 benign nodules. Histopathological diagnoses of these accessory nodules from surgical specimens showed that 125 nodules were benign, with only one nodule turning out to be malignant; this was a papillary thyroid carcinoma (Table 3). Thus, the prevalence of thyroid cancer in accessory nodules that were read as benign on both US and FNAC was 0.8%. The misjudged nodule was the solid type with a diameter of 8 mm, located in the lobe contralateral to the main nodule. Preoperative cytological specimens of this nodule showed many lymphocytes but no thyroid epithelial cells.
PTC, papillary thyroid carcinoma.
Discussion
To verify the accuracy of the benign diagnosis of thyroid nodules based on US and FNAC evaluation, the histopathological findings are used to provide a definitive diagnosis. However, histopathology is not available if surgical resection is not performed and in most patients with nodules that are considered to be benign do not undergo surgical resection. Several studies reported the outcome of longstanding thyroid nodules by assessing changes in their size, with the observation periods varying from several months to more than 10 years (9 –12). The growth rates of differentiated thyroid cancers are generally slow. Indeed, in one report there was no significant difference in growth between benign and malignant nodules (14). Therefore, it is difficult to define the proper follow-up periods and determine the meaningful growth speed for judging potential malignancy. Re-evaluation by FNAC after an interval is a reliable approach, but the cytological findings are not completely compatible with histopathological findings. Further, the histopathological relevance in previous reports has been verified for nodules with a benign cytology that had high risk factors for surgical indication, which is not representative for the follow-up of patients with benign nodules. The accessory nodules judged as benign on both US and FNAC in this study may be more like a follow-up group with benign nodules because they are not susceptible to selection bias for surgical indications such as the nodular size. Our approach of evaluating accessory nodules enables us to confirm histopathological information of benign nodules in the follow-up group.
The high negative predictive value (93.8%) of US evaluation among accessory nodules shows that our US classification system is reliable for a benign diagnosis as compared with previous reports (4,15,16). In contrast, the negative predictive value (85.0%) of FNAC for malignancy in accessory nodules was relatively low compared to other studies (93%–99%) (17 –19). One possible reason for this discrepancy may be the small sizes of nodules in our subjects. The sizes of tumors with a benign cytology but malignant histopathology were significantly smaller than those of nodules with both a benign cytology and histopathology, and 71% of these tumors with a malignant histopathology were less than 10 mm (Table 2 and data not shown). The diagnostic performance of FNAC is reduced by the technical difficulty of accurately aspirating cells from small nodules, and a subsequently inadequate biopsy or undistinguished features of cytological specimens causes potentially malignant tumors to be misjudged as benign nodules. However, combined evaluation employing both US and FNAC markedly improved the preoperative diagnostic accuracy, resulting in a low pathological risk of malignancy (0.8%). Moreover, a false-negative rate by FNAC is more likely to occur for small nodules than a false-negative rate by US (Tables 1 and 2). In other words, intrinsic limitations of FNAC can be overcome by careful US evaluation even if the nodules are small. However, a satisfactory comparison of the relative efficacy of US and FNAC with regard to false-negative readings is not possible because not all accessory nodules were evaluated by both US and FNAC.
Despite careful evaluation of thyroid nodules using both US and FNAC examinations, some cases may be difficult to diagnose as benign or malignant. Follicular carcinoma can hardly be differentiated from follicular adenoma by routine US and FNAC evaluation (1). Chronic thyroiditis is very common and occasionally presents focally low-echoic lesions similar to nodules, which may cause sampling error during FNA performance. Therefore, the prevalence of follicular carcinoma and complicated chronic thyroiditis in accessory nodules may be critical for the false-negative rate in this study. A previous report showed that combined evaluation with our US and FNAC system allows the efficient exclusion of follicular carcinoma (13). Indeed, no follicular carcinoma was diagnosed among accessory nodules judged as benign on both US and FNAC. In contrast, one misjudgment of accessory nodules with tentative diagnosis as benign on both US and FNAC was caused by inadequate biopsy with aspiration in the context of chronic thyroiditis. Overall, combined evaluation employing our US and FNAC system can accurately differentiate benign nodules from the multifocal lesions regardless of any histopathological findings of main nodules. However, more attention needs to be paid to evaluate US and cytological judgments in patients complicated with chronic thyroiditis.
Our unique evaluation focusing on accessory nodules outlines the possible histopathological relevance of benign nodules in the observation group. Consequently, the accuracy of diagnosing benign nodules based on US and FNAC evaluation is adequate based on the evidence of high-level histopathological compatibility.
Footnotes
Author Disclosure Statement
The authors declare that no competing financial interests exist.