
Abstract
Background:
Primary mucoepidermoid carcinoma (MEC) of the thyroid is a rare clinical and pathological entity that accounts for <0.5% of all thyroid malignancies. Although the histogenesis has been controversial, most investigators now favor it as arising from either metaplasia of thyroid follicular epithelium or heterologous de-differentiation from papillary thyroid carcinoma (PTC). We report three cases of thyroid MEC found in continuity with, and clearly arising from de-differentiation of, well-differentiated thyroid carcinomas (WDTCs).
Patient Findings and Summary:
The cases presented here included two women (aged 22 and 52) and one man (aged 58). One of these cases arose in conjunction with PTC, one with follicular thyroid carcinoma (FTC), and one with Hurthle cell carcinoma (HCC). In all three cases, there was a gradual transition in morphology between the areas of typical WDTC and the areas showing MEC differentiation. In addition, immunohistochemistry demonstrated a gradual loss of thyroid specific markers (thyroid transcription factor-1, thyroglobulin) mirroring the change in morphology.
Conclusion:
We conclude that thyroid MEC can arise from metaplastic de-differentiation of WDTC, including FTC or HCC in addition to PTC. Currently, we recommend that after excision, each of the WDTC and MEC components of these tumors be treated with targeted adjuvant therapies, which may involve radioactive-iodine ablation, thyrotropin suppression, and external beam radiotherapy.
Introduction
Much of the controversy surrounding thyroid MEC has centered on its histogenesis. Various authors have suggested that it may arise from intra-thyroidal salivary gland rests, solid cell nests (SCN), and ultimobranchial body remnants or from squamous metaplasia of benign thyroid follicular cells as occurs in Hashimoto's thyroiditis (2,5,13 –16). It has frequently been reported in association with papillary thyroid carcinoma (PTC), where the authors have suggested that it represents metaplastic transformation (13). In this article, we present the first documented series showing association of MEC with all three forms of well-differentiated thyroid carcinoma (WDTC): PTC, follicular thyroid carcinoma (FTC), and Hurthle cell carcinoma (HCC).
Patients and Methods
Patient 1
A 22 year-old woman presented for investigation of a left-sided thyroid nodule during her first pregnancy. She was euthyroid, and clinical examination confirmed a small nodule in the left lobe of the thyroid. A neck ultrasound demonstrated a 2 cm nodule with irregular borders and internal calcification. Fine needle aspiration (FNA) cytology showed features consistent with a follicular neoplasm. During her second trimester, she underwent a diagnostic left hemithyroidectomy. Histology demonstrated a papillary carcinoma with an area of unusual de-differentiation, which at the time was thought to represent a component of poorly differentiated (insular) carcinoma (Fig. 1). After completion thyroidectomy postpartum, she was treated with radioactive iodine and thyroxine suppression.
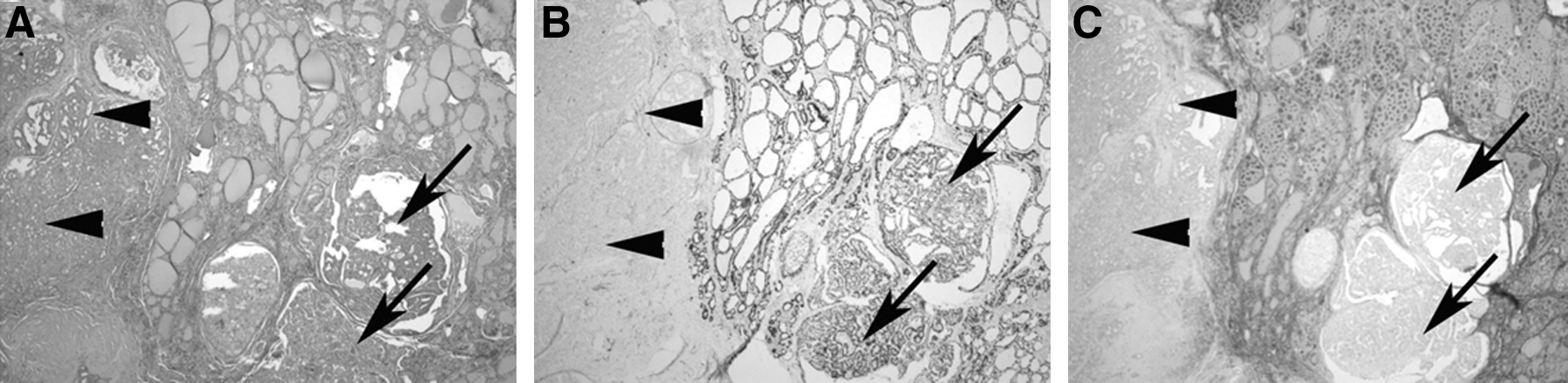
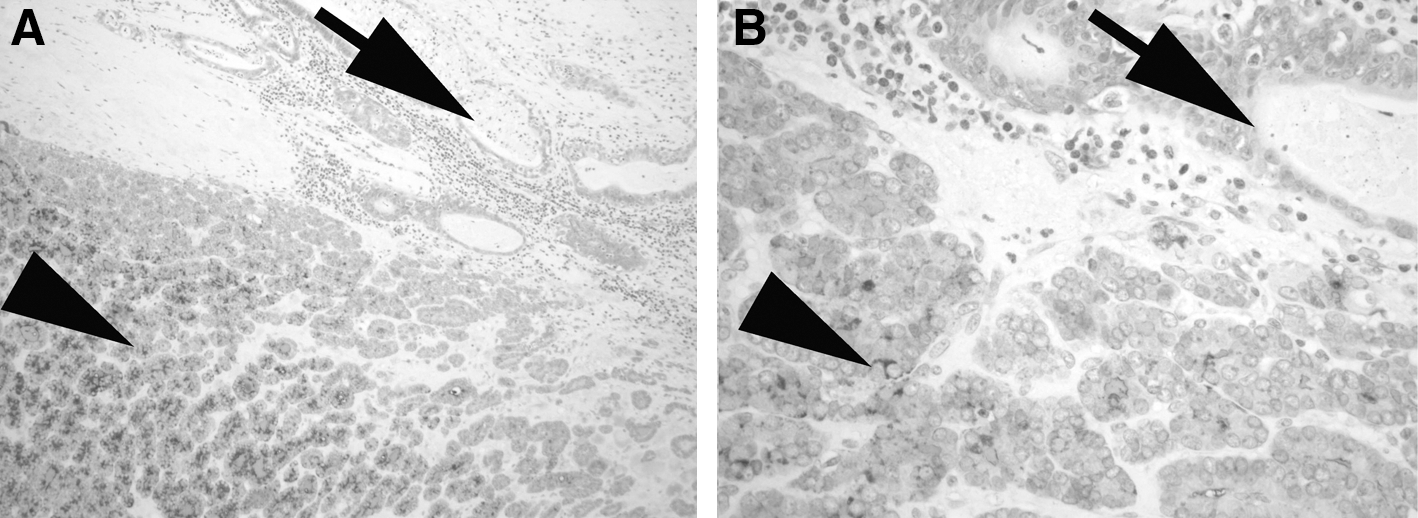
Photomicrographs of serial sections from Patient 1 showing the gradual transition between areas of carcinoma with a papillary architecture (arrows) and MEC (arrowheads)
She presented one year later with a palpable nodule in the left lateral jugular chain. A radioactive iodine scan was negative. A neck ultrasound demonstrated a suspicious node in level II of the left neck. FNA confirmed the presence of recurrent disease. A positron emission tomography (PET) scan did not show any distant metastatic disease; however, bilateral suspicious uptake was seen in the level II neck nodes. Histology from the bilateral selective neck dissection confirmed the presence of a deposit of carcinoma in a single left-level II node. The carcinoma in this node showed diagnostic features of MEC. The primary pathology was reviewed in parallel with the recurrence. With hindsight, it could be appreciated that the area of unusual de-differentiation in the primary tumor (the area thought to be insular carcinoma) actually represented an area of MEC albeit with less classical morphology (Fig. 2). Sixty-three other nodes were negative for disease. There was no evidence of PTC recurrence. Thorough ENT examination excluded the possibility of a primary neoplasm in any major or minor salivary gland. She had a further course of radioactive iodine ablation.
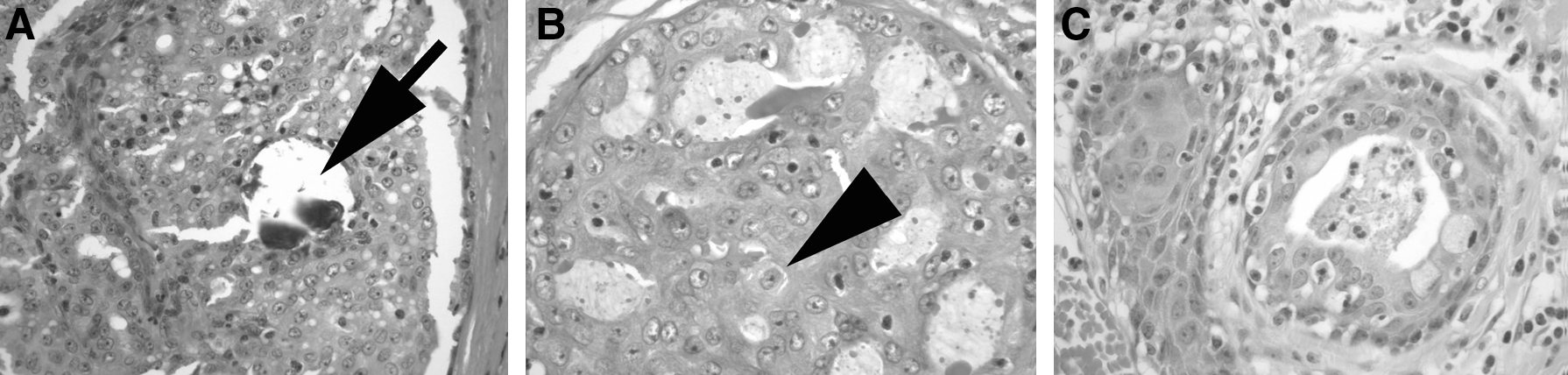
Illustration of the transition zone between the areas of definite papillary carcinoma and definite MEC in patient 1.
She subsequently presented a year later during her second pregnancy with a palpable nodule in the lower aspect of the original Kocher's incision. Radioactive iodine and PET scanning were negative. Her thyrotropin and thyroglobulin were undetectable. However, ultrasound and FNA confirmed the presence of recurrent MEC. She underwent local excision of the lesion during her second trimester. Histology confirmed a 7 mm deposit of MEC and no PTC. She received external beam radiation after delivery.
Patient 2
A 52 year-old woman presented for investigation of rapid enlargement and compressive symptoms associated with her long-standing right-sided goiter. Clinical examination revealed a large right-sided thyroid nodule. She proceeded to have a neck ultrasound that demonstrated a predominantly right-sided multi-nodular goiter with the largest nodule measuring 4 cm. FNA demonstrated an atypical follicular pattern. A diagnostic right hemithyroidectomy was performed.
In the specimen, there was a 38 mm FTC positive for both capsular and vascular invasion. In continuity, there was an area of MEC 20 mm in maximal diameter (Fig. 3). She proceeded to a completion thyroidectomy and right-level six central neck dissection. Histology demonstrated three positive lymph nodes out of five central compartment nodes. All three positive nodes contained deposits of MEC rather than FTC. She had radioactive iodine ablation and was maintained on suppressive doses of thyroxine. External beam radiation was also administered. She is currently disease free at 15 months postoperatively.
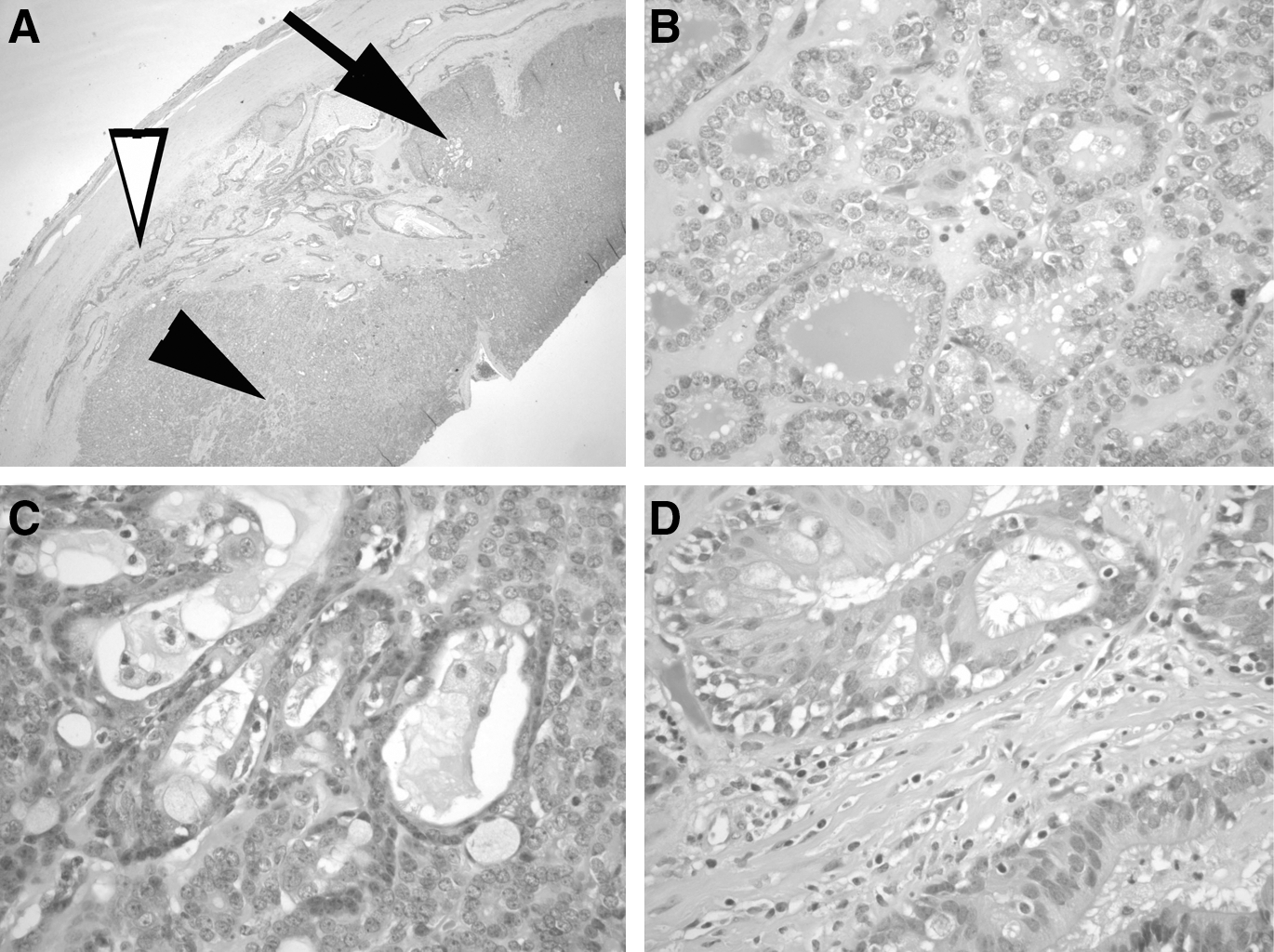
Illustration of the gradual transition between areas of typical follicular carcinoma and areas of MEC.
Patient 3
A 58 year-old man presented for investigation of progressive dyspnea. He was otherwise well. He proceeded to have a neck ultrasound and computed tomography scan that confirmed the presence of a 7×5 cm lesion in the right thyroid lobe, extending retrosternally with tracheal displacement. FNA of the lesion demonstrated atypical follicular pattern with predominant Hurthle cells. A diagnostic right hemithyroidectomy was performed.
Histology demonstrated a 48 mm minimally invasive HCC without vascular space invasion. In direct continuity with this, there was a 20 mm MEC showing similar subtle morphology to that seen in the area of intermediate differentiation present in case 1 (Fig. 4).
Representative photomicrographs from Patient 3 showing areas of Hurthle cell carcinoma
He underwent a completion thyroidectomy, radioactive iodine ablation and thyroxine suppression for the HCC, and external beam radiotherapy for the MEC. He is currently disease free 6 months after treatment.
Immunohistochemistry
Immunohistochemistry was performed on formalin-fixed, paraffin-embedded tissue using commercially available antibodies—thyroid transcription factor-1 (TTF-1) at a dilution of 1/20 (Novocastra, Newcastle-upon-Tyne, United Kingdom, SPT24), thyroglobulin at 1/2000 (Dako, Carpenteria, CA, Cat A0251), polyclonal carcinoembryonic antigen (CEA) at 1/800 (Dako Cat A0115), and calcitonin at 1/800 (Dako Cat A0576).
Results
Hematoxylin and eosin (H&E) tumor sections from all three patients demonstrated the transition of WDTC to MEC. A detailed example is shown in Figure 3, where an area of MEC with classic features of cystic change and squamous differentiation, and no follicular features, was seen next to an area of typical follicular cytological features and architecture. An intervening area of transition is noted where both follicles including some goblet cells and squamoid differentiation were seen.
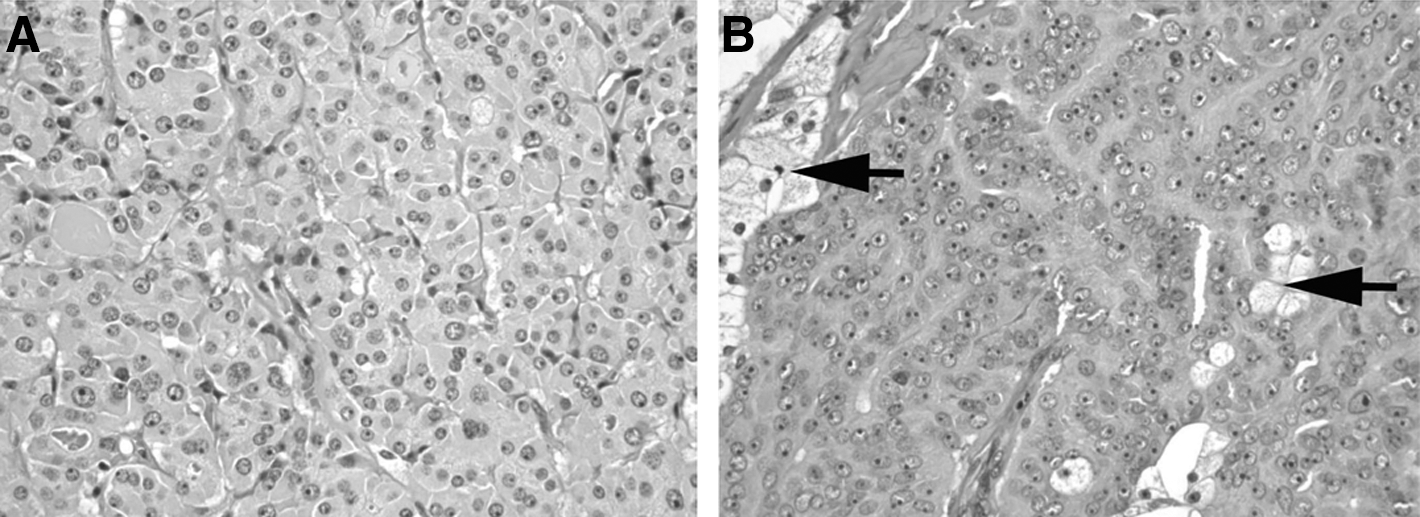
The immunohistochemistry for all cases showed that TTF-1 and thyroglobulin were positive in the areas of WDTC with a gradual transition to complete loss of staining in the MEC areas (Fig. 1). Figure 5 further illustrates the transition of FTC to MEC with strong positive staining of thyroglobulin in an area of FTC and no staining in an area of MEC. These two areas were separated by a transitional area of weak staining. Calcitonin was uniformly negative. Only the MEC component stained positive for CEA.
Gradual transition between typical follicular carcinoma component (arrowheads) that shows diffuse strong positive staining for thyroglobulin and mucoepidermoid component (arrows) which shows completely negative staining for thyroglobulin. At the transition zone between the two, there are areas that show focal/weak staining [thyroglobulin IHC, original magnifications
Discussion
MEC is rare, constituting <0.5% of all thyroid malignancies. Typically, there is a bimodal age distribution with affected women outnumbering men (2:1) (7). The underlying risk factors remain unclear; however, there have been two reported cases found in association with childhood irradiation, and they appear to occur more commonly in association with Hashimoto's thyroiditis (7,8,10). It most commonly presents as a painless neck mass. Patients are euthyroid, and the tumor is usually cold on radio-iodine scan (1 –5,11 –17). Preoperative diagnosis with FNA is unusual. The mainstay of treatment is surgical excision. A total thyroidectomy remains the gold standard, but reports of successful treatment with more limited resections, such as a hemithyroidectomy, can be found within the published literature (15). Although nodal metastatic disease does occur, there is no evidence to suggest that prophylactic central lymph node dissection is beneficial in these patients (13). MEC usually does not take up radioactive iodine, and adjuvant therapy is largely confined to external beam radiotherapy. There does not appear to be a role for adjuvant chemotherapy (15). The prognosis is worse than WDTC, and death due to tumor may occur in up to 20% of individuals, sometimes after transformation to anaplastic carcinoma (7,11,12).
Controversy has surrounded the histogenesis of MEC of the thyroid. Initially, Rhatigan proposed that MEC might arise from salivary gland rests, but evidence for this has been consistently lacking and as such has since been largely disregarded (1). Subsequently, it was suggested that these tumors arose from remnants of the ultimobranchial apparatus, namely the SCN derived from the fourth branchial pouch (2,20). This was as a result of the many shared histological, histochemical, and immunological features between SCN and MEC. However, with increasing use of immunohistochemical markers, such as TTF-1, PAX8, and calcitonin, there is mounting evidence to suggest that MEC does not derive from the ultimobranchial apparatus (17).
More recent debate centered on whether MEC arises from thyroglossal duct remnants or metaplasia of benign or malignant thyroid follicular cells. Derivation from the thyroglossal duct was proposed because of the presence of mucin and sometimes ciliated epithelial within this tumor. However, neither the presence of mucosubstances nor ciliated epithelium is exclusive to the thyroglossal duct and can be found in both remnants of the ultimobranchial apparatus and lesions of follicular epithelial cell origin (21,22). Second, if these tumors were truly to have arisen from the thyroglossal duct, one could reasonably expect that they would be located within the isthmus of the gland. Although there are some reported cases of this occurring, they are in the minority. Indeed, in our series, no tumor arose in the isthmus and, therefore, we consider this an unlikely hypothesis.
Since Hashimoto's thyroiditis is commonly associated with squamous metaplasia, it has been proposed that MEC may arise from this benign but metaplastic squamous epithelium (7). Since none of our three cases were associated with lymphocytic thyroiditis, we have demonstrated that Hashimoto's thyroiditis is certainly not a prerequisite for the development of MEC, and we consider that the frequent occurrence of PTC in Hashimoto's thyroiditis explains the apparent association of MEC and thyroiditis.
The immunohistochemical staining patterns of these cases support the notion that MEC arises from WDTC. In the H&E sections of all three of our cases, there was a gradual transition from typical areas of WDTC to MEC, and this was accompanied by a gradual loss of the thyroid-specific immunohistochemical markers TTF-1 and thyroglobulin.
With these clinical, histological, and immunohistochemical findings, we, therefore, postulate that most cases of MEC of the thyroid arise from metaplastic de-differentiation of WDTC rather than directly from benign squamous metaplasia, salivary gland rests, SCN, or thyroglossal duct remnants. Interestingly, in two of the three cases, despite the MEC component being much smaller than the WDTC, the nodal metastases that occurred showed pure MEC differentiation. This demonstrates the increased aggressiveness of MEC when compared with WDTC. Over time, areas of MEC differentiation may overwhelm and replace areas of WDTC, which might have been unrecognized in the past.
Conclusion
In conclusion, we present the first case series which demonstrates that MEC can arise from FTC and HCC as well as PTC, and provide compelling evidence that MEC usually arises from de-differentiation of pre-existing WDTC rather than directly from benign components of the thyroid gland. Since metastatic disease from the salivary gland to the thyroid or to a thyroid tumor is possible, we recommend that individuals with thyroid MEC undergo a comprehensive examination of the aerodigestive tract to exclude a salivary gland primary unless there is clear cut histological evidence of this progressive de-differentiation from WDTC. Since MEC is usually resistant to radioiodine and is more aggressive than WDTC, this unique variant of thyroid carcinoma is important to be recognized. In the absence of evidence-based guidelines, we believe that our approach of offering adjuvant therapy for both the WDTC and MEC components of these tumors with radioiodine and external beam radiotherapy, respectively, is a logical one.
Footnotes
Disclosure Statement
The authors have nothing to disclose.